

Abstract
Objective. To examine the influence of concomitant methotrexate (MTX) with adalimumab (ADA) on outcomes in patients with psoriatic arthritis (PsA) using data from an observational study of ADA.
Methods. Data from a German noninterventional study of patients with PsA starting treatment with ADA were analyzed retrospectively for effects of concomitant MTX on key outcomes, including Disease Activity Score-28 joints, tender and swollen joint counts, skin assessments, and safety. Patients were categorized into those with symptoms of axial involvement and those with no symptoms of axial involvement as judged by the examining clinician.
Results. A total of 1455 patients met the study criteria, 296 with axial involvement (ADA monotherapy = 165; plus MTX = 131) and 1159 with no axial involvement (ADA monotherapy = 658; plus MTX = 501). ADA, alone or combined with MTX, resulted in strong and comparable reductions in disease activity measures in patients with and those without axial disease over 24 months of therapy. In multiple regression analyses, concomitant MTX did not affect joint or skin outcomes in either the group with axial manifestations or the group without axial disease. Neither adverse event rates nor withdrawal rates were significantly influenced by concomitant MTX.
Conclusion. ADA is an effective treatment option for patients with PsA with or without axial involvement. Compared with ADA monotherapy, the use of concomitant MTX with ADA does not improve articular or skin outcomes in patients with PsA regardless of axial symptoms. Trial registration: Clinicaltrials.gov NCT01111240
The clinical efficacy of concomitant therapy with inhibitors of tumor necrosis factor (TNF) and methotrexate (MTX) has been well established for rheumatoid arthritis (RA)1,2,3. However, the influence of concomitant MTX has been less clear for patients with psoriatic arthritis (PsA)4. A placebo-controlled prospective multicenter study was unable to document the benefits of MTX monotherapy in reducing synovitis in patients with PsA5, but to our knowledge no randomized trial has addressed the influence of concomitant MTX on the effectiveness of TNF inhibitors in patients with PsA. There is some evidence that MTX may contribute to improved treatment persistence with anti-TNF therapy6,7, particularly when used in combination with infliximab, but there are few data to support a benefit in effectiveness outcomes in patients with PsA treated with concomitant MTX and TNF inhibitors, including adalimumab (ADA)8,9. Consequently, the latest European League Against Rheumatism guidelines for the pharmacologic management of PsA include studies of combination therapies with conventional disease-modifying antirheumatic drugs (DMARD) and biologic agents on the research agenda10.
A potential confounding factor in studies of the clinical effectiveness of concomitant MTX is the lack of activity of conventional DMARD in patients with axial disease10. It is possible that MTX improves joint symptoms in the subset of patients with PsA without axial disease, but not in those with axial involvement. Patients with axial manifestations may account for 25% to 75% of patients with PsA, depending on disease duration and the accuracy of diagnosis11. However, the prevalence of axial disease is not reported in many retrospective PsA studies, and thus its potential effect on the reported response of PsA to MTX treatment has not been investigated. To evaluate the effect of concomitant MTX in PsA patients with varying disease presentations, we conducted an analysis of data from a large noninterventional study of patients with PsA who were treated with ADA at the decision of their clinician.
MATERIALS AND METHODS
Study design
This was a retrospective analysis of data from a multicenter, prospective, noninterventional study of patients with PsA who received ADA therapy at the decision of and under the direction of their physician during routine clinical practice at 355 centers (234 rheumatology centers, 101 dermatology centers, and 20 general practices) in Germany. The main objective of our study was to examine the influence of concomitant MTX on patient outcomes (effectiveness and safety) during routine clinical practice and to determine whether this effect varied depending on the pattern of musculoskeletal manifestation (axial manifestations or no axial manifestations). The use of concomitant therapies, including MTX, was at the decision of the clinician and was not influenced by this retrospective evaluation.
