

Abstract
Objective. To examine whether different groups of fatigue trajectories can be identified among patients with early symptomatic osteoarthritis (OA) of the knee or hip, to describe the level of fatigue severity within each of these fatigue groups, and to investigate the involvement of age, sex, use of medication, comorbidity, and OA severity in relation to group membership.
Methods. Six years of followup data on fatigue (Medical Outcomes Study Short Form-36 Vitality scale) came from the Cohort Hip and Cohort Knee (CHECK) cohort. Growth mixture modeling was applied to identify distinct fatigue trajectories as well as to take into account the effects of the patient characteristics.
Results. Three fatigue trajectories were identified: low fatigue, low-to-high fatigue, and high fatigue. Latter trajectories showed considerable overlap from years 2 to 6, but differed in some patient characteristics in comparison with each other and in comparison with the low fatigue group. Comorbidity, medication use, and sex were significantly associated with the identified trajectories. Women, individuals with a comorbid disease, and those who used medication were more likely to follow a high fatigue trajectory.
Conclusion. These findings suggest heterogeneous development of fatigue in the early OA population associated with varying patient characteristics. Further, this study shows that a considerable number of patients with OA already experience elevated levels of fatigue at an early stage of OA. While these findings need to be replicated, the identification of these trajectories with differing patient characteristics may warrant tailored psychosocial interventions for patients with elevated levels of fatigue.
One of the most prevalent symptoms reported by patients with osteoarthritis (OA) besides pain is fatigue1,2. Nevertheless, as emphasized by patients, fatigue has almost no involvement in treatment decisions and is mainly neglected in the communication between healthcare providers and patients3. This negligence might be due to a lack of knowledge concerning the severity and effect of fatigue in OA.
Only a few studies have examined fatigue in OA, showing that fatigue is ubiquitously present and related to several physical and mental health aspects1,4,5,6,7,8,9,10,11,12. Not only older patients with severe OA have increased levels of fatigue and are affected physically and mentally by it, but middle-aged adults with early or moderate OA also report higher fatigue levels and experience the debilitating influence of fatigue on their physical functioning, mental condition, and social and daily activities2,3. The latter 2 studies described the experience of fatigue and its consequences qualitatively among a small sample. For representative OA cohorts, little is still known about the actual severity of fatigue in early OA and its clinical relevance. Research pointed to intraindividual variability in fatigue experienced among patients with OA10,13,14, and showed that this variation was negatively associated with daily changes in positive events and positively related to pain10,13. In addition, heterogeneity regarding fatigue in a population of older adults with OA was described15, suggesting that there are notable differences in the levels of fatigue between patients with OA. However, no study has yet examined differences in the development and severity of fatigue between patients with OA over a period of several years, and whether patient characteristics or severity levels of OA (e.g., based on radiologic evidence) are related to differences in the development and severity of fatigue. Further, although age is a known risk factor for OA, its involvement in relation to fatigue in OA is less clear. One study found that middle-aged adults with OA reported more difficulties coping with OA symptoms and the consequences of the disease than older individuals with OA3, possibly indicating an association between age and fatigue. Another rarely studied issue is whether men and women experience OA fatigue differently.
Our study set out to identify distinct groups of longterm fatigue trajectories in patients with early symptomatic OA of the hip or knee, and to explain the differences between and within these subgroups using patient characteristics, including age, sex, medication use, comorbidity, and OA severity. The identification of distinct longitudinal fatigue trajectories and their relation with specific patient characteristics can offer profound knowledge about fatigue in early OA and might provide indications for tailored treatment of OA-related fatigue.
MATERIALS AND METHODS
Study design and recruitment
Our present study used longitudinal data — 7 waves collected during a period of 6 years — originating from the Cohort Hip and Cohort Knee (CHECK) study. CHECK is an ongoing prospective cohort study consisting of 1002 participants with early symptomatic OA of the knee or hip. The cohort, formed from October 2002 to September 2005, is the result of the collaboration of 10 general and academic hospitals in the Netherlands. The study was approved by the medical ethics committees of all participating centers.
Individuals were included if they had pain or stiffness of the knee or hip, were aged 45–65 years, and had not previously consulted their physician regarding these symptoms. They were excluded if further research revealed any other pathological condition that could explain the symptoms (e.g., other rheumatic disease, previous hip or knee joint replacement, congenital dysplasia, osteochondritis dissecans, intraarticular fractures, septic arthritis, Perthes disease, ligament or meniscus damage, plica syndrome, Baker cyst), in cases of comorbidity that did not allow physical evaluation and/or a followup of at least 10 years, malignancy in the past 5 years, and the inability to understand the Dutch language16.
