

Abstract
Objective. The incidence of primary systemic vasculitides varies among different geographic regions and ethnic origins. The aim of this study was to examine the incidence rates of vasculitides in the Jerusalem Jewish population, and to examine possible trends in incidence rates over a 20-year period.
Methods. The clinical databases of inpatients at the 2 medical centers in Jerusalem were searched for patients with vasculitis diagnosed between 1990–2009. Individual records were then reviewed by one of the authors. The significance of trends in incidence rates throughout the study period was evaluated by Pearson correlation coefficient.
Results. The average annual incidence rate of polyarteritis nodosa was 3.6/million adults (95% CI 1.6–4.7). Incidence rates did not change significantly during this period (r = 0.39, p = 0.088). The incidence of granulomatosis with polyangiitis (GPA) was 4.1 (2.2–5.9) for the whole period, during which it increased significantly (r = 0.53, p < 0.05). The incidence of microscopic polyangiitis (MPA) was lower: 2.3 (1.2–3.5)/million. It also increased significantly (r = 0.55, p < 0.05). The incidence of eosinophilic granulomatosis with polyangiitis was 1.2 (0.4–1.9), which remained stable throughout the study period. The incidence of Takayasu arteritis was 2.1/million (95% CI 1.2–2.9), and it also remained stable. Giant cell arteritis (GCA) incidence was 8.1 (5.7–10.6)/100,000 population aged 50 years or older. In sharp contrast with other vasculitides, its incidence decreased significantly throughout the study period (r = −0.61, p < 0.01).
Conclusion. The incidence rates of vasculitides in the Jewish population of Jerusalem are in the lower range of global incidence rates. While GPA and MPA incidence are increasing, GCA incidence is decreasing.
- VASCULITIS
- MICROSCOPIC POLYANGIITIS
- ISRAEL
- GRANULOMATOSIS WITH POLYANGIITIS
- GIANT CELL ARTERITIS
- INCIDENCE
The primary systemic vasculitides (PSV) are a heterogeneous group of inflammatory diseases of unknown etiology, affecting blood vessels of different sizes. The incidence of PSV varies among different geographic regions and ethnic origins. Giant cell arteritis (GCA) is more common in northern countries1,2,3, and Takayasu arteritis (TA) is considered more common in the Far East. Among the antineutrophil cytoplasmic antibodies (ANCA)-associated vasculitides (AAV), granulomatosis with polyangiitis (GPA) tends to be more common in Europeans, whereas microscopic polyangiitis (MPA) tends to be relatively more common in Japan and other Asian countries, and in Kuwait4,5,6. The incidence of polyarteritis nodosa (PAN) was reported to be exceptionally high in native Alaskans and in Kuwait, compared to reports from European countries6,7,8,9,10. These differences may be due to both ethnic and environmental factors4.
The Jewish people in Israel are unique in this regard: originating in the Middle East, they were dispersed in Europe after being conquered by the Roman Empire about 2000 years ago, and later spread mainly to North Africa and parts of the Middle East. They were largely conserved genetically with some local genetic influences throughout those centuries11. Upon emigrating to Israel during the last century, intermarriages between ethnic groups were initially uncommon, but became increasingly common in the last decades. Therefore those genetic pools are mixed mainly in the younger population.
The epidemiology of GCA in Israel has already been studied. Its incidence among the Jewish population in Jerusalem was reported to be similar to the incidence in southern European countries, but lower than incidence rates in northern countries12,13. Among Israelis, there were no differences between people in families emigrating from European countries and those emigrating from North Africa, Asia, or Middle Eastern countries12. Our aim was to examine the incidence rates of other PSV in the Jewish population of Jerusalem, and to examine possible trends in incidence rates over a 20-year period (1990–2009).
MATERIALS AND METHODS
The city of Jerusalem (latitude 31.77° north) is served by 2 major medical centers, Hadassah and Shaare-Zedek. The vast majority (more than 90%) of the Jerusalem Jewish population seeks medical advice and hospitalization within the city in those 2 medical centers. Non-Jews in Jerusalem occasionally seek medical advice in medical facilities elsewhere. That segment of the population was not included in this report.