Patients enrolled in the ADA noninterventional study had a diagnosis of PsA and active disease as judged by the clinician. Patients who had received previous treatment with ADA and did not have documentation of musculoskeletal disease, or had received concomitant therapy with a DMARD other than MTX, were excluded from the analyses presented here. Previous treatment with TNF-α inhibitors other than ADA was not an exclusion criterion. All patients were informed of the objectives of the study and gave written consent for their voluntary participation and the anonymous use of their personal data in statistical analyses. Because this was a noninterventional study that used anonymized data sets, ethics approval was not required by German law.
All patients enrolled in the noninterventional study who initiated ADA monotherapy or ADA plus MTX between August 2005 and December 2009 and had adequate postbaseline data were included in these analyses. Patients were categorized into those with symptoms of axial involvement as judged by the examining clinician during the baseline physical evaluation (axial PsA) and those with no evidence of axial involvement (no axial PsA).
To assess the effect of therapeutic changes during the 24-month period, subgroup analyses were conducted on patients who discontinued concomitant MTX or initiated concomitant MTX in each group (axial PsA and no axial PsA). These additional analyses were performed to address the possibility that the response curves of ADA monotherapy and ADA plus MTX would appear similar because only patients who continued to do well on a given regimen would continue therapy for the full 24 months, and that therefore evaluations limited to patients receiving continuous therapy may underestimate the contribution of concomitant therapy. In addition, patients receiving MTX could potentially have been receiving this therapy prior to initiation of ADA, and this prolonged treatment period might have obscured the effect of concomitant treatment in comparison to more recent initiation, which would be more likely to have an evident influence on effectiveness.
Effectiveness and safety assessments
Baseline evaluations included demographic characteristics, previous and concomitant therapy, measures of arthritis and psoriasis disease activity, including the presence of enthesitis and dactylitis as judged by the investigator, and type of joint involvement. Effectiveness evaluations included tender (TJC) and swollen joint counts (SJC) performed on 78 and 76 joints, respectively, and the Disease Activity Score-28 joints (DAS28), which has been shown to reflect disease activity in PsA12,13. Psoriasis was assessed by use of the target lesion score (TLS), which ranged from 0 (absent) to 15 (severe erythema, scaling, and infiltration), and body surface area (BSA) measurements. Safety evaluations included reports of adverse events by system organ class and preferred term, rates of treatment discontinuation, and the proportion of patients who continue therapy (drug survival). In German noninterventional studies, clinicians are asked to report adverse events considered likely to be related to therapy; other adverse events were generally not reported.
Statistical analyses
Statistical analyses were performed using SAS statistical software (version 9.2) except for Kaplan-Meier analyses for drug survival, which used the survival package in R (version 3.1.2). Descriptive statistics or frequencies were computed for all data as appropriate. Owing to the documentary design of the study, data were not available for all assessments, and thus the sample size differed among variables. Missing data were not imputed.
T tests were used to evaluate differences between mean values in outcomes for ADA monotherapy versus ADA plus MTX at month 24, chi-square tests were used to compare adverse event and withdrawal rates in these groups, and the log-rank test was used to evaluate differences between these groups in Kaplan-Meier analyses. Because the patient groups were heterogeneous and not matched with respect to confounding factors such as age, disease duration, and disease activity, stepwise multiple regression analysis was used to identify associations among relevant variables14,15. Stepwise regression analyses (forward selection and backward elimination) were performed on key outcome measures (change from month 0 to month 24 in DAS28, TJC, SJC, TLS, and BSA) using 36 explanatory variables (See Supplementary Information on statistical analyses, available online at jrheum.org) to determine possible associations between concomitant MTX therapy and patient outcomes.
