

Abstract
Objective. Clinical and psychosocial attributes are associated with clinical outcomes after total knee replacement (TKR) surgery in patients with osteoarthritis (OA), but their relationship with TKR-related costs is less clear. Our objective was to evaluate the effect of clinical and psychosocial attributes on TKR costs.
Methods. We conducted a 6-month prospective cohort study of patients with knee OA who underwent TKR. We examined baseline demographic, clinical [body mass index (BMI) and comorbidities], and psychosocial attributes (social support, locus of control, coping, depression, anxiety, stress, and self-efficacy); baseline and 6-month OA clinical outcomes [Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) pain and function]; and 6-month direct and indirect TKR-related costs. Multiple regression was performed to identify determinants of TKR-related costs.
Results. We included 212 patients; 66% were women, 71% were white, and the mean age was 65.2 years. The mean baseline WOMAC pain score was 55 (SD 19) and WOMAC function score was 54 (SD 20). Mean total TKR-related costs were US$30,831 (SD $9893). Multivariate regression analyses showed that increasing BMI and anxiety levels and decreasing levels of positive social interactions were associated with increased costs. A lower cost scenario with a lower range of normal BMI (19.5), highest positive social interaction, and no anxiety predicted TKR costs to be $22,247. Predicted costs in obese patients (BMI 36) with lowest positive social interaction and highest anxiety were $58,447.
Conclusion. Increased baseline BMI, anxiety, and poor social support lead to higher TKR-related costs in patients with knee OA. Preoperative interventions targeting these factors may reduce TKR-related costs, and therefore be cost-effective.
Total knee replacement (TKR) surgery has been shown to be an effective treatment for patients with endstage osteoarthritis (OA) of the knee who did not respond to medical therapy1,2,3. However, TKR is a costly intervention, with a heavy economic burden in the United States. In 2007, the average cost per procedure was about US$25,000, representing total hospital charges of nearly US$16 billion4,5. Although TKR has been shown to be cost-effective4,6,7,8,9, 20%–40% of patients do not achieve clinically significant improvement4. Patients with persistent, moderate to extreme functional impairment at 3 and 6 months after surgery report increased use of health services and higher productivity losses, which leads to even higher health-related costs10. Lack of success can occasionally be attributed to surgical complications, comorbidities, or medical reasons, but the incidence of these problems is low and does not appear to contribute substantially to the longterm functional outcomes11,12,13,14. Moreover, psychosocial factors have been shown to be involved in the functional outcomes after TKR15,16. We have previously demonstrated that psychosocial and educational barriers are independent determinants of recovery after TKR. Low educational levels, little tangible support, depression, low levels of problem-solving coping, high levels of dysfunctional coping, and low internal locus of control negatively influence postoperative outcomes17. However, the relationship between these psychosocial attributes and TKR-related costs has not been established.
The aim of our study was to evaluate the effect of clinical and psychosocial attributes on TKR-related costs in patients with knee OA during the first 6 months after the procedure, and after adjusting for clinical variables including body mass index (BMI) and comorbidities. We hypothesized that poor baseline psychosocial skills and resources lead to not only poor postoperative outcomes, but also increased TKR-related costs during the initial 6 months of followup.
MATERIALS AND METHODS
Patients
The Patient Expectations about Knee Surgery cohort was a prospective cohort study of patients with knee OA who underwent TKR4,17. Patients were recruited between December 2004 and May 2007 from 2 outpatient orthopedic clinics affiliated with St. Luke’s Episcopal Hospital in Houston, Texas. Inclusion criteria were as follows: (1) radiologic diagnosis of knee OA, (2) first TKR procedure (previous hip replacement surgery was allowed), (3) adequate cognitive status, (4) living in the community (not in longterm care facilities), and (5) ability to communicate in English. All patients in the study had health insurance (private or Medicare). We excluded patients who were undergoing revision surgery, bilateral TKR, or unicompartmental replacement; patients diagnosed with inflammatory arthritis (e.g., rheumatoid arthritis), neurologic disorders, Paget syndrome, or other bone disorders; and patients involved in a litigation process related to surgery or seeking or receiving workers’ compensation benefits.
