

Abstract
Objective. Prior studies investigating the efficacy of oral treprostinil to treat digital ulcers (DU) in systemic sclerosis (SSc)-associated Raynaud phenomenon have yielded conflicting results. In this investigation, we examined whether DU burden increased after patients withdrew from oral treprostinil that was administered during an open-label extension study.
Methods. A multicenter, retrospective study was conducted to determine DU burden in the year after withdrawal from oral treprostinil. DU burden 3–6 months (Time A) and > 6–12 months (Time B) after drug withdrawal was compared with DU burden at baseline, defined as the last day receiving drug in the open-label extension study, by a paired Student t test. Changes in DU burden while receiving drug in the open-label study were compared with changes in DU burden at Time B by a paired Student t test.
Results. Fifty-one patients from 9 clinical sites were included for analysis. DU burden increased significantly from baseline (mean 0.47) to Time A (mean 2.1, p = 0.002, n = 23) and Time B (mean 1.45, p = 0.013, n = 30). Total DU burden decreased during oral treprostinil exposure (mean change −0.6) and then increased by Time B (mean change 1.05, p = 0.0027 for comparison, n = 30). In the year after drug withdrawal, many patients required vasodilator therapy and pain medications. Three patients were hospitalized for complications from DU, and 4 patients required surgery for DU.
Conclusion. Total DU burden increased significantly after discontinuation of oral treprostinil. These data provide supportive evidence of a beneficial effect of oral treprostinil for the vascular complications of SSc and suggest that further study is warranted.
Systemic sclerosis (SSc)-associated Raynaud phenomenon (RP) is characterized by episodic cold and stress-induced vasoconstriction of small arteries associated with a small vessel obliterative vasculopathy. Ischemic digital ulcers (DU) are a frequent complication, estimated to occur in over 40% of patients with SSc1. DU are painful, slow to heal, can be complicated by secondary infection, and may result in major morbidity including digital amputation. In the United States, there are no therapies for RP with or without digital ulcerations that are approved by the US Food and Drug Administration (FDA), and the current standard treatment with calcium channel blockers often proves inadequate for patients with severe disease2. Patients with active DU often try phosphodiesterase (PDE) 5 inhibitors, endothelin receptor antagonists, prostacyclin analogs, botulinum toxin injections, and sympathectomies. Intravenous prostacyclin therapy has been demonstrated to maximize perfusion and healing in patients with active DU in multiple clinical trials3,4,5,6, yet its complex delivery method often limits its administration outside major medical centers.
Treprostinil diolamine (oral treprostinil) is a newer prostacyclin analog that has been developed for oral delivery as an extended release osmotic tablet. It was approved by the FDA for the World Health Organization Group I pulmonary arterial hypertension (PAH) to improve exercise capacity. Severe RP resulting in digital ulceration has been studied as another potential indication. In a phase I pharmacokinetic and pharmacodynamic study examining oral treprostinil in patients with SSc with active or recent DU, cutaneous perfusion and temperature improved with short-term treatment7. A larger, randomized, double-blind, placebo-controlled clinical trial of oral treprostinil was subsequently conducted in patients with SSc with DU (DISTOL-1 trial, ClinicalTrials.gov identifier NCT00775463). While this trial did not meet the desired endpoint (change in net ulcer burden at 20 weeks), there was a significant improvement in several secondary endpoints that measured RP severity8. In addition, patients who enrolled into an open-label extension study (DISTOL-EXT, ClinicalTrials.gov identifier NCT00848107) after the clinical trial developed fewer DU, suggesting a clinical benefit (unpublished data). After termination of the extension study, all participants were withdrawn from oral treprostinil. Therefore, in our investigation, we examined clinical outcomes in these patients in the year after discontinuation of oral treprostinil. We specifically investigated whether DU burden increased after withdrawal of oral treprostinil.