RESULTS
Subjects
Of the 1455 patients who met the entry criteria, 296 (20.3%) displayed symptoms of axial involvement and 1159 (79.7%) did not. Both the axial and nonaxial groups had peripheral manifestations as indicated by mean SJC and TJC (Table 1). With the exception of axial involvement, there were no other obvious differences in baseline characteristics between patients with axial PsA and those with no axial involvement. Similar proportions in each group (about 55%) were treated with ADA monotherapy and the remainder with concomitant ADA and MTX. In patients receiving concomitant MTX, the mean MTX dose at baseline was 14.9 ± 3.9 mg/week (range 8–30) in the group with axial PsA and 15.9 ± 4.7 mg/week (range 3–30) in the group with no axial involvement. Baseline characteristics were generally well matched between treatment groups (Table 1), although patients receiving MTX were more likely to be treated with concomitant systemic glucocorticoids, and patients receiving monotherapy had more severe psoriasis as indicated by higher TLS and BSA values. The proportion of patients with polyarthritis at study entry was higher in the groups receiving concomitant MTX, and the proportion of patients with distal interphalangeal joint involvement was lower. In the group with no evidence of axial involvement, patients receiving monotherapy had higher TJC than patients receiving ADA plus MTX.
Baseline characteristics of patients with PsA in the adalimumab noninterventional study by axial involvement and use of concomitant MTX. Values are mean (SD) unless otherwise specified.
Therapeutic response
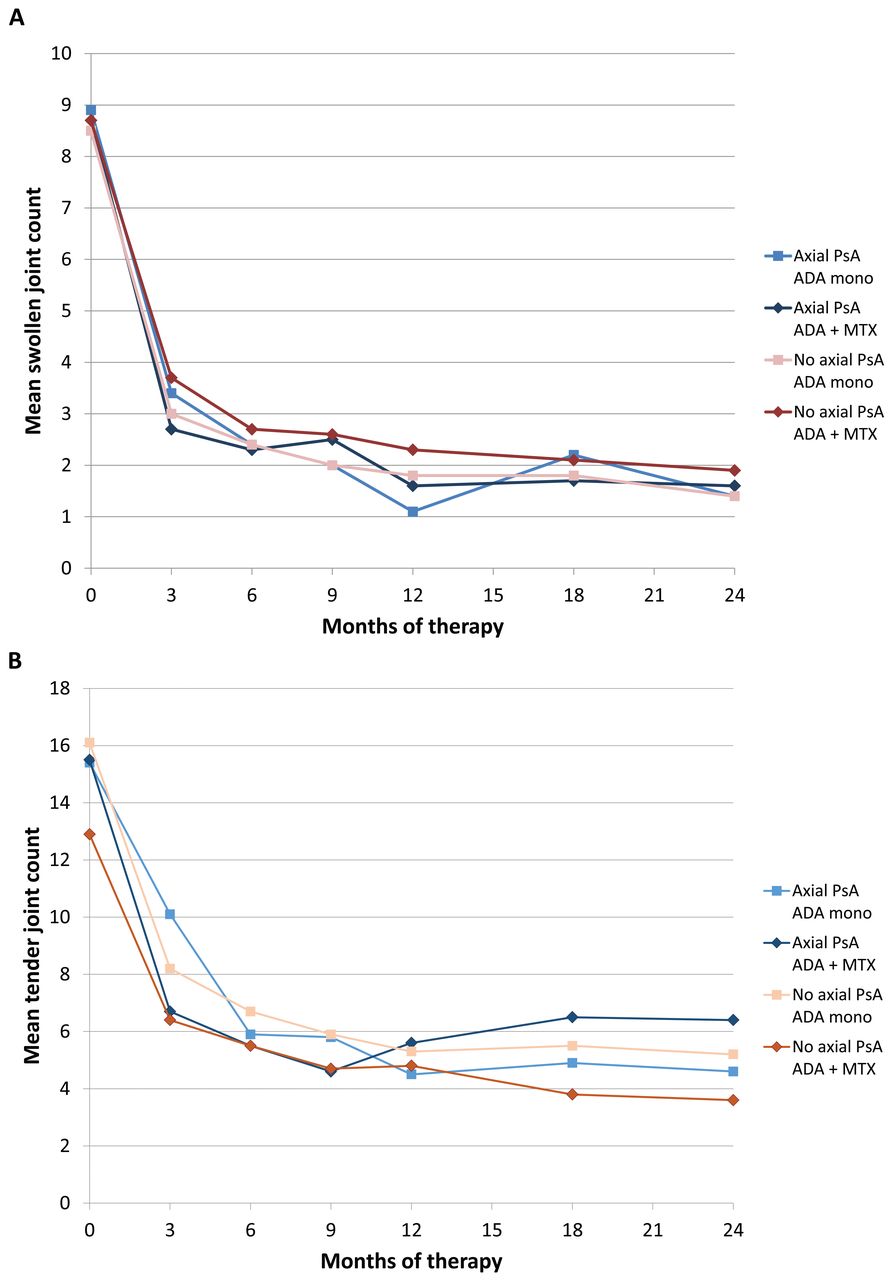
All subgroups showed rapid and sustained therapeutic responses to ADA therapy (Figure 1, and Supplementary Figure 1, available online at jrheum.org). The pattern and extent of response was similar regardless of the use of concomitant MTX. At month 24, patients with axial involvement showed no significant differences in key outcomes on the basis of MTX treatment, although psoriasis TLS approached significance (p = 0.062). Patients with no axial involvement showed a significant difference between ADA monotherapy and ADA plus MTX at Month 24 in TJC (p = 0.036) and TLS (p = 0.011). However, for both variables, baseline values in the group receiving monotherapy were higher than in the group receiving concomitant MTX. These increased baseline values were reflected throughout the course of therapy.
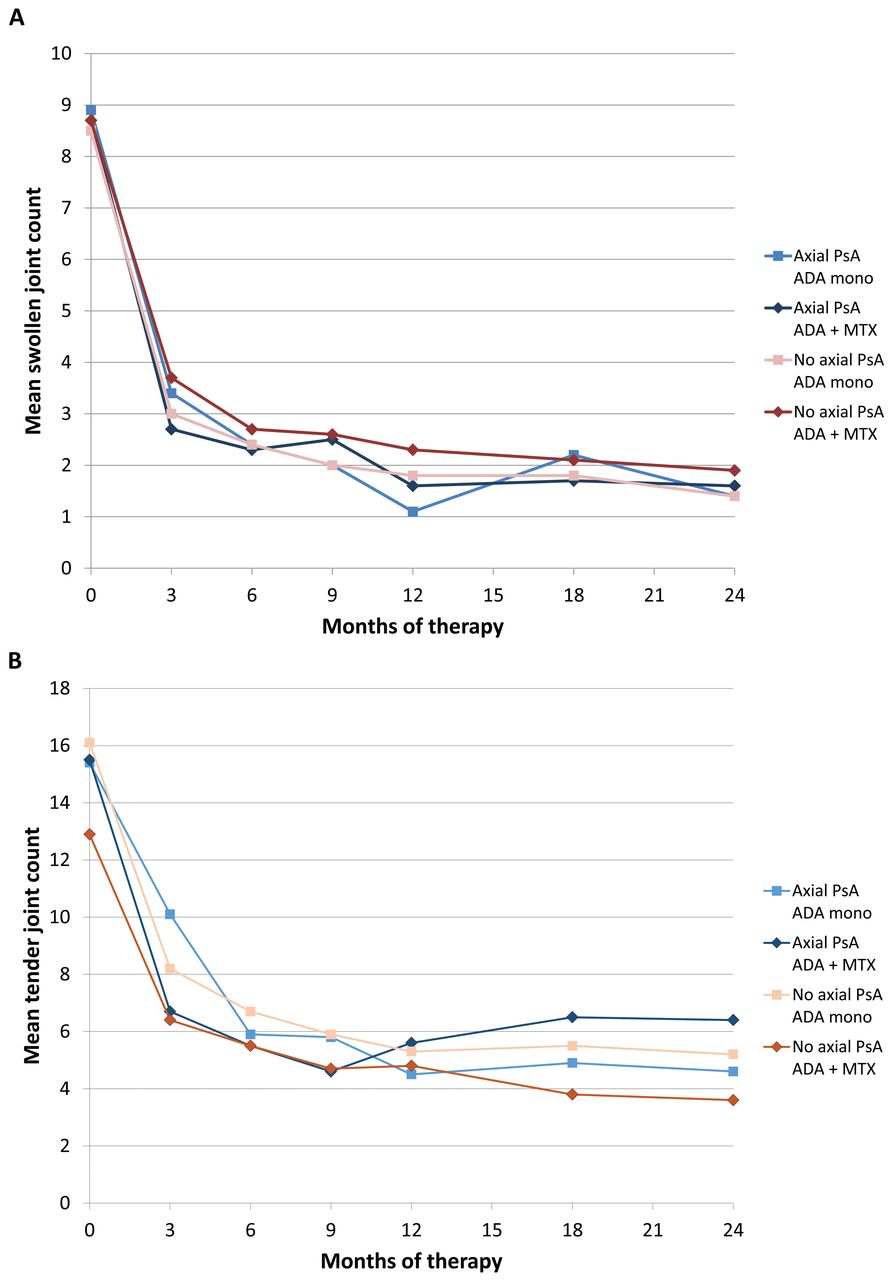
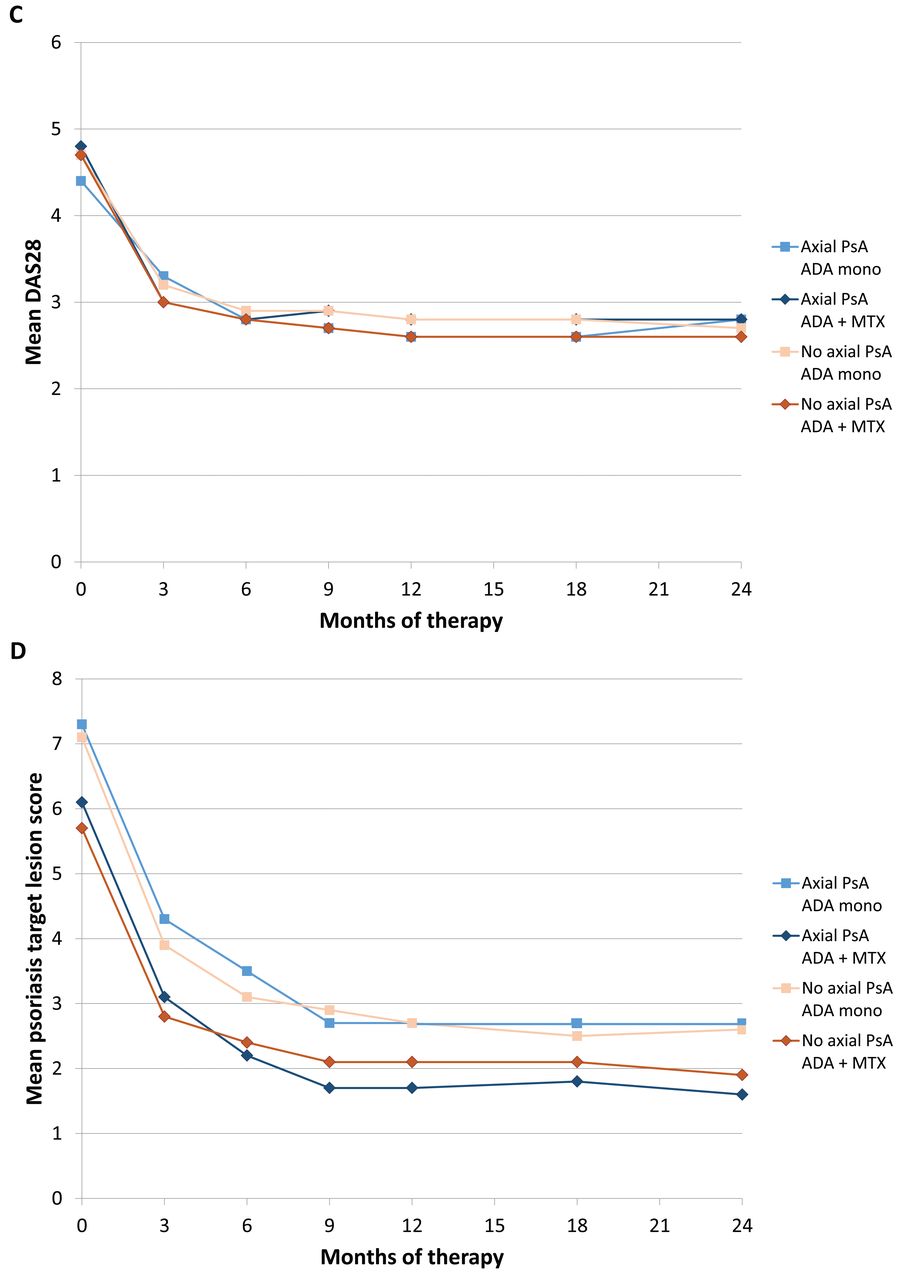
