

Abstract
Objective. We sought to identify specific microRNA (miRNA) for systemic juvenile idiopathic arthritis (sJIA) and to determine the involvement of these miRNA in regulating the expression of cytokines.
Methods. Microarray profiling was performed to identify differentially expressed miRNA in sJIA plasma. Levels of candidate miRNA and mRNA were assessed by real-time PCR, and cytokines were measured by ELISA. Dual-luciferase reporter assay was used to validate the direct interaction between miR-26a and interleukin 6 (IL-6).
Results. Forty-eight miRNA were differentially expressed in the plasma of patients with sJIA compared with healthy controls (HC). Five miRNA were selected for further validation. The expression level of miR-26a was exclusively elevated in the plasma of patients with sJIA as compared with 4 rheumatic diseases and 2 subtypes of JIA (oligoarticular and polyarticular). The levels of IL-6, IL-1β, and tumor necrosis factor-α in the plasma of patients with sJIA were increased, and only IL-6 presented a positive correlation with miR-26a (r = 0.539, p < 0.0001). After stimulation with IL-6, miR-26a expression was upregulated in THP-1 cells, while the supernatant level of IL-6 was downregulated by transfection of miR-26a mimics. Consistently, direct target relationship between miR-26a and IL-6 was confirmed.
Conclusion. This study demonstrates that miR-26a is expressed specifically and highly in sJIA plasma and suggests that miR-26a may regulate the levels of cytokines in sJIA. Our findings highlight miR-26a as a potential biomarker for the diagnosis as well as differential diagnosis of sJIA.
Juvenile idiopathic arthritis (JIA) is the most common rheumatic and chronic disease in children. Among 3 dominated subtypes, including systemic (sJIA), oligoarticular (oJIA), and polyarticular (pJIA), sJIA is differentiated and regarded as an autoinflammatory disease characterized by the absence of autoantibodies and the overproduction of proinflammatory cytokines1. The pathogenesis of sJIA remains poorly understood. At present, the diagnosis of sJIA mostly relies on clinical features and laboratory investigations. However, the clinical heterogeneity and lack of specific diagnostic markers make the early diagnosis of sJIA very difficult. For this reason, searching for highly specific and valid biomarkers to diagnose sJIA at early stages seems particularly urgent and important.
Micro RNA (miRNA) are short, single-stranded, noncoding RNA that posttranscriptionally regulate gene expression through the binding to 3′-untranslated regions (3′-UTR) of target genes2. miRNA are involved in a wide range of crucial biological processes and their dysregulation has been described in different diseases, including cancer and immune disorders3,4. Increasing evidence has demonstrated that circulating miRNA in blood have the potential to serve as biomarkers because of 3 properties: specificity5, stability6, and rapid detection7. In particular, detection of plasma or serum levels of miRNA has the potential for an earlier disease diagnosis and to predict prognosis and response to therapy8. Previous studies have proven that the expression levels of several miRNA are dysregulated in immune cells, inflamed joints, and the peripheral blood of patients with rheumatoid arthritis (RA)9. More recently, abnormal expression of miR-16, miR-132, miR-146a, miR-155, and miR-223 in the plasma of patients with oJIA and pJIA has been reported10.
As stated, sJIA have special clinical features and an inflammatory profile compared with other JIA subtypes. Therefore, we speculated that miRNA profiling might also be different in patients with sJIA. In our study, we aimed to search for special and sensitive circulating miRNA in the plasma of patients with sJIA to investigate the potential value of the miRNA as a kind of biomarker for diagnosis. In addition, we sought to perform a preliminary study to investigate the underlying mechanisms.