The clinical databases of inpatients (including patients admitted for biopsy procedures) at each medical center were searched for patients diagnosed as PAN, MPA, GPA (formerly Wegener’s granulomatosis), eosinophilic GPA (EGPA, formerly Churg-Strauss syndrome), TA, or GCA, between 1990 and 2009. In addition, pathology and ANCA serology records were reviewed. Individual patient records were then reviewed by 2 co-authors (GN, GSB). Cases were included when either the American College of Rheumatology (ACR) 1990 classification criteria or the 1994 Chapel Hill Consensus Conference (CHCC) definition were fulfilled14,15,16,17,18,19. There was 1 exception: MPA cases were included if they met the 1994 CHCC definition, because no ACR classification criteria were available. Cases with isolated ANCA-positive glomerulonephritis were considered separately. Patients residing outside Jerusalem and non-Jewish patients were not included. Ethics approval for the project was obtained from the institutional ethics review committees.
Data on the Jerusalem population throughout the study period were obtained from the annual publications of the Israel Bureau of Statistics and the Jerusalem Institute for Israel Studies Statistical Yearbook20,21. Incidence rates of GCA were calculated per 100,000 Jewish adults (age 50 years or older), and incidence rates for other PSV were calculated per million Jewish adults (age 20 years or older). Incidence rates were calculated according to the annual population size. The significance of trends in incidence rates throughout the study period was evaluated by Pearson correlation coefficient.
RESULTS
The Jewish adult population (age 20 years or more) in Jerusalem was 219,400 in 1990 and steadily increased to 294,900 in 2009. The male:female ratio in this age group was 48:52 throughout this period. The older population (age 50 years or more) was 71,100 in 1990, steadily increasing to 108,500 in 2009. The male:female ratio in this age group was 45:55 throughout this period.