Response of patients with psoriatic arthritis (PsA) with axial involvement and those with no axial involvement to 24 months of adalimumab (ADA) therapy [monotherapy or plus methotrexate (MTX)] for the following outcomes: (A) mean swollen joint count; (B) mean tender joint count; (C) mean 28-joint Disease Activity Score (DAS28); (D) mean psoriasis target lesion score.
Because treatment groups showed potentially important differences in confounding factors, including baseline disease severity, comparisons of response patterns may be misleading. To provide a more statistically valid assessment of the influence of MTX on therapeutic response in this diverse patient population, multiple regression analyses were performed. As expected, baseline levels of most assessments showed an effect on outcomes (e.g., lower TLS levels at baseline were associated with lower TLS levels at 24 months). MTX treatment was not significantly associated with 24-month outcomes for any joint or skin assessment.
We considered the possibility that only patients who experienced satisfactory tolerability and effectiveness would continue therapy for 24 months, and that therefore the response curves of ADA monotherapy and ADA plus MTX would appear similar because of a differential dropout effect. To address this question, we analyzed clinical responses in patients who changed from ADA plus MTX to ADA monotherapy (33 patients in the group with axial PsA and 120 in the group with no axial involvement) or changed from ADA monotherapy to ADA plus MTX (21 and 59 patients, respectively) during the 24-month study (Table 2; data were not available for all patients at each timepoint). Treatment responses remained robust to changes in MTX comedication, although the numbers of patients were low for some subgroups.
Comparison of mean disease activity values after 24 months of treatment in patients with psoriatic arthritis (PsA) who changed therapy at least once and patients who did not.
Safety and treatment discontinuation
Concomitant MTX treatment was not associated with a statistically significant difference in adverse event rates compared with monotherapy [24.8% in the monotherapy group, 21.4% in the ADA plus MTX group for patients with axial involvement (p = 0.48); 16.3% in the monotherapy group and 17.4% in the ADA plus MTX group for patients with no axial involvement (p = 0.62)]. The most common adverse event by system organ class was infections and infestations [8.5% and 9.2% for axial PsA patients treated with monotherapy or concomitant MTX, respectively (p = 0.84); 4.7% and 5.6% for patients with no axial involvement treated with monotherapy and concomitant MTX (p = 0.50)]. No new safety signals were reported.