General practitioners in the region of the participating centers were asked to refer those patients who matched the inclusion criteria to the nearest center. Participants were recruited through advertisements and articles in local newspapers, and through the Dutch Arthritis Association website. All patients were checked for eligibility by physicians in the participating centers and asked to give their written informed consent.
Measures
Fatigue was measured using the Medical Outcomes Study Short-Form 36 Health Survey Vitality scale (SF-36 VT)17, an often-applied instrument in musculoskeletal research to assess fatigue among rheumatology patients. Its reliability is measured in internal consistency (0.84 to 0.92), and test-retest (r = 0.92) is excellent18,19. Further, the construct validity of the SF-36 VT is generally considered good20, and its criterion validity varies from moderate to very strong based on correlations with the Functional Assessment of Chronic Illness Therapy Fatigue (FACIT-F; 0.73–0.84), Multi-Dimensional Assessment of Fatigue (−0.54 to 0.79), and the Bristol Rheumatoid Arthritis Fatigue Multi-Dimensional Questionnaire (BRAF-MDQ; −0.40 to 0.68) in OA and rheumatoid arthritis (RA) research18,21,22,23. The SF-36 VT includes 4 questions. These items evaluate how much of the time in the past 4 weeks participants “felt full of life,” “had a lot of energy,” “felt worn-out,” and “felt tired.” Each item has a 6-level response format ranging from “all of the time” to “none of the time.” The latter 2 items are reverse-coded prior to all items being summed and linearly transformed to a score ranging from 0 to 100, with lower scores representing more fatigue. Data from samples of the general Dutch population (mean 68.6, SD 19.3)24, Dutch cancer population (mean 60.1, SD 22.3)24, and an early RA cohort (mean 53.6, SD 20.6)25 were used to assess the fatigue severity in our early OA cohort24.
The Kellgren-Lawrence (KL) radiographic classification system was applied to measure OA severity26. For each patient, a KL grade at baseline was determined if possible with regard to their left and right knees, and left and right hip. OA severity was defined as the maximum grade assigned to 1 of the 4 joints. At baseline, only patients with KL grades ≤ 1 were present, thus according to our definition, a dichotomous variable had been created with a group of individuals who had a KL score of 0 for all joints and a group of individuals who had a KL score of 1 concerning at least 1 of the 4 joints. Some patients (11.4%) could not be classified because of missing data on the KL variable for all joints.
In the CHECK cohort, the existence of comorbidity was assessed through a self-report health module of Statistics Netherlands, which included a list of chronic diseases27. Participants were first asked whether they had any other chronic disease or disorder besides their knee or hip complaints. Participants were then asked if they had or have had in the last 12 months the following diseases or disorders: disorder of the neck, shoulder, elbow, wrist, or hand; hypertension; back disorder (including slipped disc); migraine or chronic headache; asthma, chronic bronchitis, pulmonary emphysema, or chronic nonspecific lung disease; pharyngitis or sinusitis; thyroid disease; uterine prolapse; chronic inflammation of joints; diabetes mellitus; cholelithiasis; dizziness with falls; chronic urolithiasis; peptic ulcer or duodenal ulcer; severe heart disease or myocardial infarction; skin disease; or other longterm illness or disorder, e.g., bowel disorders, psychological disorders. For each participant, the presence of a comorbid disease was defined as having at least 1 distinct chronic disease or condition.
Statistical analyses
Growth mixture modeling (GMM) was applied to detect unobserved heterogeneity in the development of fatigue by identifying distinct homogeneous patient subpopulations within the early OA population, where each subgroup followed a different fatigue trajectory and where patients with early OA within a certain subgroup were more alike than patients with early OA between subgroups28,29,30. The optimal number of subgroups that identify the heterogeneity best was determined on account of parsimony, interpretability, and model fit indices31. A significant bootstrapped likelihood ratio test and adjusted Lo-Mendel-Rubin likelihood ratio test implied that a K-1 class model was rejected in favor of a model with K classes. Further, information criteria such as the Bayesian Information Criterion (BIC) and the sample-size adjusted BIC were compared between competing models, where a smaller value corresponds to a better model. Finally, the accuracy of classification was assessed through entropy and the average latent class assignment probabilities, where a value of ≥ 0.8 for entropy is desired for a clear delineation between trajectories, whereas a value close to 0 indicates classification uncertainty30,32. The average class assignment probabilities denote the amount of certainty that individuals belong to a certain group. This probability is also required to be near 0.8 to distinguish between groups. Both GMM with linear slopes and models with quadratic slopes were evaluated to incorporate both linear and nonlinear fatigue change.