MATERIALS AND METHODS
In our multicenter, retrospective study, medical records were reviewed for the year after discontinuation of oral, twice-daily treprostinil. Data from routine clinical visits were abstracted into a template designed a priori to identify information on the number of active and indeterminate DU at the end of the extension study and at visits subsequent to drug withdrawal. Participants who did not have a subsequent clinical visit with documentation of ulcer status were excluded from our study. When available, additional data were collected from each clinical visit on the use of calcium channel blockers, PDE5 inhibitors, and general pain or narcotic medication use for DU pain. Hospitalizations and surgeries required to treat DU were also recorded.
Data on active, indeterminate, and total DU burden at the start of the randomized clinical trial (DISTOL-1 or TDE-DU-201) and the start of the extension study (DISTOL-EXT or TDE-DU-202) were also obtained from the study sponsor, United Therapeutics Corp. For these studies, a DU was defined as “an area with visually discernable depth and a loss of continuity of epithelial coverage, which could be denuded or covered by a scab or necrotic tissue”9. If denudation was not clearly visible, the investigator determined whether there was loss of epithelialization, epidermis, and dermis. If the area was denuded, the ulcer was classified as “active”. If denudation could not be judged because of the presence of a scab or necrotic tissue, the ulcer was classified as “indeterminate”. Only DU distal to the proximal interphalangeal joints, volar to the equator of the finger, and not localized to the proximal and distal interphalangeal creases were classified, because these were most likely to be vascular in origin. DU related to calcinosis were not included. Total DU burden was the sum of active and indeterminate ulcers.
Data on baseline characteristics, including age, sex, race, SSc subtype, autoantibody status, SSc disease duration, treprostinil dose, and oral treprostinil treatment duration in the extension study, were also obtained from the study sponsor.
This investigation was approved by each participating institution’s review board (IRB). Each IRB determined whether a waiver of consent (given prior patient consent for the DISTOL-1 and DISTOL-EXT studies) was permitted or whether new patient consent was required. Each investigator followed the protocol required by his/her IRB.
Statistical analysis
The number of new DU that developed from the end of the extension study (hereafter referred to as “baseline”) through the first year after discontinuation of oral treprostinil was examined. The number of active, indeterminate, and total DU 3–6 months (Time A) and > 6–12 months (Time B) after discontinuation of oral treprostinil were compared with baseline by a paired Student t test. If more than 1 visit occurred during a given time interval, the ulcer data were averaged across visits. Secondary descriptive outcomes were analyzed, including use of other vasodilator therapy or pain medications, hospitalization attributed to DU, and surgical intervention for digital ulcerations.
Changes in DU burden over 2 time intervals were also examined: (1) during the time patients were receiving oral treprostinil (i.e., while in the extension study), and (2) after withdrawal from oral treprostinil through the > 6–12–month timepoint. The changes in active, indeterminate, and total DU burden over these 2 time periods were compared using a paired Student t test. In addition, we examined whether the changes in DU burden over these 2 time intervals differed by SSc subtype [limited cutaneous (lcSSc) or diffuse cutaneous (dcSSc)] and anticentromere status, given prior data suggesting that oral treprostinil had greater benefit in patients who were anticentromere antibody-negative8. Because of the small numbers of patients with dcSSc included in our study, only descriptive statistics were examined.
Last, total DU burden over time was graphically examined, including data at the beginning of the randomized clinical trial (DISTOL-1 or 201), the start and end of the extension study (DISTOL-EXT or 202), and 3–6 months and > 6–12 months post-withdrawal of oral treprostinil. A spline interpolation method was used to generate individual patient trajectories of total DU burden for ease of review and comparison. However, because patients were in the extension phase of the study (therefore receiving open-label drug) for variable durations, we were concerned that any findings could be secondary to a seasonal confounding effect alone. In addition, it is important to note that most patients withdrew from the extension phase of the study during the summer of 2011. To address the effect of season, we performed paired Student t tests comparing the number of total DU while receiving the drug in January 2011 ± 3 months to total DU burden while not receiving the drug in January 2012 ± 3 months.
Statistical analyses were performed using Stata version 13.0 and SAS version 9.2.