MATERIALS AND METHODS
Patient variables
A total of 280 participants were recruited for our study: 105 patients with sJIA (40 sJIA, 40 oJIA, and 25 pJIA), 25 with systemic lupus erythematosus (SLE), 30 with juvenile ankylosing spondylitis (JAS), 40 with Kawasaki disease (KD), 40 with Henoch-Schönlein purpura (HSP), and 40 healthy controls (HC; Table 1). Patients were diagnosed at the Department of Rheumatology and Immunology at the Capital Institute of Pediatrics Hospital from 2012 to 2014. Children having a health check in the Department of Health were included as control subjects. Patients with JIA met the diagnostic criteria of the International League of Associations for Rheumatology11. Patients with JAS, SLE, and KD fulfilled the criteria of the American College of Rheumatology12,13,14. Patients with HSP were diagnosed according to the criteria of the European League Against Rheumatism/Paediatric Rheumatology European Society15. All the enrolled patients had active disease, were newly diagnosed, and were not treated with any kind of nonsteroidal antiinflammatory drug, disease-modifying antirheumatic drug, glucocorticoid, immune-suppressor, or biological agent. Our study was approved by the ethics committee of the Capital Institute of Pediatrics. Written informed consent was obtained from each of the participants and their guardians.
Clinical features and laboratory information of the participants who contributed plasma. Values are n unless otherwise specified.
Plasma preparation
Blood samples from patients were collected directly into EDTA-treated tubes and centrifuged at 2500 g for 4 min at room temperature. Aliquots of the supernatant were transferred into new RNase-free tubes and stored at −80°C.
miRNA microarray assays
Total RNA was extracted using RNeasy mini kits (QIAGEN). RNA quality was assessed with the Agilent Bioanalyzer 2100 (Agilent Technologies). Then 100 ng of miRNA was fluorescently labeled with Cy3 using an miRNA Complete Labeling and Hyb Kit and hybridized on miRNA array. miRNA expression analysis was performed using Agilent human miRNA (8*60K) V16.0 microarrays according to the manufacturer’s protocol (Agilent Technologies). Raw data were normalized by GeneSpring Software 11.0 (Agilent Technologies).
RNA extraction
Total RNA was extracted from 250 μl of plasma using TRIzol LS reagent (Invitrogen) following the protocol for liquid samples. Then 5 μl of 5 nM synthetic Caenorhabditis elegans miRNA (cel-miR-39) was spiked into each denaturing solution to normalize sample-to-sample variation in the processing of RNA extraction. For RNA extraction from cultured cells, transfected cells were harvested and washed 3 times with 1 × phosphate buffered saline (PBS). RNA was extracted using TRIzol (Invitrogen) according to the manufacturer’s instructions. U6 snRNA was used as a quality control for the process of extraction.
Reverse transcription (RT) and quantitative real-time PCR (qRT-PCR)
RT-PCR was performed with miRNA-specific, stem-loop RT primer using the RT System A3500 Kit (Promega). SYBR Green Real-Time PCR assay was carried out on a 7500 Fast Real-Time PCR System (Applied Biosystems). Standard curves were obtained using serial dilutions of synthetic miRNA mimics at known concentrations for absolute quantification. For the quantification of miRNA and mRNA in cultured cells, 1 μg of total RNA was added into an RT reaction. The expression levels of miRNA and mRNA were, respectively, normalized to U6 snRNA and β-actin. Data were analyzed with SDS v2.0.4 using 2−ΔΔt method.
Cell culture and transfection
The human monocytic cell-line THP-1 was purchased from Concorde Cell Bank and cultured in RPMI 1640 (Gibco) with 10% fetal bovine serum. miR-26a mimics, or a scrambled negative control (NC; Invitrogen), were transfected at a final concentration of 40 nM by Lipofectamine RNAiMAX reagent (Invitrogen). After 48 h, THP-1 cells were stimulated with 1 μg/ml of lipopolysaccharide (LPS; Sigma) for 24 h. Cells were harvested for western blotting and qRT-PCR, and culture supernatants were collected for measuring cytokine protein levels.
Luciferase reporter assay
HEK293T cells were seeded in 6-well plates at 5 × 105 per well for 24 h before transfection. Then 750 ng of miR-26a expression plasmid or NC vector were transfected into HEK293T cells simultaneously with 250 ng of wild-type or mutant interleukin 6 (IL-6) 3′UTR-pmirGLO plasmid using lipofectamine 2000 (Invitrogen) according to the manufacturer’s instructions. The luciferase activity was measured using a dual-luciferase Reporter Assay System (Promega) 24 h after transfection and the relative luciferase activity value was achieved against the renilla control.