The study was approved by the institutional review boards of St. Luke’s Episcopal Hospital and the University of Texas MD Anderson Cancer Center. All participants signed an informed consent document.
Assessments
Patients were interviewed at baseline (within the month before they were scheduled for surgery) and followed for 6 months after surgery. Patient-reported outcomes were collected through self-report questionnaires at baseline and 2 weeks, 3 months, and 6 months after surgery. Healthcare use and cost data were collected at separate interviews with patients at baseline and 1, 2, 4, and 6 months after surgery. Data collected included demographic information, BMI, and self-reported current comorbidities including 9 conditions (heart failure, chronic lung disease, blindness or trouble seeing, deafness or trouble hearing, diabetes, asthma, gastrointestinal ulcer or bleeding, arthritis, and chronic low back pain). We added the number of present conditions for the comorbidity score.
Other measures included:
The Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) pain and function scales. The WOMAC is a well-known questionnaire that includes 5 items on pain and 17 on function18. Final pain and function scores are scaled 0–100, with 100 representing the worst pain and function.
The Medical Outcome Study–Social Support Scale (MOS-SSS). This 19-item scale measures patients’ perception of social support using 4 subscales: tangible support, affectionate support, positive social interaction, and emotional or informational support. A global score is also calculated as a weighted average of all items. All scale scores range from 1 to 5, with 1 representing the worst social support19.
The Depression, Anxiety and Stress Scale 21 (DASS21). This questionnaire includes 21 items and 3 subscales (i.e., depression, anxiety, and stress). Subscale scores range from 0 to 42, with higher scores indicating a worse emotional state20.
The Brief COPE Inventory. This questionnaire examines responses to stressors (i.e., coping mechanisms) and provides 3 summary scores: emotional coping, problem-solving coping, and dysfunctional coping. Each summary score ranges from 1 to 4, with 4 indicating the highest level of that coping behavior21.
The Multidimensional Health Locus of Control Questionnaire (MHLC). This questionnaire measures beliefs about what determines one’s health, using 3 subscales: internal (I am in control of my health), chance (my health is related to chance events), and powerful others (others have control over my health). Subscale scores range from 6 to 36, with 36 indicating the strongest beliefs22.
The Arthritis Self-Efficacy Scale. This questionnaire measures belief in one’s own capability to perform tasks or cope with adversity. Scores range from 0 to 10, with higher scores indicating more self-efficacy23.
The Life Orientation Test–Revised (LOT-R). This questionnaire measures optimism. The summary score was rescaled to a possible range of 0–100, with higher values indicating more optimism24.
Costs
The economic evaluation was conducted using a societal perspective. Cost analysis was performed according to 2007 prices and inflated to 2015 dollars using the Consumer Price Index for medical care as reported by the US Bureau of Labor Statistics. Medical costs were retrieved from 2 sources: hospital admission UB-92 billing statements and patient interviews. Our study horizon was 6 months after TKR, starting from the time a patient was admitted to hospital to undergoing TKR. No discount rate was applied owing to the short study time frame. We considered only TKR-related costs.
Direct medical costs were estimated using the Medicare Reimbursement Prospective Payment System25, and hospital billing was adjusted by cost-to-charge ratios reported to Medicare for the 2007 fiscal year26. Average wholesale prices reported in the 2007 Red Book were used to estimate medication costs27. Health-related transportation costs (direct, nonmedical costs) were calculated using the standard Internal Revenue Service mileage rates for people traveling because of medical issues28. Productivity losses for patients and their relatives (indirect costs) were estimated using a human-capital approach. Average wages per occupation for Texas were obtained from the US Bureau of Labor Statistics (fiscal yr 2007)29. A volunteer hourly mean wage was used to estimate productivity losses for those who were retired, disabled, unemployed, or students.