Epidemiological data on patients with PSV are summarized in Table 1 and Figure 1. Incidence rates were calculated for the whole 20-year period (Figure 1), and also divided into 4 quinquennial periods (Table 1).
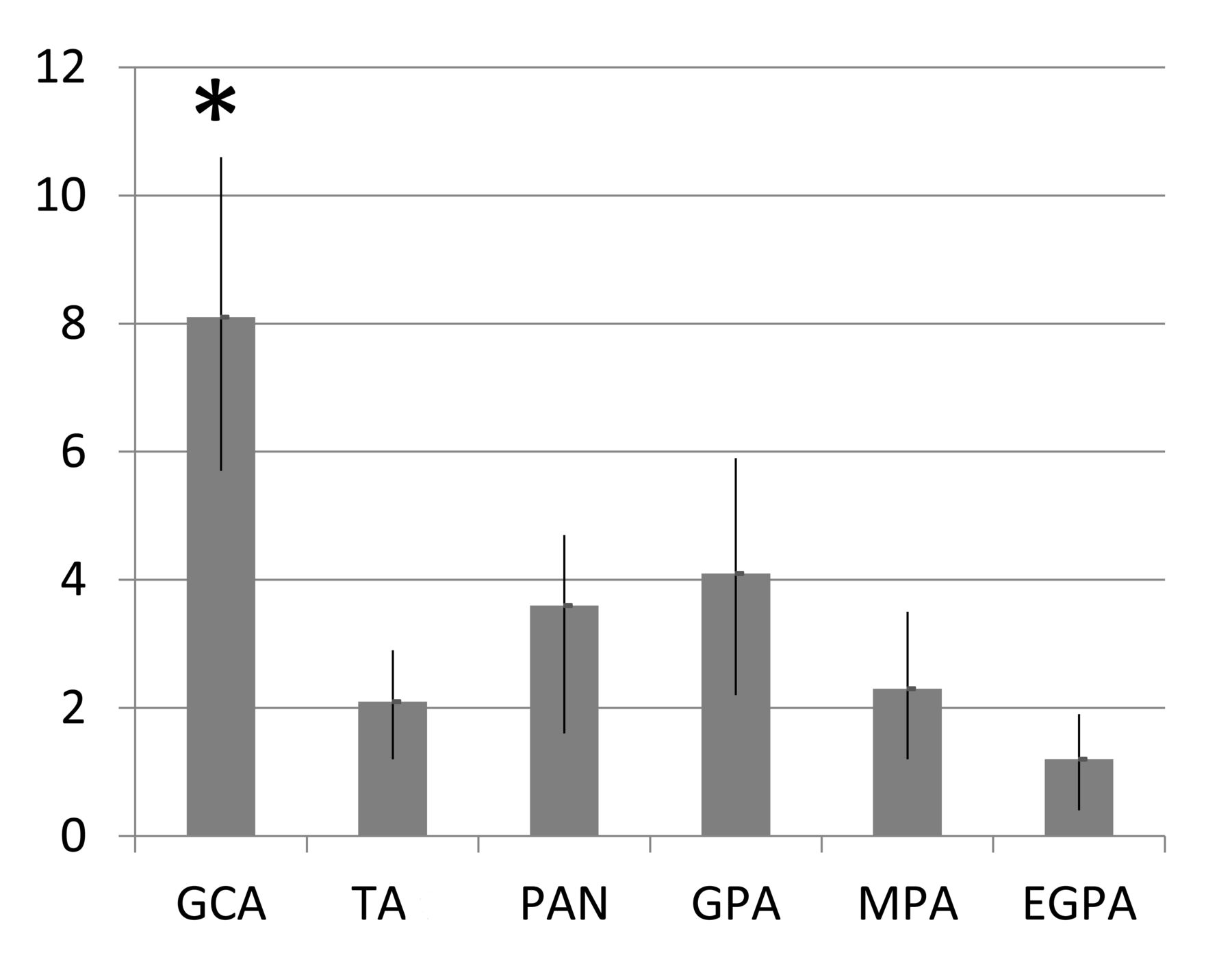
Incidence rates with 95% CI of primary systemic vasculitides in Jerusalem during 1990–2009 per 1 million adults (age ≥ 20 years). *Incidence in GCA cases was calculated per 100,000 adults, age 50 years or older. EGPA: eosinophilic granulomatosis with polyangiitis; GCA: giant cell arteritis; GPA: granulomatosis with polyangiitis; MPA: microscopic polyangiitis; PAN: polyarteritis nodosa, TA: Takayasu arteritis.
Incidence rates of PSV in Jerusalem during a 20-year period (1990–2009) and in quinquennial periods.
For the whole 20-year period, the average annual incidence rate of PAN was 3.6/million adults (95% CI 1.6–4.7) in the age group of 20 years and older. Mean age of the 17 patients with PAN at the time of diagnosis was 53 ± 14 years, and the male:female ratio was 1:1. The annual incidence rates of PAN did not change significantly (r = 0.39, p = 0.088) during this period. Three of the 17 patients had cutaneous PAN, and 14 had systemic involvement. Hepatitis B serology was reported in 11 cases: HBsAg was negative in all of them, and 1 patient had anti-core antibodies. ANCA serology was reported in 10 cases and was negative in all. Diagnosis was confirmed histologically in 11 patients and by imaging in 5 cases.
Among AAV, GPA was the most common: its incidence was 4.1 (2.2–5.9) for the whole period, during which it increased steadily and significantly (r = 0.53, p < 0.05), reaching an incidence of 6.2/million from 2005 to 2009. Patients with GPA were older, with 2:1 male predominance. ANCA serology was reported in 20 of the 22 GPA cases. Only 2 of these 20 patients were ANCA-negative: 1 had limited disease (involving the upper respiratory tract and orbit) and 1 had systemic involvement. Eighteen patients had positive cytoplasmic ANCA. None had a positive perinuclear ANCA (pANCA). Proteinase 3 serology was reported in 14 cases and all were positive. In addition, GPA diagnosis was histologically confirmed in 7 cases.