ELISA
Concentrations of IL-1β, IL-6, and tumor necrosis factor-α (TNF-α) in culture supernatants or sJIA plasma were quantitatively determined by ELISA kits (R&D Systems) following the manufacturer’s instructions.
IL-6 stimulation of THP-1 cells
Before stimulation with LPS, THP-1 cells were cultured in 6-well plates at 1 × 105 per well and stimulated with 100 ng/ml of IL-6 recombinant human protein (Invitrogen) for 48 h. PBS was used as a control in the same volume.
Statistical analysis
Statistical analyses were performed using SPSS 16.0. Comparisons between 2 groups were analyzed by the Student t test. One-way analysis was used to compare variance among more than 2 groups. P values < 0.05 were considered statistically significant. Receiver-operating characteristic (ROC) curves were performed to evaluate the diagnostic performance of miR-26a expression levels of cases and HC. Sensitivity against 100% minus specificity was plotted at each cutoff threshold, and the area under the curves (AUC) was calculated to indicate the probability of correctly identifying patients with sJIA from control subjects. Correlations were analyzed by Pearson correlation.
RESULTS
miRNA expression profiling in the plasma of patients with sJIA
To identify miRNA that were specifically expressed in sJIA, we performed microarray analysis with plasma miRNA from 5 patients with sJIA and 5 age- and sex-matched HC using Agilent Technologies’ human miRNA microarray version 16.0 (Agilent Technologies). After normalization of the raw data, 48 miRNA that were significantly differentially expressed were identified by screening for p values < 0.05 and fold-change > 2. Compared with HC, 29 miRNA were upregulated and 19 were downregulated in patients with sJIA (Figure 1).

Hierarchical clustering analysis of miRNA expression profiles in plasma samples. Expression values were determined by microarray analysis, and miRNA are plotted whose expression differed by 2-fold or more in the sJIA and control samples, with p < 0.05. Columns represent plasma samples and row miRNA. miRNA: microRNA; sJIA: systemic juvenile idiopathic arthritis.