RESULTS
Nine SSc centers in the United States participated in our retrospective study. There were 57 patients from these centers who participated in the open-label extension study, and 51 of these patients had followup data after drug withdrawal and met our inclusion criteria. The mean age at the end of the open-label extension study was 53.8 years (SD 11.9), and 80.4% of the patients were women (Table 1). The majority (84.3%) of patients had lcSSc, and the mean SSc disease duration upon exit of the open-label extension study was 12.3 years (SD 9.1). The mean oral treprostinil dose was 5.7 mg/day (SD 3.87), and patients were treated for a mean of 340 days (SD 120.5) in the open-label extension study.
Baseline characteristics of study patients (n = 51). Values are mean (SD) unless otherwise specified.
DU burden, medication use, and complications in the year after treprostinil discontinuation
At the conclusion of the treprostinil extension study, the mean number of active, indeterminate, and total DU was 0.25 (SD 0.63), 0.22 (SD 0.54), and 0.47 (SD 0.78), respectively (Table 2). Information on DU status was available for 23 patients at Time A (3–6 mos after discontinuation of oral treprostinil) and 30 patients for Time B (> 6–12 mos after discontinuation of oral treprostinil). The mean number of active DU increased from baseline to Time A (mean 1.62, p = 0.004, n = 23) and Time B (mean 1.03, p = 0.076, n = 30), although the change from baseline to Time B did not reach statistical significance. The mean number of indeterminate DU increased significantly from baseline to Time B (mean 0.42, p = 0.030, n = 30), but the change from baseline to Time A did not reach statistical significance (mean 0.48, p = 0.357, n = 23). The mean total DU burden increased significantly from baseline to Time A (mean 2.1, p = 0.002, n = 23) and Time B (mean 1.45, p = 0.013, n = 30). After withdrawal from oral treprostinil, the majority of patients required intensive vasodilator therapy and pain medications. While no patients were taking PDE5 inhibitors during the open-label extension study when receiving oral treprostinil, 21.6% of patients had to start a PDE5 inhibitor after drug withdrawal. The majority of patients continued their calcium channel blockers (60.8% after drug withdrawal vs 56.9% before drug withdrawal). An additional 10% of patients had to add some type of pain medication (58.8% after drug withdrawal vs 47.1% before drug withdrawal), while the percentage requiring opioids did not change (33.3% both before and after drug withdrawal). Three patients were hospitalized after withdrawal from oral treprostinil for complications from DU: one for debridement of a non-healing, infected ulcer and need for intravenous antibiotics, another for a toe amputation, and another for uncontrolled pain. Two additional patients required outpatient surgical interventions, including debridement or drainage of wounds after withdrawal from oral treprostinil. One other patient had documented antibiotic use for a DU after withdrawal from oral treprostinil. While receiving oral treprostinil, 2/51 patients were diagnosed with exercised-induced pulmonary hypertension and 1/51 with PAH; after withdrawal from oral treprostinil, 5/51 patients were diagnosed with pulmonary hypertension. No deaths were reported during the clinical trial, and 1/115 patients died during the extension study from cardiac arrest. During the year following withdrawal from oral treprostinil, 4/51 patients died: 2 because of cardiac arrest, 1 from progression of interstitial lung disease and PAH, and 1 from an antineutrophil cytoplasmic antibody-associated vasculitis.
Active, indeterminate, and total DU burden in the year after treprostinil withdrawal. Values are mean (SD) unless otherwise specified.
Comparison of changes in DU burden while receiving treprostinil versus after treprostinil discontinuation
Further analyses were performed to compare changes in DU burden during the time patients were receiving oral treprostinil (during the open-label extension study) with the time after withdrawal of oral treprostinil (Time B, > 6–12 mos; Table 3). Complete data from the open-label extension study and from baseline and Time B were available for 30 patients. On average, active, indeterminate, and total DU burden decreased while receiving the drug and increased while withdrawn from the drug; these changes were statistically significantly different for indeterminate and total DU, and of borderline statistical significance for active DU. The mean change in active DU burden was −0.17 (SD 0.65) while receiving oral treprostinil and 0.7 (SD 2.09) after withdrawal from oral treprostinil (p = 0.0509). The mean change in indeterminate DU burden was −0.43 (SD 0.82) during the extension study and 0.35 (SD 0.84) after oral treprostinil withdrawal (p = 0.0009), and similarly the mean change in total DU burden was −0.6 (SD 1.04) while receiving the drug and 1.05 (SD 2.16) after drug discontinuation (p = 0.0027).