After determining the best-fitting model, baseline patient characteristics were added as predictors to explain the differences between and within the identified subgroups. The between differences were analyzed using a multinomial logistic regression, with the latent categorical variable (the number of trajectory groups) as the outcome variable. In addition, the within differences were assessed by regressing the latent continuous variables (intercept, and linear and quadratic slope) on the patient characteristics. All analyses were performed in Mplus, version 7.1.
RESULTS
Patient characteristics of the early OA sample
Table 1 provides an overview of the patient characteristics at baseline. Two participants were omitted from analysis because of nonresponse on the SF-36 VT for all measurements, resulting in a total sample of 1000 participants with a mean age of 56 years and mostly women (79%). Further, in the early OA sample, cohabitation was the predominant marital status (82.8%), primary or secondary education was the highest attained education level for almost three-quarters of the sample (72.6%), and most patients were native Dutch speakers (88.1%). A sizeable portion of all patients frequently used at least 1 type of pain medication (37.9%), while the majority had 1 or more comorbid diseases (72.8%). On average, the early OA cohort scored 64.1 on the SF-36 VT, which denoted a higher fatigue level than the general population, but lower in comparison with the cancer population and the early RA cohort.
Patient characteristics at baseline (n = 1000). Valid percentages are listed in case of missing data. Medication use is defined as using at least 1 type of NSAID (acetaminophen, aspirin, ibuprofen, or other). Comorbidity is defined as any distinct additional disorder. For OA severity, a 0 is assigned to patients with a KL score of 0 for all joints, and a 1 to patients with KL score of 1 for at least 1 of the 4 joints examined. Values are n (%) unless otherwise specified.
Assignment of individual fatigue trajectories into fatigue subgroups
An overview of the GMM analyses and the corresponding fit statistics are shown in Table 2. All models depicted in Table 2 are specified with linear and quadratic slopes. These models outperformed models with linear slopes only (not shown). Based on parsimony, interpretability, and fit indices, the 3-class quadratic fatigue model was chosen as the best model for describing the fatigue development of the early OA sample. Somewhat problematic was the relatively low entropy value for our final model. However, inspection of the estimated average latent class probabilities for the 3 fatigue groups showed that these were relatively low, albeit not far from 0.8 for 2 groups (0.757 and 0.766) and good for the third group (0.863). The 2 groups with the lowest correct classification probability also showed the largest overlap as indicated by the misclassification probabilities of 0.211 and 0.154. This indicated that the observed fatigue trajectory for some patients within these latter 2 groups could not be assigned with a high degree of certainty to 1 group only.
Fit indices for various growth mixture models. The number of classes denotes the number of fatigue trajectory subgroups being estimated based on the individual trajectories of patients on the SF-36 VT. For example, the 1-class solution implies that a single mean growth trajectory fits all individual trajectories, whereas the 2-class solution assumes that patients with early OA can be divided into 2 subgroups based on their fatigue development. For each model, all classes contained linear and quadratic slopes to assess nonlinear fatigue development, if present.
Figure 1 shows the different fatigue subgroups that stem from the best-fitting GMM. The 330 patients (33.0%) who were assigned to the low fatigue group experienced a constant low level of fatigue early on in their disease process. The low-to-high fatigue group consisted of 213 patients (21.3%) who showed a fatigue trajectory that started with a low fatigue level at baseline, and continued to show a higher fatigue level until it leveled off toward the sixth year. The last group contained most individuals (n = 457, 45.7%). This trajectory group showed an almost steady higher level of fatigue. Although the latter 2 groups showed fatigue levels that were comparable with the cancer population, their level was slightly lower in comparison with the early RA cohort. As can be seen in the figure, the latter groups were difficult to distinguish because their fatigue patterns were quite similar after 2 years. However, the results from the conditional model, which included the patient characteristics as predictors (Table 3), showed that these 2 groups were perhaps more distinct than what was to be expected from the figure and the entropy value alone, and therefore could not simply be taken as 1 group.