Through bioinformatic analysis, 5 (miR-26a, miR-145, miR-1237, miR-1228, and miR-181a) of the 48 differentially expressed miRNA were selected for further study based on their predicted association with immune and inflammatory responses (data not shown). qRT-PCR was performed to validate the 5 candidate miRNA using an independent set of plasma samples of 20 patients with sJIA and 20 HC. The average expression levels of miR-26a, miR-145, miR-181a, and miR-1228 in plasma samples of patients with sJIA were significantly higher than those of HC, while miR-1237 expression was remarkably lower in patients with sJIA compared with HC. Except for miR-1228, expression patterns of the other 4 miRNA were consistent with the microarray data.
miR-26a expressed differentially and specifically in sJIA
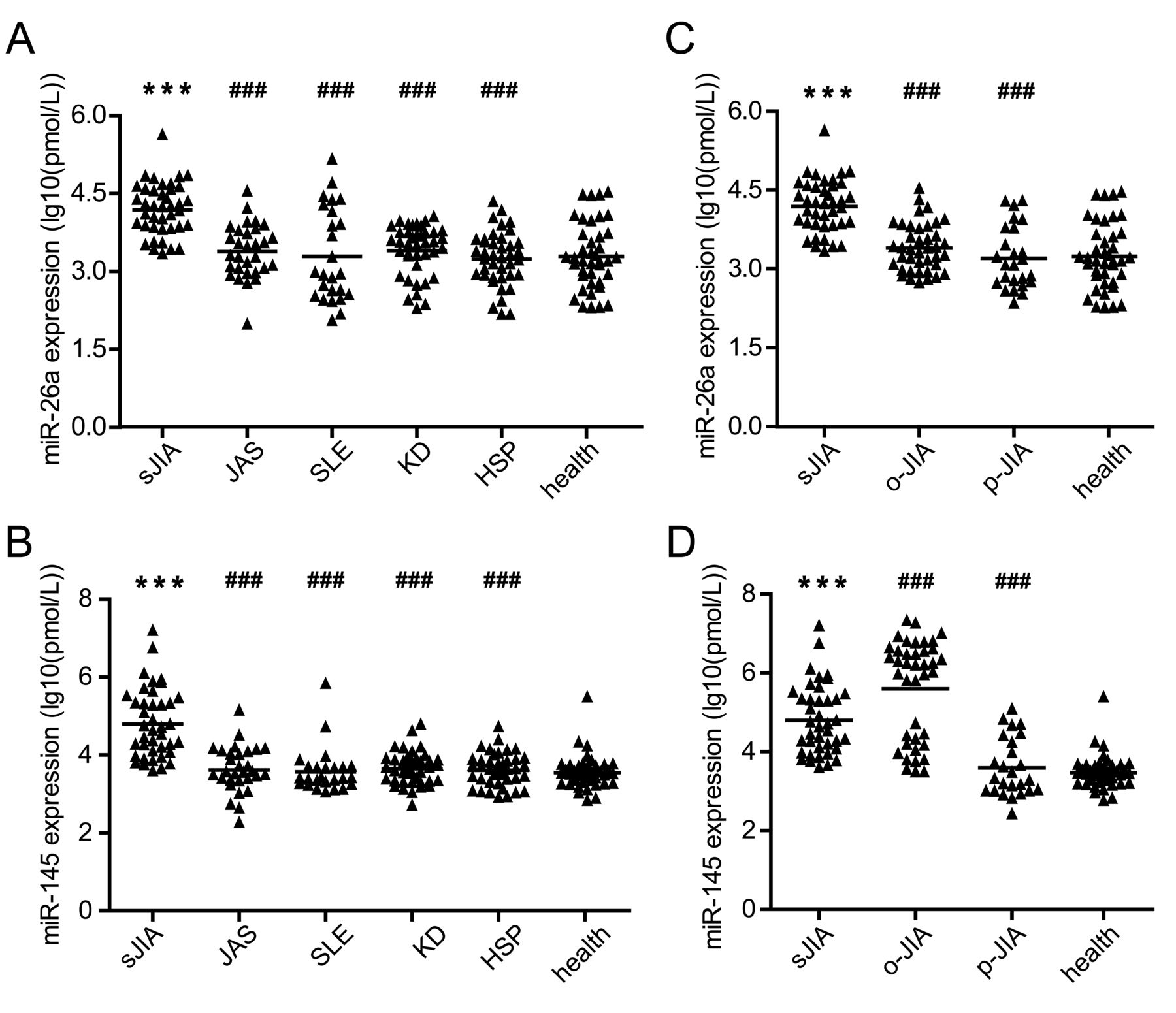
To determine whether the levels of the 5 miRNA can distinguish sJIA from other rheumatic diseases, we compared the same cohort of 20 patients with sJIA with the patients with JAS, SLE, KD, and HSP. Notably, the expression levels of miR-26a and miR-145 were dramatically elevated in sJIA (data not shown), but miR-181a, miR-1228, and miR-1237 showed irregular expression patterns in the 4 rheumatic diseases, suggesting their expression is JIA nonspecific. Based on the results, an expanded set of plasma samples was enrolled to further validate the specificity of miR-26a and miR-145 in sJIA. With the integration of the 2 experimental data derived from the total of 215 subjects, it could be concluded that miR-26a and miR-145 were differentially expressed specifically for sJIA (Figures 2A and 2B).

The expression of miR-26a was specially upregulated in sJIA. (A–B) The levels of miR-26a and miR-145 in the plasma from patients with sJIA (n = 40) and HC (n = 40) were compared to the levels in plasma from patients with JAS (n = 30), SLE (n = 25), KD (n = 40), and HSP (n = 40). (C–D) The levels of miR-26a and miR-145 in plasma from patients with sJIA (n = 40) and HC (n = 40) were compared to the levels in the plasma from patients with oJIA (n = 40) and pJIA (n = 25). ### p < 0.001 compared with sJIA. *** p < 0.001 compared with HC. JIA: juvenile idiopathic arthritis; sJIA: systemic JIA; HC: healthy controls; JAS: juvenile ankylosing spondylitis; SLE: systemic lupus erythematosus; KD: Kawasaki disease; HSP: Henoch-Schönlein purpura; oJIA: oligoarticular JIA; pJIA: polyarticular JIA.