Change in DU burden during open-label treprostinil exposure and after treprostinil withdrawal (n = 30).
Whether the changes in total DU burden over these 2 time windows differed by SSc cutaneous subtype (dcSSc vs lcSSc) was of interest. However, only 8 of the 51 patients in our study had dcSSc, and out of the 30 patients with data from Time B, 4 patients had dcSSc. Given the small sample size of patients with diffuse disease, paired Student t tests were not performed and descriptive statistics were tabulated (Appendix 1). During the open-label extension study (receiving drug), patients with diffuse disease had a larger decrease in total DU burden (mean change −1.75) than patients with limited disease (mean change −0.42). When examining the change in total DU burden after drug withdrawal, patients with diffuse disease had a greater increase in total DU burden than patients with limited disease (mean change 3.5 diffuse vs 0.67 limited). A similar pattern was observed when examining median (rather than mean) changes in total DU burden (Appendix 1). These findings were compatible with our analyses by anticentromere status. We calculated the change in total DU burden during the extension study (while patients received oral treprostinil) and compared this with the change in total DU burden after drug withdrawal (change from end of extension study to Time B) in anticentromere-positive patients, and repeated this analysis for anticentromere-negative patients. Among anticentromere-positive patients, there were no statistically significant differences in the change in total DU burden comparing these 2 timepoints (p = 0.0606, n = 14 with paired data). There were 13 patients who were negative for anticentromere antibodies with paired data, and this comparison was statistically significantly different (p = 0.0195). These data suggest that anticentromere-negative patients may have worsened to a greater extent while not receiving oral treprostinil than anticentromere-positive patients.
Trajectory of DU burden over time
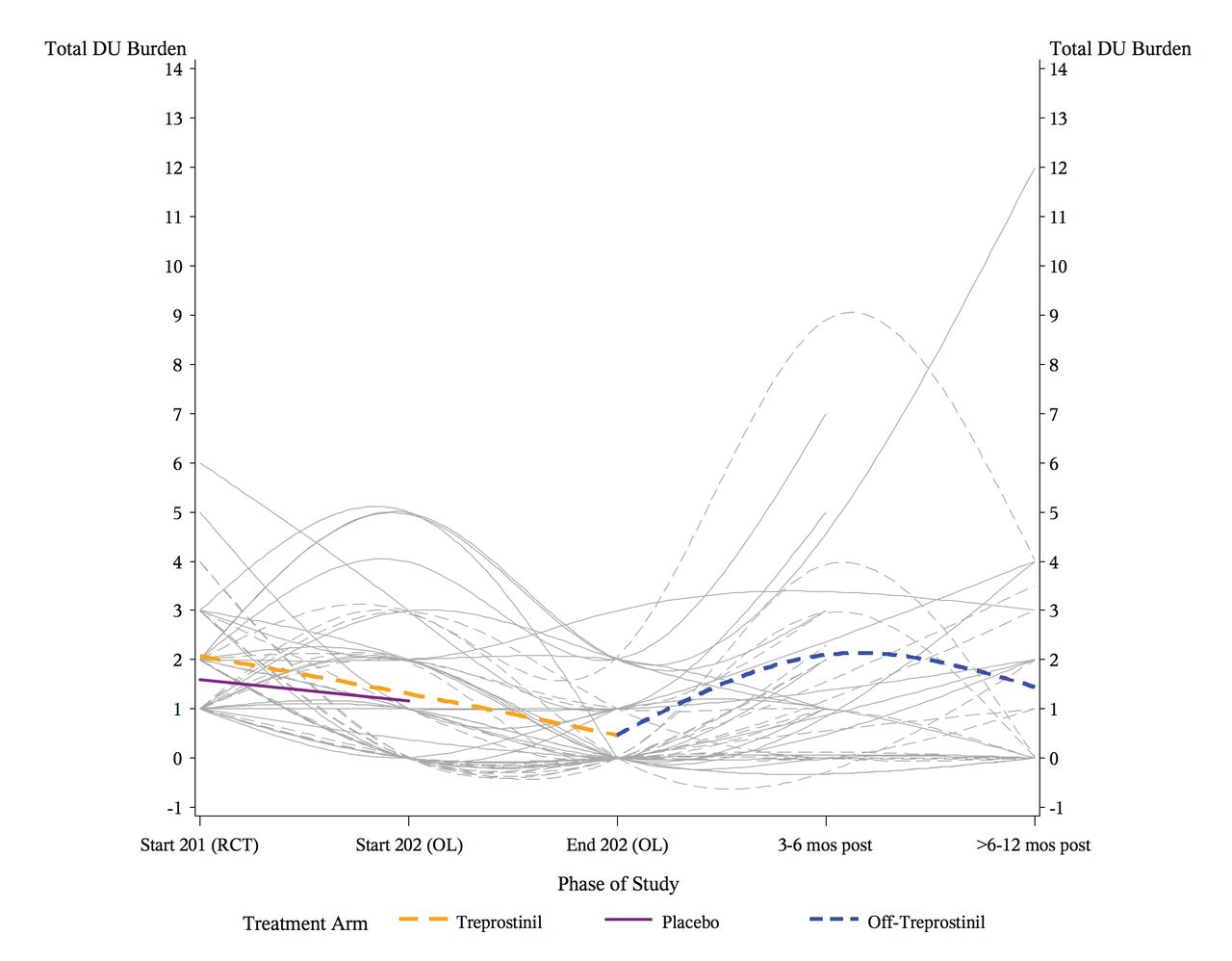
To better understand the trajectory of DU burden, we tabulated active, indeterminate, and total DU burden throughout the oral treprostinil studies and at the 2 timepoints post-withdrawal of oral treprostinil (Table 4). Individual patient level data were also plotted over time, from the initiation of the randomized clinical trial through the year after withdrawal from the open-label extension study (Figure 1). Overall, we see that total DU