Additionally, we estimated patients’ baseline OA-related expenses prior to surgery using average self-reported OA-related costs 2 months prior to TKR (diagnostic tests and outpatient visits related to the surgery were excluded). Full details of the cost analysis are provided in our previous publication and in the data supplement (available online at jrheum.org)4.
Statistical analysis
The outcome measure of interest was patient total TKR-related costs at 6 months after the procedure. Unless otherwise specified, frequencies and percentages were used to summarize categorical variables, and means and SD were used to summarize continuous variables. Cronbach’s alpha coefficient was computed for each scale score at baseline to check for internal consistency. Mean baseline and 6-month scores were compared to identify changes between the 2 timepoints using paired Student t tests. Spearman rank correlations between baseline factors and outcomes at 6 months were also calculated for each variable, with the exception of sex and education, for which biserial correlation was used.
A linear regression model was used to assess the influence of various patient characteristics and psychosocial domain scores at baseline on TKR-related costs at 6 months, which were natural log–transformed to correct skewness. Transformation was performed on the outcomes to address nonnormality of the distribution. A linear regression model was obtained by first including an initial set of candidate predictor variables with p < 0.20 in the univariate analysis. A stepwise elimination Student t test was then performed using p < 0.10 to enter the model and p < 0.05 to stay in the model. Patient age, sex, baseline functional status, and costs incurred prior to surgery (log-transformed) were kept in the model regardless of significance. Once the list of variables to be used in our final model was selected, the functional form of each variable and multicollinearity between the variables were examined.
Because depression and anxiety scores were moderately correlated, models that considered only depression, or only anxiety, were run. Taking into account the association between employment and comorbidity (employed patients were likely to have fewer comorbidities than disabled and retired patients), we also ran models that considered only the number of comorbidities as a predictor (excluding employment).
Finally, to estimate the hypothetical effect of a psychosocial intervention on TKR costs, we performed a 2-way sensitivity analysis using multiple regression estimates. A 2-sided p value of 0.05 was considered statistically significant. All statistical analyses were performed using SAS 9.3 (SAS Institute Inc.).
RESULTS
Of the 250 patients included in the main cohort, 212 were included in our current study (14 patients who underwent unicompartmental knee replacement and 24 patients with incomplete followup data were excluded)4,17. Patient baseline characteristics are presented in Table 1. Baseline levels of pain and function were moderate to severe (mean ± SD: baseline WOMAC pain scores 54 ± 19, and baseline WOMAC function scores 53 ± 20). Mean BMI was 33. Compared with patients who did not complete all assessments, patients who attended all followup visits and were included in our study had better baseline function and less pain (WOMAC function scores 53 ± 20 vs 62 ± 15, p < 0.01, and WOMAC pain scores 54 ± 19 vs 61 ± 19, p < 0.05). No statistically significant differences were observed between these 2 groups with regard to age, sex, race, education levels, income, comorbidities, or BMI.
Baseline patient characteristics (n = 212). Values are n (%) or mean ± SD.
Table 2 shows the internal consistency of the self-report questionnaires at baseline and the results of the paired Student t test comparing baseline and 6-month scores. Scale reliability was at least 0.60 in all psychosocial measures. All scores except the MHLC subscales and LOT-R showed a statistically significant change between baseline and 6-month followup.
Internal consistency (Cronbach’s alpha) of the psychosocial measures and changes in psychosocial attribute scores between baseline and 6 months after total knee replacement surgery. In ASES, higher scores indicate more self-efficacy; in the COPE Inventory, higher scores indicate more of the coping behavior; in DASS21, higher scores indicate worse emotional states; in LOT-R, high values imply optimism; in MHLC, higher scores indicate more of a particular belief; and in MOS-SSS, higher scores indicate more frequent availability of support.