To evaluate whether miR-26a and miR-145 can differentiate JIA subtypes, we examined plasma samples from 40 patients with oJIA and 25 patients with pJIA by qRT-PCR. It was interesting that the expression levels of miR-26a for the oJIA and pJIA subtypes were both less than those for sJIA. In addition, neither oJIA nor pJIA showed obvious differences with HC (Figure 2C). For miR-145, though its expression levels were significantly higher in oJIA and lower in pJIA as compared with sJIA, there was no remarkable difference between pJIA and HC (Figure 2D). These results suggested that only miR-26a expressed differentially and specifically in sJIA.
Assessment of the diagnostic and discriminatory value of miR-26a for sJIA
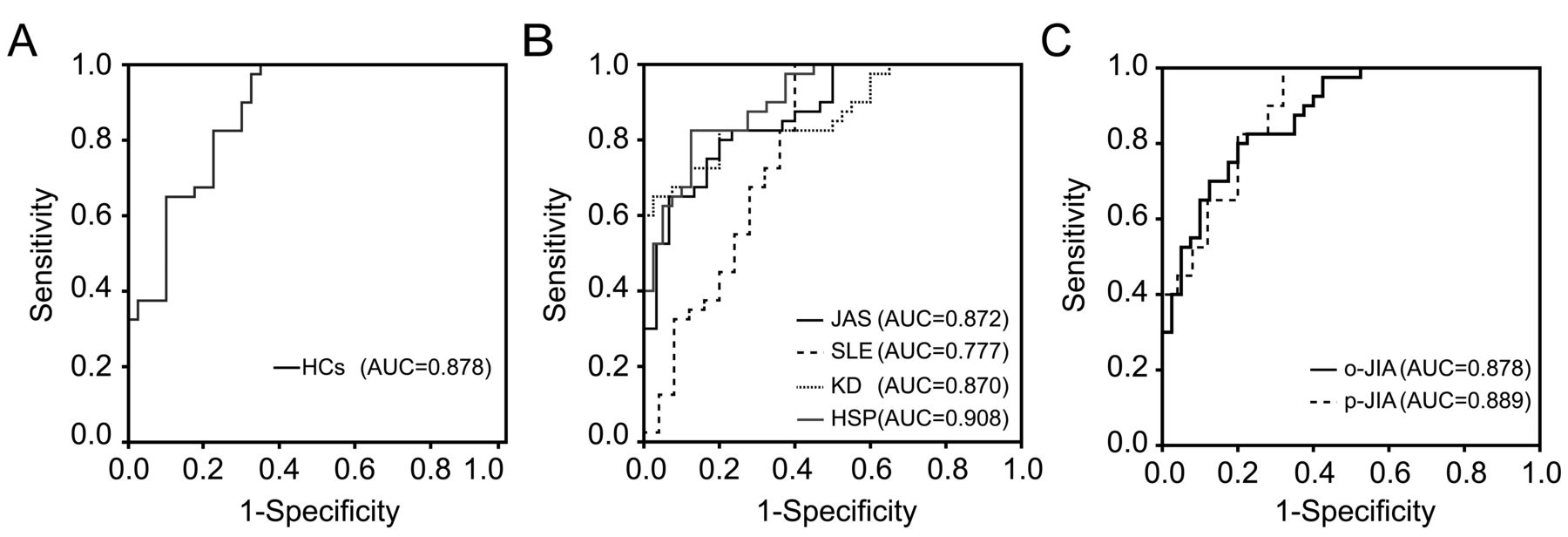
To assess the diagnostic and discriminatory value of miR-26a for sJIA, we used ROC curve analysis. The ROC curves of miR-26a reflected that plasma miR-26a levels were robust in separating patients with sJIA from HC subjects with an AUC of 0.878 (95% CI 0.803–0.952; Figure 3A). miR-26a was also effective in discriminating sJIA from rheumatic disease controls: the AUC was 0.872 (95% CI 0.791–0.953) for JAS, 0.870 (95% CI 0.793–0.947) for KD, and 0.908 (95% CI 0.846–0.969) for HSP. However, miR-26 displayed worse performance in discriminating sJIA from SLE, with an AUC of 0.777 (95% CI 0.647–0.907; Figure 3B). We did the same analysis for JIA subtypes. The AUC were determined to be 0.878 (95% CI 0.805–0.950) for oJIA and 0.889 (95% CI 0.806–0.972) for pJIA (Figure 3C). Collectively, these results indicated that miR-26a represented a potential utility biomarker for sJIA.