The incidence of MPA was lower than GPA: 2.3 (1.2–3.5)/million adults at the age group of 20 years or older. It also increased significantly during the 20-year period (r = 0.55, p < 0.05), reaching an incidence of 4.1/million during 2005 to 2009. The mean age at the time of diagnosis of the 15 patients with MPA was similar to that of the patients with GPA, but in contrast to GPA, females were predominant in MPA, 4:1. ANCA serology was reported in 13 of the 15 MPA cases. Only 2 of these 13 patients were ANCA-negative, and 11 patients had positive pANCA. Antimyeloperoxidase (anti-MPO) serology was reported in 9 cases and all were positive. In addition, MPA diagnosis was histologically confirmed in 10 cases. There were 3 additional cases with ANCA-associated glomerulonephritis. All 3 were pANCA-positive and 2 were anti-MPO–positive. None developed systemic vasculitis during a mean followup of 7 years.
EGPA was the least common among AAV with an incidence of 1.2 (0.4–1.9), which remained stable throughout the study period. The 6 patients with EGPA were younger, with no sex predominance. ANCA serology was reported in 5 of the 6 EGPA cases, 2 were ANCA-positive (pANCA). Anti-MPO was positive in 1 of them. EGPA diagnosis was histologically confirmed in 4 cases.
The annual incidence of TA was 2.1/million (95% CI 1.2–2.9), and it remained stable throughout the study period. Patients with TA were the youngest: 9 of the 11 patients were younger than 40 years at the time of diagnosis, but 2 were diagnosed at the age of 64. Both cases had long histories of constitutional symptoms and intermittently elevated erythrocyte sedimentation rates (ESR). Both had negative temporal artery biopsies and none fulfilled GCA classification criteria. All patients with TA were women. In all cases, TA diagnosis was supported by characteristic imaging findings (either direct vascular angiography or computed tomography angiography).
GCA was the most common PSV, with 140 patients diagnosed during this 20-year period, bringing the incidence rate to 8.1 (5.7–10.6)/100,000 population aged 50 years or older. Biopsy was to prove 83% of the cases. In sharp contrast with other PSV, GCA incidence decreased significantly during the study period (r = −0.61, p < 0.01). It reached a peak incidence of 14/100,000 from 1995 to 1999, but decreased sharply thereafter, reaching an incidence of 1.9 from 2005 to 2009. Patients with GCA were the oldest, with 2:1 female predominance.
DISCUSSION
The incidence rates of PSV in the Jewish adult population of Jerusalem are within the range of incidence rates reported in other populations, but tend to be in the lower part of the range in most PSV. Epidemiological data suggest that the overall incidence of PSV is similar in different places across the globe22. However, the incidence of individual PSV is more heterogeneous and appears to vary with location. In particular, GCA has long been known to be more common in Scandinavia and the northern United States (incidence rates of 16–36/100,000 aged 50 years or older), compared to countries in the southern part of Europe (Spain and Italy) and in Israel (incidence rates 6–12/100,000)1,2,3,23,24,25,26. However, reports from other European countries (Germany, Lithuania) described very low incidence of GCA (fewer than 4/100,000)27,28.
The reported incidence of PAN varies considerably from 77/million among native Alaskans (where hepatitis B is relatively common) to 16/million in Kuwait, and 1–9/million in several European countries and in Australia6,7,8,9,10,27,28,29,30,31. PAN incidence was in the lower part of this range in our population (3.2/million).
The incidence of MPA also appears to vary according to location, being more common in Kuwait (24/million) and Japan (18/million) compared to European countries and Australia (2–10/million)4,5,6,8,9,27,28,30,31. The incidence in our population was in the lowest part of this range (2.3/million). The variability in MPA incidence rates may be attributed in part to case selection: some studies included cases with renal limited involvement, while others included cases with additional features. In our study, cases with isolated ANCA-positive pauciimmune glomerulonephritis without additional features were not included. Inclusion of these cases would have increased MPA incidence to 3/million.