The mean (SD) total TKR-related cost during the first 6 months after surgery was US$30,831 ($9893). Direct medical costs represented the largest proportion of the cost (65%, US$20,031, SD $5659), followed by indirect costs (34%, US$10,581, SD $7468), and direct nonmedical costs (1%, US$206, SD $208). Patients’ OA-related expenses prior to surgery were estimated to be US$1809 ($2728) per patient, with indirect costs representing the largest proportion (78%, US$1417, SD $2664), followed by direct medical costs (20%, US$356, SD $284) and direct nonmedical costs (2%, US$37, SD $37).
The correlation matrix between psychosocial attributes at baseline and TKR-related costs during the first 6 months after the procedure is presented in Table 3. Younger age, increased BMI, and increased expenses related to knee OA prior to surgery were associated with increased costs during the first 6 months after surgery. With regard to psychosocial attributes, characteristics associated with increased costs included low social support, depression, anxiety, low levels of optimism, and the belief that health was related to chance events. The largest correlations were observed for BMI and anxiety.
Correlations between patient baseline characteristics and TKR-related costs during the first 6 months after the procedure. In ASES, higher scores indicate more self-efficacy; in the COPE Inventory, higher scores indicate more of the coping behavior; in DASS21, higher scores indicate worse emotional states; in LOT-R, high values imply optimism; in MHLC, higher scores indicate more of a particular belief; and in MOS-SSS, higher scores indicate more frequent availability of support.
Table 4 shows the results of stepwise multiple linear regression analyses to determine the independent influence of baseline psychosocial attributes on TKR-related costs during the first 6 months after the procedure. Higher BMI and anxiety and reduced positive social interaction were associated with increased total TKR-related costs. For each increase in BMI unit, there was a 1% (US$299) increase in the geometric mean of TKR-related costs. For each single-unit of increase in the DASS21 anxiety score, we observed a 1.3% (US$384) increase in the geometric mean of TKR-related costs, and for each single-unit decrease in the MOS-SSS positive social interaction score, we observed a 6.6% (US$1833) increase in the geometric mean of TKR-related costs. The inclusion of the number of comorbidities as a predictor variable did not affect the conclusions from the model. The model explained about 25% of the variation in the costs, 7.2% explained by BMI, 5.0% by anxiety, and an additional 2.3% by social support. The remaining explained the variation related to demographic characteristics and medical expenditures before surgery.
Stepwise multiple linear regression model of the influence of baseline patient characteristics on TKR-related costs. For DASS21 anxiety, higher scores indicate more anxiety, and for MOS-SSS positive social interaction, higher scores indicate more frequent availability of positive social interaction.
Our model resulted in the following estimates for low and high risk of increased costs for a hypothetical female patient, white, 65 years old, baseline WOMAC function score of 53 (mean for cohort), and log of costs prior to surgery of 7 (mean for cohort). (1) Lower cost scenario: lower range of normal BMI (BMI = 19.5), highest score for MOS positive social interaction (MOS = 5), no anxiety (DASS21 = 0) = TKR costs predicted to be $22,247. (2) Higher cost scenario: obese (BMI = 36), lowest score for MOS positive social interaction (MOS = 1), highest anxiety (DASS21 = 42) = TKR costs predicted to be $58,447.