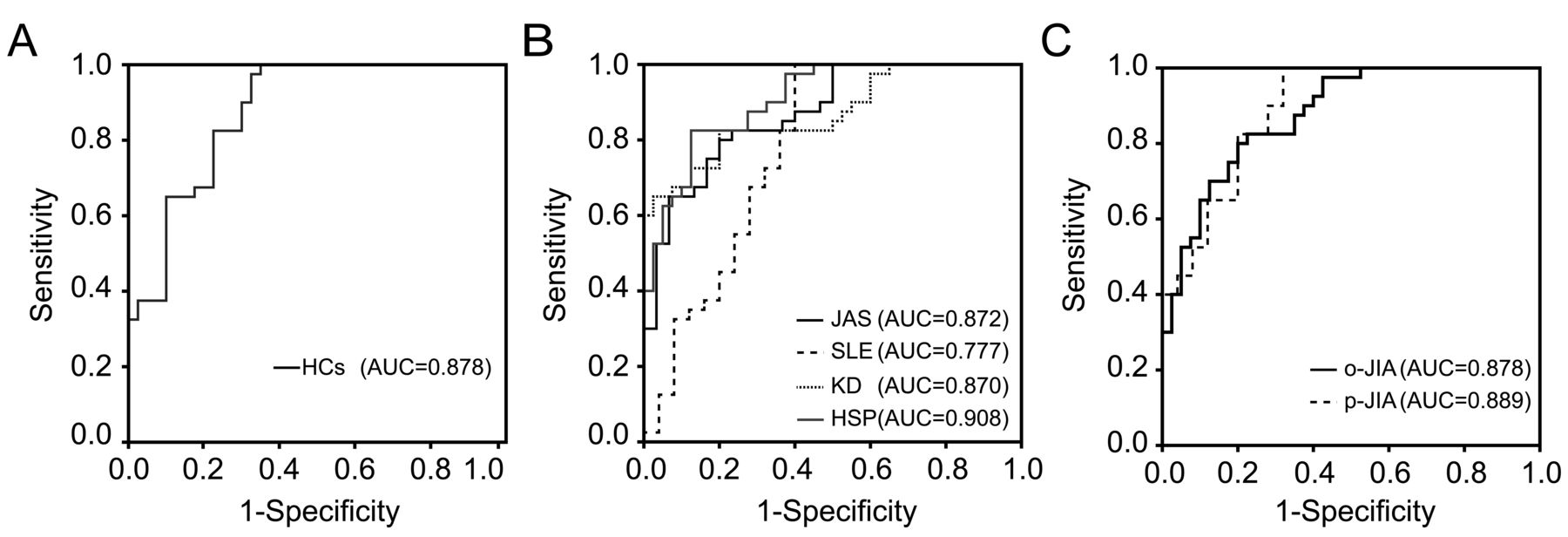
ROC analysis of the diagnostic and discriminating value of miR-26 for sJIA. A. ROC analysis of the ability of miR-26a to distinguish patients with sJIA from HC. B. ROC analysis of the ability of miR-26a to distinguish 4 rheumatic diseases from sJIA. C. ROC analysis of the ability of miR-26 to distinguish sJIA from oJIA and pJIA. ROC: receiver-operating characteristic; JIA: juvenile idiopathic arthritis; sJIA: systemic JIA; HC: healthy controls; oJIA: oligoarticular JIA; pJIA: polyarticular JIA; AUC: area under the curve; JAS: juvenile ankylosing spondylitis; SLE: systemic lupus erythematosus; KD: Kawasaki disease; HSP: Henoch-Schönlein purpura.