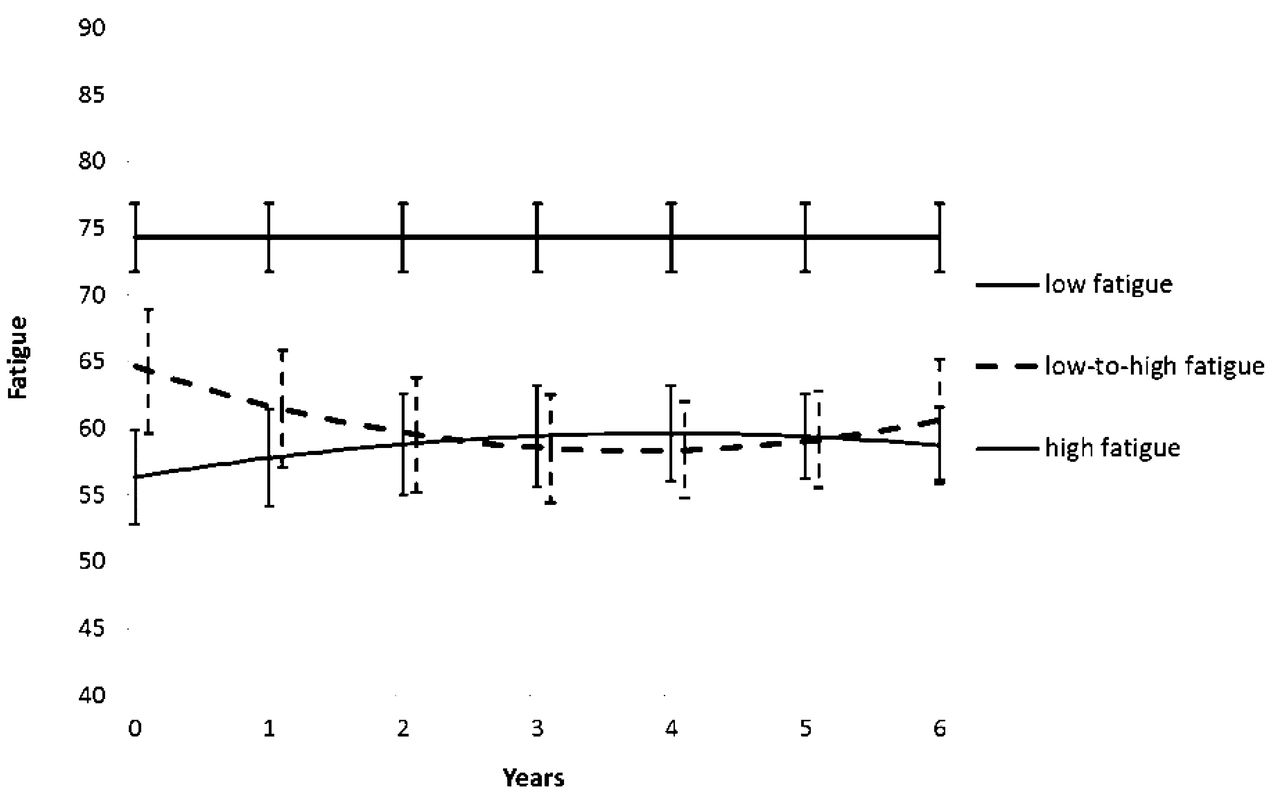
Three trajectories of fatigue were identified within the early osteoarthritis cohort: the low fatigue group (n = 330, 33.0%), the low-to-high fatigue group (n = 213, 21.3%), and the high fatigue group (n = 457, 45.7%). Lower numbers on the Y-axis indicate higher fatigue levels.
Associations between fatigue trajectories and patient characteristics: multinomial regression. The high fatigue group is the reference group. The number of cases used in the analysis is 870.
Differences in patient characteristics among the 3 groups
To assess the differences in patient characteristics between the fatigue trajectories, age, sex, medication use, comorbidity, and OA severity were added as predictors to the 3-class GMM. In this conditional model, the grouping variable, which represented the 3 different trajectories, was regressed on the predictors using multinomial regression analysis (Table 3). The high fatigue group was set as the reference class to clarify the differences and similarities between this trajectory group and the low-to-high fatigue trajectory. Sex, medication use, and comorbidity were found to be significantly and negatively related to the log odds of being in the low fatigue group versus the high fatigue group. Thus, relative to the high fatigue group, the odds of membership in the low fatigue group were significantly increased by being male, not using any nonsteroidal antiinflammatory drugs (NSAID), and not having a comorbid disease. The odds of being in the low fatigue group versus the high fatigue group were 2.128 (1 ÷ odds = 1 ÷ 0.47) times higher for men than women, 4 (1 ÷ 0.25) times higher for non-NSAID users than NSAID users, and 3.030 (1 ÷ 0.33) times higher for individuals without comorbid diseases than individuals with comorbid diseases. Relative to the high fatigue group, the odds of membership in the low-to-high fatigue group were significantly increased by not having a comorbid disease. The odds of being in the low-to-high fatigue group were 4 (1 ÷ 0.25) times higher for individuals without any comorbid disease than individuals who had a comorbid disease.