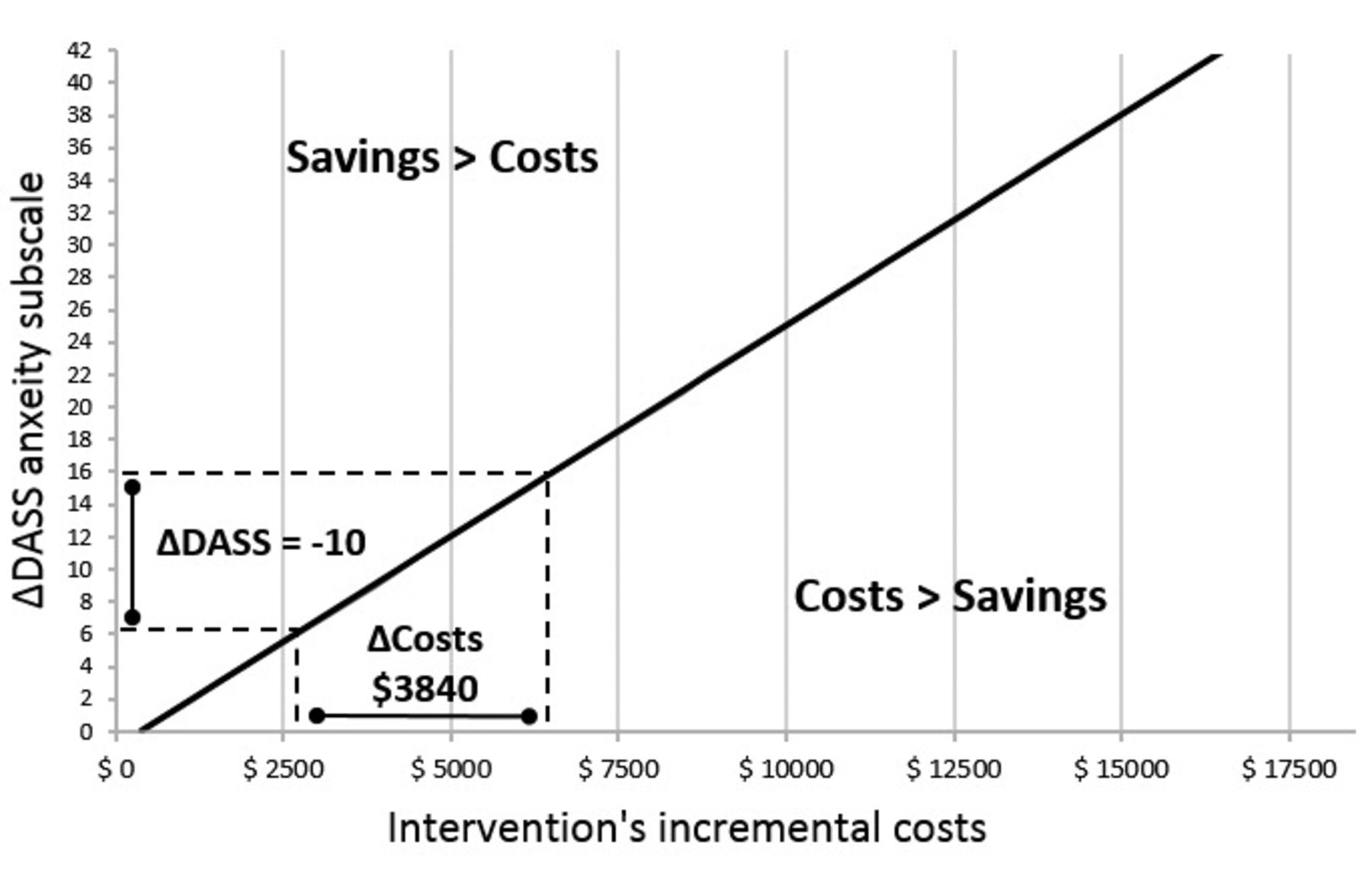
The hypothetical effect of a preoperative intervention on TKR-related costs is shown in Figure 1, which shows the relationship between the efficacy and cost of an intervention, presenting the results for each potential combination of values according to a cost-saving ratio. For example, an intervention that could reduce the anxiety level from severe to mild (i.e., a reduction in the DASS21 anxiety score from 16 to 6) would be cost-saving if the incremental cost of the program were less than US$3840.