Effect of miR-26a on cytokines levels in innate immune response
To get an insight into whether plasma miR-26a expression was correlated with the clinical and laboratory variables of patients with sJIA, we carried out Pearson correlation analysis. Interestingly, there was no obvious correlation of miR-26a expression with common clinical and laboratory features, such as tender or swollen joint count, erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP; all at p > 0.05). Several studies have demonstrated that the overproduction of proinflammatory cytokines, including IL-1β, IL-6, and TNF-α, contributed to the multisystem inflammation of sJIA. Our results also indicated that the levels of IL-1β, IL-6, and TNF-α in the plasma of patients with sJIA were increased. After examining the correlations between miR-26a with IL-1β, IL-6, and TNF-α levels, a median positive correlation between the levels of miR-26a and IL-6 in plasma was observed (r = 0.539, p < 0.0001; Figure 4A).

The effect of miR-26a on IL-6. A. Positive correlation between miR-26a and IL-6 plasma levels in sJIA. B. miR-26a expression in THP-1 cells stimulated with IL-6. * p < 0.05. C. Levels of IL-6 in the supernatants of posttransfected THP-1 cells and effects of miR-26a mimics on the expression of IL-6 mRNA. D. Sequence alignment of miR-26a with putative binding sites within the wild-type and mutant 3′-untranslated regions of IL-6. E. The relative luciferase activity transfected with wild-type or mutant IL-6 promoter/luciferase reporter. IL-6: interleukin 6; sJIA: systemic juvenile idiopathic arthritis; WT: wild-type; UTR: untranslated regions.
To directly determine the effect of IL-6 on miR-26a expression, we treated THP-1 cells with IL-6 for 48 h and examined miR-26a levels after an additional 24-h treatment with LPS. As shown in Figure 4B, levels of miR-26a were elevated by IL-6 treatment, possibly explaining the positive correlation of IL-6 and miR-26a in sJIA.
Previous studies suggested that miR-26a may function as an antiinflammatory factor16,17, implying that the increased levels of miR-26a induced by excessive IL-6 in sJIA could in turn repress the expression of IL-6 through a negative-feedback regulatory loop. To identify the hypothesis, we transfected miR-26a mimics into THP-1 cells and detected the levels of IL-6 in cell culture supernatants by ELISA. Indeed, the secreted IL-6 levels were decreased in the miR-26a mimics group compared with the control group. Meanwhile, IL-6 mRNA expression was also significantly suppressed after miR-26a mimics transfection (Figure 4C). All the results supported that miR-26a negatively regulated IL-6 expression in THP-1 cells. Bioinformatics analysis showed that miR-26a was a candidate miRNA for targeting IL-6 mRNA 3′-UTR (Figure 4D). To confirm whether IL-6 was the target of miR-26a, we performed luciferase reporter assays in HEK293 cells. Transfecting miR-26a mimics and pmirGLO-IL-6 vector could lead to a significant reduction (p < 0.05) of luciferase activity compared with the NC mimics (Figure 4E). On the contrary, transfecting miR-26a mimics together with a mutated pmirGLO-IL-6 vector failed to regulate the luciferase activity, suggesting that miR-26a directly targeted IL-6 mRNA to exert its inhibitory effects on IL-6 expression.
These results indicated the preliminary mechanism of miR-26a in the progress of sJIA. Because of the overproduction of cytokines, miR-26a was upregulated in sJIA, most potentially through signaling pathways mediated by IL-6.
DISCUSSION
The diagnosis of sJIA has been a great challenge because of the lack of specific and sensitive diagnostic markers. Several conventional clinical and laboratory variables, such as white blood cell count, ESR, CRP, serum interleukins levels, thrombocytosis, and anemia also change in multiple inflammatory and self-limited diseases18,19,20,21,22,23,24,25. Thus, finding novel and sensitive biomarkers for this complicated disease seems to be imperative. A study reported that S100A12 serum levels may serve as molecular markers for sJIA diagnosis26. In addition, circulating miRNA from the blood, for their characteristics of stability and availability, are emerging as ideal candidates.