Treatment discontinuation and retention were evaluated as surrogate indicators of tolerability, safety, and effectiveness (Supplementary Table 1 and Supplementary Figure 2, available online at jrheum.org). Cumulative withdrawal over 24 months was higher in patients with axial involvement (32.7% for monotherapy and 32.1% for ADA plus MTX) than in those without axial involvement (24.0% for monotherapy and 24.4% for ADA plus MTX), but concomitant MTX did not have a significant effect on the rate of documented total withdrawals or on withdrawals for adverse events or lack of efficacy. In the groups with no axial PsA, a significant difference was observed in the proportion of patients with no withdrawal in the monotherapy subgroup (45.0%) compared with the combination therapy subgroup (53.1%; p = 0.006), but this finding can most likely be explained by a significantly higher proportion of patients lost to followup for unknown reasons in the monotherapy group (31.0% vs 22.6% for combination therapy; p = 0.001). In Kaplan-Meier analyses of drug survival, the proportion of patients continuing therapy did not differ significantly between ADA monotherapy and ADA plus MTX for patients with axial involvement (p = 0.739) or for those with no axial involvement (p = 0.993; Supplementary Figure 2, available online at jrheum.org).
DISCUSSION
We investigated the influence of concomitant MTX on the effectiveness of ADA in patients with PsA. A randomized trial found that MTX monotherapy did not improve joint counts or other measures of articular disease activity in patients with PsA compared with placebo5, suggesting that MTX alone may have minimal clinical effects in this patient population. However, the influence of MTX in combination with TNF inhibitors has not been well studied in PsA4. A study based on observational data from Norway did not detect a difference in clinical responses with the concomitant use of MTX and TNF inhibitors, but the authors stressed that they did not have the data to address the issue of peripheral versus axial disease, a major potential confounding factor8.
We used the clinician’s assessment of axial involvement at baseline to form subgroups consisting of patients with symptoms of axial involvement or with no clinical evidence of axial involvement by treatment group (ADA monotherapy or ADA plus MTX). All subgroups had signs of peripheral involvement as shown by mean joint counts at baseline. Subgroups were generally well matched with respect to baseline demographic and disease characteristics, but patients receiving ADA monotherapy had more severe skin disease at baseline than patients receiving ADA plus MTX. In the subgroup with no axial manifestations, patients treated with ADA monotherapy had a higher mean TJC at baseline compared with patients receiving combination therapy.
All subgroups showed rapid and sustained responses to ADA monotherapy or to ADA plus MTX. Although the addition of MTX to ADA therapy resulted in significant improvements in TJC and TLS at Month 24 in patients with no axial involvement as assessed by T tests, this finding was not confirmed by regression analyses. Both these variables showed discrepancies at baseline (lower mean levels in the ADA plus MTX subgroup), which likely acted as confounding factors in T tests of significance. Our study provides a strong example of the importance of using regression analyses in populations with multiple confounding variables. Regression analyses minimize the effects of confounding variables and thus represent a more accurate method of assessing the influence of an individual factor on clinical outcomes that are affected by multiple variables14,15.
On the basis of regression analyses, we conclude that in patients with PsA who start ADA therapy, concomitant MTX does not influence joint or skin outcomes in patients with axial manifestations or those with no axial manifestations. This finding was further confirmed by an analysis of patients who changed therapy (added or discontinued MTX) during the observation period. Alterations in therapy had no obvious effect on response to therapy, indicating that the lack of difference in outcomes between ADA monotherapy and ADA plus MTX was not due to a differential dropout effect.
Because of the noninterventional design of the study, reasons for changing the treatment regimen by either adding MTX to ADA monotherapy or by discontinuing it after an initial combination therapy remain elusive. However, our data suggest that the addition of MTX to ADA monotherapy may have been influenced by a less favorable response in joint disease in a subset of patients as shown by a lower degree of change in DAS28 at 24 months compared with patients who continued monotherapy. On the other hand, a good treatment response (a higher mean DAS28 reduction) may have facilitated the decision to taper MTX in a subgroup of patients receiving initial combination therapy. This association of treatment change with DAS28 improvement was detectable in patients with axial as well as those with nonaxial disease, whereas outcomes in skin involvement did not show a consistent pattern among subgroups. However, irrespective of the reasons for changing concomitant therapy, the addition or tapering of MTX was not associated with a clear effect on skin or articular outcomes.