burden declined while patients were receiving oral treprostinil and increased again after withdrawal of the drug. However, the individual patient trajectories suggested that there was (1) a subset of patients who were responsive to oral treprostinil and then demonstrated increased digital ulceration after drug discontinuation, and (2) a subset of patients who were remarkably stable with little or no DU burden over time whether receiving or not receiving the drug. We examined whether these individual trajectories could be a reflection of the cumulative treprostinil dosage exposure, but we were unable to identify any distinct patterns (data not shown).

Total DU burden throughout the DU burden studies. The Y-axis reflects total DU burden and the X-axis reflects time. The start of the 201 study is the beginning of the RCT, and the start of the 202 study is the beginning of the OL extension. The end of the 202 study is the end of the OL extension and forms the baseline visit for our current study. Data are also identified 3–6 mos (Time A) and > 6–12 mos (Time B) post-treprostinil withdrawal. The grey lines reflect each patient’s individual trajectory. Those with dashed lines were initially randomized to oral treprostinil during the RCT, whereas those with solid lines were initially randomized to placebo. During the 201 phase, the orange dashed line and the purple solid line reflect the mean total DU burden over time for patients initially randomized to treprostinil or placebo, respectively. During the 202 phase, the orange dashed line reflects the mean total DU burden when patients were taking treprostinil during the OL extension. After the end of 202, the blue dashed line denotes the mean total DU burden after discontinuing oral treprostinil. DU: digital ulcers; RCT: randomized controlled trial; OL: open-label.
DU burden throughout the treprostinil studies.
Because most patients withdrew from the open-label extension study during the summer of 2011, we were also concerned that the changes observed could be secondary to seasonal effects. The total DU burden closest to January 15, 2011 (± 3 mos), was compared with the total DU burden closest to January 15, 2012 (± 3 mos). Thirty-seven patients had data available for analysis at these 2 timepoints. The mean total DU burden was 0.7 in the winter of 2011 (receiving drug) and 1.92 in the winter of 2012 (not receiving drug; p = 0.0006), suggesting that the differences observed were related to drug exposure status rather than seasonal effects.