In our study, we found that levels of miR-26a in plasma were increased in the active phase of patients with systemic-onset JIA. Similarly, the elevation of miR-26a levels has been observed in circulating peripheral blood from patients with RA27. It has been proven that miR-26a acts as an important regulator in cell proliferation, differentiation, and tumorigenesis28. In recent years, with the discovery of its strong expression in major immune organs and cartilage, scientific researchers have paid more attention to the study of miR-26a in arthritis development. Osteoclasts that arise from cells of the monocyte/macrophage lineage are involved in bone matrix erosion in the joints of patients with RA. Kim, et al observed that the expression of miR-26a is gradually increased during receptor activator of nuclear factor-κB ligand–induced osteoclast differentiation and negatively regulates osteoclast formation through suppression of connective tissue growth factor29. A study revealed that miR-26a targets the Toll-like receptor 3 gene and ameliorates arthritis severity in the pristine-induced arthritis rats17. These studies provide some clues for further functional and mechanistic study of miR-26a in the pathogenesis and development of sJIA.
The involvement of proinflammatory cytokines is of great importance in the pathogenesis of sJIA. However, the regulatory network of cytokine expression in sJIA is still unclear. We revealed that miR-26a levels have positive correlations with IL-6 levels in the plasma of patients with sJIA. IL-6 stimulation can induce upregulation of miR-26a in THP-1 cells, and in turn, increased miR-26a suppresses IL-6 expression in circulating monocytes by directly targeting the IL-6 3′-UTR. To a certain extent, the expression levels of miR-26a could reflect inflammatory severity of sJIA. IL-6 is implicated in sJIA pathogenesis and contributes to several important clinical features. Plasma levels of IL-6 are markedly elevated following the peak of fever30. Overproduction of IL-6 can induce reticuloendothelial iron block and hepatocytes producing acute-phase reactants31. Additionally, high levels of IL-6 are associated with microcytic anemia31 and periods of fever, thrombocytosis32, growth retardation, joint destruction, and osteopenia33. Effective control of cytokine levels could substantially reduce many symptoms. Our study might provide useful information to better understand the regulatory mechanism of cytokines in sJIA.
Interestingly, when we transfected THP-1 cells with miR-26a mimics, levels of IL-1β and TNF-α in the supernatant were also decreased (data not shown). This result is consistent with the antiinflammatory function miR-26a plays in the innate immune response. We anticipated that miR-26a might participate in a signaling pathway associated with proinflammatory cytokine expression; this requires further study. Angiogenesis is an additional pivotal pathology process in sJIA, and miR-26a is also suggested to serve as an antiangiogenesis regulator in various disease models34,35,36. It is therefore likely that the function of miR26a extends beyond the regulation of cytokines.
There are some limitations to our present study. First, to determine whether miR-26a can be a diagnostic biomarker, it is desirable to evaluate whether it can effectively distinguish sJIA from infectious diseases, which are characteristic with chronic fever. We would add the typical infectious diseases in our further studies to strengthen the contention that miR-26a may serve as a diagnostic biomarker for sJIA. Second, we only examined the effect of IL-6 on miR-26a in THP-1 cells. However, the main source of plasma miRNA remains unclear, so it is likely that other factors, potentially originating from abnormal cells in blood, also modulate the expression of miR-26a. Identification of these triggers may help to design strategies by stimulating blood cells to produce more endogenous miR-26a to decrease levels of proinflammatory cytokines and alleviate inflammatory conditions.
Our present study demonstrates that miR-26a in plasma may serve as a potential biomarker for sJIA diagnosis and proposes a novel involvement of miR-26a in innate immune response by regulating IL-6 expression. Our findings provide new insight into the pathogenesis of sJIA and useful information to further research.
Footnotes
Supported by Capital Health Development Scientific Research Fund (2011-1008-02).
- Accepted for publication April 18, 2016.








{kind=link}
{kind=link}
{kind=link}
{kind=link}