Safety outcomes were also comparable among subgroups. To further analyze drug tolerability, we examined withdrawal rates during the 24 months of therapy. Other studies in patients with PsA have found that MTX increases the rate of persistence with anti-TNF therapy6,7,8 and that PsA patients treated with ADA plus MTX have higher serum concentrations of ADA than those treated with ADA alone16,17, possibly due to suppression of development of anti-ADA antibody. However, our findings do not support an increased rate of treatment persistence with ADA in patients receiving concomitant MTX. Patients with axial PsA showed higher rates of withdrawal than patients with no axial PsA, but the use of MTX did not influence the rates of documented withdrawal, the rates of withdrawal due to adverse events or lack of efficacy, or drug survival as assessed by Kaplan-Meier analyses. However, 22.6% to 31.0% of patients were lost to followup during the study. This large group who left the study without a documented reason appeared to influence the rate of treatment retention in the monotherapy subgroup of patients with no axial PsA, which was significantly lower than treatment retention in the combination therapy group. Although it is possible that the greater proportion of patients lost to followup in the monotherapy group was due to treatment failure or intolerance, we consider this unlikely, because withdrawals specifically attributed to lack of efficacy or adverse events were somewhat lower in the monotherapy compared to the combination therapy group. Based on our experience with noninterventional studies, we believe that the discrepancy in the proportion of patients lost to followup is more likely to be a random outcome unrelated to treatment.
Our study has some important limitations. As with all noninterventional studies, patients were not randomly assigned to the 2 treatment groups, and therefore between-group comparisons are inevitably affected by confounding variables. The categorization of axial involvement was done on the basis of clinical examination by the treating physician; imaging was not required to confirm the diagnosis. Adverse event reporting was limited to those events believed to be related to treatment and no specific evaluations of potential MTX-related toxicities were conducted. Further, the rates of patients who withdrew from the study or were lost to followup during the 24-month period were relatively high. As a result, some of the subgroups examined at 24 months had fairly small numbers of patients.
Our evaluations show that ADA is an effective option for patients with PsA with symptoms of axial involvement and for those with no symptoms of axial involvement. The addition of MTX to ADA does not improve articular or skin outcomes in patients with PsA compared with ADA monotherapy, regardless of axial disease status. Although ADA was the only TNF inhibitor used in this study, we consider it likely that this finding will apply to concomitant therapy with MTX and other anti-TNF agents. Other studies have suggested that concomitant MTX therapy may improve skin outcomes5,18. Our regression analyses did not show an association between MTX use and improvements in skin assessments, but it is notable that the patients who were receiving MTX at baseline did have less severe skin disease (lower TLS and BSA) at baseline. However, compared with patients receiving concomitant MTX, the monotherapy group showed numerically greater improvements in skin disease outcomes over 24 months. Given the known risks associated with MTX therapy, including gastrointestinal effects and hepatotoxicity19, clinicians may wish to consider the use of biologic monotherapy to manage patients with PsA.
ONLINE SUPPLEMENT
Supplementary data for this article are available online at jrheum.org.
Acknowledgment
We thank Sharon L. Cross, PhD, for medical writing services on behalf of CIRI, Frankfurt am Main, Germany, under contract with AbbVie for medical writing services.
Footnotes
Full Release Article. For details see Reprints/Permissions at jrheum.org
Supported by AbbVie Deutschland GmbH and Co. KG (formerly Abbott GmbH and Co. KG).
Dr. Behrens, Dr. Koehm, Dr. Arndt, Dr. Thaçi, Dr. Scharbatke, Dr. Tony, and Dr. Burkhardt have received speaker’s fees, research funding, or compensation for consultancies or board memberships from AbbVie Deutschland GmbH and Co. KG (formerly Abbott GmbH and Co. KG).
- Accepted for publication September 1, 2015.
Free online via JRheum Full Release option








{kind=link}
{kind=link}