Explaining the individual differences within the 3 groups
The above-mentioned patient characteristics were also regressed on the intercepts and slopes to explain the individual differences in the initial fatigue level and the rate of change in fatigue within each trajectory group (Table 4). Age, comorbidity, and medication use were significantly related to the intercept of the low fatigue group. Within this group, younger patients, patients using medication, and patients with a comorbid disease started off with a higher fatigue level on average. The differences in individual fatigue levels at baseline within the low-to-high fatigue group were predicted by comorbidity and age, while the individual differences at the outset in the high fatigue group were predicted by comorbidity only. These initial differences stayed stable over the developmental course of fatigue, which followed from the nonsignificant effects on the slopes.
Estimated effects of the patient characteristics on the initial fatigue level and the rate of fatigue change for each trajectory group to explain the individual differences within each fatigue group (n = 870). Within each trajectory group, the initial fatigue level (intercept) and the rate of change in fatigue (linear/quadratic slope) are regressed on the patient characteristics. Note that the rate of change is not assessed in the low fatigue group because of a nonsignificant linear and quadratic slope. The resultant regression coefficients (= β) can be interpreted as coefficients derived from a linear regression model. For example, the sign and magnitude of the effect of sex indicate that the average starting point on the Vitality scale for female patients within the high trajectory group is 8.2 points lower than for male patients. On the other hand, the nonsignificant effect on the slope shows that female and male patients within the high fatigue group do not differ in their rate of fatigue change.
DISCUSSION
By studying fatigue longitudinally, we were able to provide a more detailed view of the fatigue experience of patients with early hip and knee OA. Three groups of patients with OA based on their longitudinal fatigue experience were found. The low fatigue trajectory group contained patients who displayed a stable and low level of fatigue over time. The low-to-high fatigue trajectory is characterized by lower fatigue at the start and elevated fatigue toward the end, while the high fatigue trajectory starts with a higher fatigue level and shows a slight decline in fatigue before it ends up with a higher fatigue level. The latter groups were difficult to distinguish because of considerable overlap in their developmental course after the second year, although the differences in patient characteristics possibly indicate the need for keeping these groups separated. These 2 trajectories indicate that elevated levels of fatigue, albeit slightly less elevated compared with the early RA cohort25, are already apparent during the early stage of the disease process for many patients with OA. This finding is in line with previous qualitative reports on fatigue among individuals with OA with early to moderate symptomatic OA3. More importantly, our study shows that fatigue in early OA cannot simply be identified by a single developmental pattern to describe the fatigue experience of all patients with early OA. This implies that awareness is required regarding the existence of different homogeneous subgroups of fatigue trajectories in the early OA population.
The different fatigue trajectory groups also increase our understanding of why certain patients with OA are more susceptible than others to experience elevated levels of fatigue at this early stage of OA. Our results indicate that patients with 1 or more comorbidities compared with patients without a comorbid disease are more likely to show a high fatigue pattern versus a low fatigue or low-to-high fatigue trajectory. This is in accordance with the finding that a comorbid disease places an additional burden on the physical and mental health of patients with OA27. We also found that patients who receive NSAID are more likely than patients who do not receive NSAID to be in the high fatigue group. The same goes for female patients compared with male patients. The sex difference is consistent with research findings on fatigue in RA, where being a woman is related to higher fatigue levels33,34. This could indicate that women with early symptomatic OA have more trouble coping with their transition from health to disease than men. These findings suggest that the presence of 1 or more comorbid diseases, and to a lesser extent the use of NSAID and being female, seem important in predicting which fatigue development a patient with OA is most likely to follow.