The incidence of GPA also seems to vary by location, with higher incidence rates reported in most European countries, Australia, and the United States (6–14/million) compared to Japan (2/million)4,5,8,9,28,31,32. The incidence rates in some European countries (Spain and Lithuania) were low (2–5/million)10,27,29,30, as was the incidence rate in our population (4.1/million). Because this is a hospital-based study, cases with limited GPA, such as isolated involvement of the upper respiratory tract, have been treated elsewhere because outpatients are not included in this report.
EGPA seems to be evenly distributed globally, with incidence rates of 1–3/million5,8,9,10,27,28,29,30,31. Again, the incidence in our population was in the lowest part of this range.
TA was initially believed to be more common in the Far East, but incidence rates do not differ considerably among the United States, European countries, Kuwait, and Japan, as well as in our population (1–3/million)10,27,28,33,34,35,36. A previous study from Israel describing 56 cases of TA found that all cases were in families that came from Africa and Asia37. Our results are in agreement with these findings. Two of the patients with TA were diagnosed at the age of 64 years. It is possible that they had large-vessel GCA; however, 1 patient had a long history of constitutional symptoms and intermittently elevated ESR since the age of 40. The other patient also had intermittently elevated ESR for many years, and had recurrent cerebral strokes since the age of 50. Both had negative temporal artery biopsies, both fulfilled TA classification criteria, and none fulfilled GCA classification criteria.
Some of the above differences in incidence rates are likely to be true; however, results of studies may be influenced considerably by differences in methodology and differences in disease definitions and classification. Most studies were retrospective in nature, a few were prospective. Retrospective studies are likely to underestimate incidence rates, and prospective studies are supposed to be more accurate. Indeed, 1 study from Sweden that started as a retrospective study reported increased rates of GCA in consecutive years while acquiring data prospectively23. Some studies were population-based whereas others were hospital-based. Hospital-based retrospective studies such as ours are likely to underestimate incidence.
Studies on epidemiology of PSV used either the ACR classification criteria or the CHCC definition or both. Some studies used the European Medicines Agency classification algorithm for AAV and PAN proposed by Watts, et al38, and some used their own criteria (especially studies prior to 1990). These differences may affect results39. Indeed, in the same time frame in 1 region in Spain, the incidence rates of GPA and of PAN were higher when ACR criteria were applied compared to CHCC criteria29,30. Studies of GCA incidence also varied according to patient selection: some included patients fulfilling ACR classification criteria, whereas others included only biopsy-proven cases, the latter practice apparently underestimating the incidence rates.
There is evidence to suggest that the incidence of PSV is changing, although the observed increasing incidence rates could be attributed to increased awareness and better ascertainment, especially with the development of ANCA as a diagnostic test for AAV40. This may explain the increasing incidence rates of GPA and MPA observed in our population.
In contrast to the increasing incidence rates of GPA and MPA and the stability of incidence rates of other PSV, the observed incidence rates of GCA in our population decreased significantly. Studies in other parts of the world show varying results: European studies reported increasing GCA incidence rates3,41. However, in a 50-year observation study in the population of Olmsted County, Minnesota, USA, the incidence rates increased between 1950 and 1979, but remained stable with a tendency to decrease since then26. The reasons for the change in GCA incidence in our population are not clear. Our findings may reflect true changes in disease incidence, but it is possible that increasing numbers of cases have been diagnosed and treated on an outpatient basis and therefore are not included in this evaluation, resulting in underestimation of the true incidence. This is less likely because 90% of rheumatologists in Jerusalem are hospital-based. Patients suspected of having GCA by their primary care physicians, neurologists, or ophthalmologists are often treated initially with corticosteroids, but then referred to hospitals for rheumatology consultations and temporal artery biopsies. A limited survey of primary care physicians did not disclose any unreferred GCA cases. Still, it is possible that in recent years some patients were not referred, and that the true incidence is actually higher. Only a population-based study would provide a more definite answer.
The incidence rates of PSV in the Jewish population of Jerusalem are in the lower range of global PSV incidence rates. While GPA and MPA rates are increasing, GCA rates are decreasing. It is not clear whether these observations are consequent to ascertainment bias, or reflect true changes in the incidence rates.
- Accepted for publication January 12, 2016.








{kind=link}