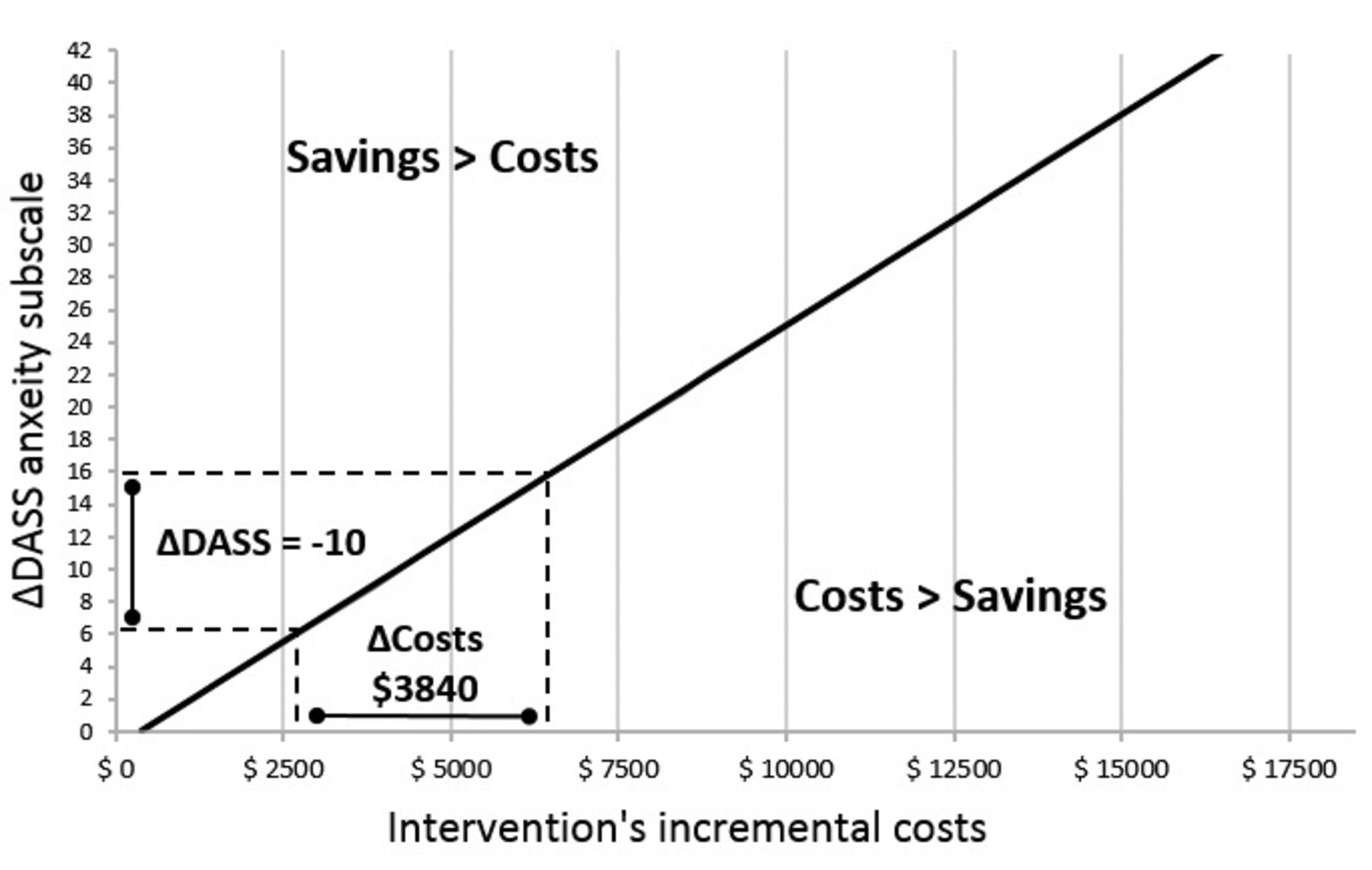
Two-way sensitivity analysis evaluating the cost-saving effects of a hypothetical intervention to reduce anxiety in patients undergoing total knee replacement surgery. For the DASS21 anxiety subscale, higher scores indicate more anxiety. Costs presented in US dollars. DASS21: Depression, Anxiety and Stress Scale 21.