Although age did not predict group membership, evidence was found for age being related to the interindividual differences in fatigue at baseline, with younger aged patients showing higher levels of fatigue. This could be explained by different expectations and role responsibilities in middle and late adulthood. People in their 40s do not expect OA symptoms that early in their life course and thus experience more distress. In addition, in middle adulthood the combination of different roles — having a career, a spouse, small children, and a social life — might be more demanding than in later phases of adulthood. Moreover, personal growth expectations might be still higher than in late adulthood. This is in line with previous findings that younger adults with OA more often report being frustrated and stressed about the physical and social consequences of their disease than older adults3. The combination of frustration, stress, and role conflicts may contribute to higher levels of fatigue.
Several limitations of our present study deserve mention. First, it is unclear whether the levels and development of fatigue in the low-to-high and high fatigue subgroup are consequences of the disease process itself, or perhaps are due to other factors unrelated to OA. However, the relative size of both groups and similarity in fatigue level compared with the cancer population and the early RA cohort suggest that fatigue is involved in OA. Second, while the influence of several patient characteristics on the trajectories was assessed, other important explanatory variables were not examined in our present study. Future studies could determine whether other factors known to be related to fatigue, such as pain, sleep deprivation, and depression7,10,11,12,13, predict the most likely trajectory for a patient with early OA. These additional risk factors are important because the predicted fatigue development may offer guidance for clinicians in tailoring interventions to the specific needs of the patient groups. Further, in addition to examining the association between presence of comorbidity and trajectory membership, the effect of specific chronic diseases as well as the effect of the number of comorbidities were examined. Because of increasing model complexity, these analyses led to numerous modeling difficulties, such as non-identified models and untrustworthy and nonsensical estimates. Nevertheless, teasing out the effects of specific chronic conditions seems worth assessing in future studies because it has been shown that comorbid diseases differ in their effect on the mental and physical health of patients with OA27. Also, the finding that OA severity was not related to the identified fatigue trajectories might be explained by the limited range of radiographic evidence present in our sample. In addition, our present study did not assess whether differences between and within trajectories could be accounted for by symptomatic evidence. Future studies could include a wider range of symptomatic and radiographic evidence, which may differentiate between the trajectories in a better way than the severity measure applied in our present study.
Another issue that needs to be addressed is the use of the SF-36 VT as a fatigue measure, because its application might be seen as suboptimal on the background of existing specific multidimensional fatigue scales for arthritis conditions. However, it is unknown whether different fatigue dimensions are relevant for OA, as has been described for RA35, and whether questionnaires with high measurement precision on very severe levels of fatigue (for example, FACIT-F or BRAF-MDQ36,37) would reflect the fatigue levels in this early OA sample adequately. With the SF-36 VT, we applied a generic instrument with established good discriminatory power at low and average fatigue levels to analyze the severity and longitudinal trajectories of fatigue in early OA. Based on the finding that a large number of patients experienced elevated levels of fatigue, the assessment with instruments for higher levels of fatigue is recommended. The dimensionality of OA fatigue should be considered for future studies.
Our present findings indicate and confirm that early in the disease course, many patients with OA of the hip or knee already experience elevated levels of fatigue. This warrants more attention for fatigue in OA research to enhance our understanding of the degree of resilience in patients with early OA in facing physical, mental, and social challenges, as well as improving our understanding of the disease process itself. The different trajectories together with the varying patient characteristics identified in our present study suggest the need to tailor psychosocial interventions and self-management strategies according to specific needs. Future studies are required to validate the fatigue trajectories and to elucidate the underlying mechanisms of these distinct trajectories by incorporating additional psychosocial and clinical factors.
Acknowledgment
The chair of the Cohort Hip and Cohort Knee (CHECK) is Professor J.W.J. Bijlsma and the coordinator is J. Wesseling, MSc. Participating institutions are the Erasmus Medical Center, Rotterdam; Kennemer Gasthuis, Haarlem; Leiden University Medical Center; Maastricht University Medical Center; Martini Hospital Groningen/Allied Health Care Center for Rheumatology and Rehabilitation, Groningen; Medical Spectrum Twente Enschede/Ziekenhuisgroep Twente; Reade, Center for Rehabilitation and Rheumatology (formerly Jan van Breemen Institute)/VU Medical Center, Amsterdam; St. Maartenskliniek, Nijmegen; University Medical Center, Utrecht; and Wilhelmina Hospital, Assen.
Footnotes
Cohort Hip and Cohort Knee (CHECK) is funded by the Dutch Arthritis Association and led by a steering committee consisting of 16 members with expertise in different fields of OA.
- Accepted for publication March 15, 2016.








{kind=link}