DISCUSSION
In our multicenter, retrospective study, total DU burden increased significantly after withdrawal from oral treprostinil. Many clinically significant problems attributable to DU also developed, including the need for pain medications, hospitalizations, surgeries, and antibiotic use. Further examination demonstrated that DU burden decreased during the open-label extension study while patients were exposed to oral treprostinil, in contrast to the increase in DU burden in the year after oral treprostinil discontinuation. Importantly, and impressively, these differences persisted after adjustment for seasonal effects. It is important to note that the randomized, placebo-controlled clinical trial of oral treprostinil did not meet its primary outcome of change in net ulcer burden at Week 208. However, our current data, in conjunction with positive trends noted in RP’s secondary outcomes during the clinical trial and the pharmacodynamic data demonstrating improvements in cutaneous perfusion7, suggest that further study is warranted to identify the subset of patients who are most likely to benefit from oral treprostinil therapy based on baseline phenotypic or biomarker characteristics.
Graphical examination of DU burden throughout the oral treprostinil studies and 1 year following oral treprostinil withdrawal suggests that there may be a subset of patients who are particularly responsive to treprostinil, whereas other patients remain stable with little DU burden over time. It is unclear whether patients who were more likely to respond to therapy, or more likely to have a rebound increase in ulcer burden while not receiving the drug, were those who received a higher dosage of oral treprostinil or had a longer duration of oral treprostinil exposure. Descriptive analyses suggest that patients with dcSSc may have greater benefit from treprostinil in treating DU than patients with lcSSc, although there were too few patients for any meaningful statistical analysis. Similarly, the data suggest that patients negative for anticentromere antibodies may benefit more from oral treprostinil than those who are anticentromere-positive.
In addition to the difficulty in ascertaining patient subsets who are most likely to respond to vasodilator therapy for DU, this series of studies examining the role of oral treprostinil in the therapy of DU illustrates many of the challenges of performing high-quality DU studies. Investigators may variably define whether a DU is present, and if a DU is active, indeterminate, or healed, based on their prior clinical experiences10. While DU definitions were prespecified for our study, the assessment remains somewhat subjective and observer-dependent. Further, changes in RP activity and DU burden may be influenced by seasonal changes or changes in other vasodilator medications that occur during an investigation. The optimal duration of followup to assess ulcer healing is also unknown.
We recognize that our study does not prove the efficacy of oral treprostinil for SSc-associated DU given that investigators were not blinded to drug status during the open-label extension study or clinical visits during the period after drug withdrawal. Data were obtained from retrospective review of visits for routine clinical care, and as a result, data were not available on all 51 patients at both timepoints of interest. Patients with more severe manifestations of RP could be more likely to present for followup evaluation, potentially biasing our study results. In addition, DU may not be recorded in the same manner or with the exact same definitions during a study as during routine clinical visits. Our sample size includes 50% of all participants who entered the open-label extension study in the United States, because our investigation was restricted to 9 US sites and subjects for whom followup data were available through routine clinical care. The small sample size in our study limited our ability to investigate dose or clinical phenotypic effects on DU burden, and the lack of a comparator group may affect the generalizability of these findings.
These data provide supportive evidence of a beneficial effect of oral treprostinil for the vascular complications of SSc, and suggest that further study of this medication for RP and DU is warranted.
Acknowledgment
The authors thank Emily Semmel, Cynthia Anderson, and Donald Rodriguez for their assistance in abstracting data from medical chart review.
APPENDIX 1.
Change in total digital ulcer burden during open-label treprostinil exposure and after treprostinil withdrawal by systemic sclerosis subtype.
Footnotes
This investigator-initiated study was funded by a research grant from United Therapeutics Corp. RM and JC are employees of United Therapeutics Corp.
- Accepted for publication May 19, 2016.








{kind=link}