DISCUSSION
Our study examined the relationship between baseline patient psychosocial attributes and TKR-related costs during the 6 months after the procedure, including both direct and indirect costs. We found that among the psychosocial attributes studied, baseline levels of social support and anxiety influenced TKR-related costs. Patients with high levels of anxiety and low levels of positive social interactions were more likely to have high TKR-related costs at 6 months after the procedure. In addition, we also found that BMI had the largest independent effect on costs, more so than other comorbidities combined. A study at a single US center also found that obesity increases length of stay and direct medical costs30,31.
Other studies have found an association between high baseline levels of anxiety and increased use of healthcare resources after TKR, as well as increased pain and knee disability, but have not incorporated an economic evaluation as we present here32,33,34. Other psychosocial characteristics, including tangible support, depression, problem-solving coping, dysfunctional coping and internal locus of control, mental health, pain catastrophizing, and preoperative expectations, have also been associated with TKR outcomes14,16,17. Patients with poor social support had worse functional outcomes after surgery, including self-reported levels of pain, function, stiffness, and wellbeing16,33,35,36,37. Among patients with other chronic diseases, those with more positive social relationships also report better quality of life and lower levels of pain and fatigue38,39,40,41. In our study, positive social interactions were associated with a reduction in postoperative costs, suggesting that the positive outcomes associated with positive social interaction also result in reduced healthcare costs for the patient.
The effect of psychosocial interventions on healthcare costs has been examined in a number of studies and reviews, with some evidence that these interventions are cost-effective or cost-saving in a number of situations42,43. In a meta-analysis of 9 controlled studies, including studies of patients undergoing hip replacement or TKR, McDonald, et al44 found that preoperative education was beneficial in reducing preoperative anxiety (modest effect) and that individually tailored programs of education and support could be beneficial in reducing the length of hospital stay, especially when the programs were targeted to patients with the highest levels of anxiety who were most in need of support.
Our study had limitations. It was conducted at a single tertiary center in Houston, Texas, and therefore may not be fully generalizable to other settings with different demographic characteristics. We chose 6 months of followup because this is the period when the majority of the costs are incurred because it includes the surgery and initial rehabilitation; however, longer-term costs that we did not measure may also be important and have different determinants. Our costing method reflected costs at the time of our study, which were adjusted for 2015, so there could have been slight variations if the study had been conducted in different years; however, the major focus of our paper is on the determinants of costs, and the observed associations are likely to remain strong. Finally, our cohort only included individuals with health insurance and is consequently not generalizable to the uninsured, who may use less healthcare or use it differently, and have different indirect and nonmedical direct costs.
The cost implications of psycho-educational assessment and interventions for patients undergoing TKR have not been determined. To the best of our knowledge, our study is the first to prospectively examine both direct and indirect costs associated with TKR and their relationship to baseline psychosocial attributes. We found that low baseline levels of social support and high baseline levels of anxiety were associated with increased TKR-related costs, suggesting that a hypothetical intervention tailored according to the patient’s baseline levels of anxiety and social support could help reduce TKR-related costs during the first 6 months after the procedure. An adequate preoperative assessment is essential to identify high-risk patients (i.e., those with poor psychosocial skills and resources) so that resources can be distributed to patients most in need of support. Finally, BMI was the strongest predictor of TKR costs, more so than comorbidities. Efforts aimed at reducing BMI prior to surgery may prove to be cost-effective. We expect that our findings will lead to the development and evaluation of potentially cost-saving interventions to enhance surgical recovery, functional outcomes, and patient satisfaction.
ONLINE SUPPLEMENT
Supplementary data for this article are available online at jrheum.org.
Acknowledgment
The authors thank Erica Goodoff for her editorial review of this manuscript.
Footnotes
Supported by a grant from the US National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS; NIAMS R01 AR48662). M.E. Suarez-Almazor is the recipient of a K24 career award from NIAMS (NIAMS K24 AR053593). H. Lin is supported by a Cancer Center Support Grant from the US National Cancer Institute (CA016672).
- Accepted for publication April 20, 2016.








{kind=link}