

Abstract
Objective. Discrimination of diffuse idiopathic skeletal hyperostosis (DISH) and ankylosing spondylitis (AS) can be challenging. Usefulness of whole-body magnetic resonance imaging (WB-MRI) in diagnosing spondyloarthritis has been recently proved. We assessed the value of clinical variables alone and in combination with WB-MRI to distinguish between DISH and AS.
Methods. Diagnostic case-control study: 33 patients with AS and 15 patients with DISH were included. All patients underwent 1.5 Tesla WB-MRI scanning. MR scans were read by a blinded radiologist using the Canadian-Danish Working Group’s recommendation. Imaging and clinical variables were identified using the bootstrap. The most important variables from MR and clinical history were assessed in a multivariate fashion resulting in 3 diagnostic models (MRI, clinical, and combined). The discriminative capacity was quantified using the area under the receiver-operating characteristic (ROC) curve. The strength of diagnostic variables was quantified with OR.
Results. Forty-eight patients provided 1545 positive findings (193 DISH/1352 AS). The final MR model contained upper anterior corner fat infiltration (32 DISH/181 AS), ankylosis on the vertebral endplate (4 DISH/60 AS), facet joint ankylosis (4 DISH/49 AS), sacroiliac joint edema (11 DISH/91 AS), sacroiliac joint fat infiltration (2 DISH/114 AS), sacroiliac joint ankylosis (2 DISH/119 AS); area under the ROC curve was 0.71, 95% CI 0.64–0.78. The final clinical model contained patient’s age and body mass index (area under the ROC curve 0.90, 95% CI 0.89–0.91). The full diagnostic model containing clinical and MR information had an area under the ROC curve of 0.93 (95% CI 0.92–0.95).
Conclusion. WB-MRI features can contribute to the correct diagnosis after a thorough conventional workup of patients with DISH and AS.
- MAGNETIC RESONANCE IMAGING
- DIFFUSE IDIOPATHIC SKELETAL HYPEROSTOSIS
- ANKYLOSING SPONDYLITIS
- SPONDYLOARTHROPATHY
- CASE-CONTROL STUDIES
Discriminating between cases of diffuse idiopathic skeletal hyperostosis (DISH) and ankylosing spondylitis (AS), also referred to as radiographic axial spondyloarthritis (SpA; fulfilling the modified New York criteria), can be challenging1. The usefulness of whole-body magnetic resonance imaging (WB-MRI) in diagnosing nonradiographic SpA and AS has been scientifically investigated in recent years2. Whereas findings in the WB-MRI reformed the classification criteria for SpA3 and became part of the new diagnosis of nonradiographic SpA, the Resnick criteria for DISH are still based on findings from conventional radiographs of the spine4. In clinical practice, later stages of the 2 illnesses may overlap both clinically and radiologically, because patients with back pain from an axial form of psoriatic arthritis (PsA) may present with coarse parasyndesmophytes and patients with back pain diagnosed with DISH may show hyperostotic excrescences on spine radiographs5,6. To make it even more complicated, both diseases may occur in the same patient, as 1 study showed7.
Because MRI is now broadly available in many countries, MRI findings of the sacroiliac joints (SIJ) became part of the new criteria introduced by the Assessment of Spondyloarthritis international Society (ASAS) in 20093. MRI will often be initiated in a diagnostic investigation of unspecified back pain because it may be difficult to differentiate between the various diseases of the spine, such as osteoarthritis, DISH, and SpA (AS), using clinical history and conventional radiographs alone. We are, however, unaware of any previous clinical study describing WB-MRI features in DISH and investigating their capacity to systematically distinguish patients with AS from patients with DISH. Therefore, in this diagnostic case-control study, we investigated the diagnostic accuracy of WB-MRI alone and in combination with clinical variables to discriminate between DISH and AS. Addressing this question in regard to an accurate diagnosis is clinically and economically important because the treatment of the 2 entities differs substantially.
MATERIALS AND METHODS
The local Ethics Committee approved the protocol of our study (#2004-37 and 2011-0193).
The study followed the current Standards of Reporting of Diagnostic Accuracy reporting guidelines8.
Study setting
In our cross-sectional study, we consecutively recruited patients with DISH according to the Resnick criteria4 from our rheumatology out-patient department of the Balgrist University Hospital between October 2011 and August 2013. Patients were mainly referred for a diagnostic investigation of unidentified back pain from family doctors, rheumatologists in private practices, and from the Department of Spine Surgery of our institution. All participating patients gave written informed consent prior to study inclusion.
Selection of patients with DISH
Patients over the age of 18 years with a case of DISH based on radiograph findings of the cervical, thoracic, or lumbar spine with partial or complete ossification of at least 4 adjacent vertebral bodies (Resnick criteria4) and an available radiograph of the pelvis were selected. Moreover, an experienced rheumatologist with extensive training in musculoskeletal rheumatology (BW) reviewed all radiographs and confirmed the diagnosis of DISH, carefully excluding those patients presenting with clinical signs or laboratory findings associated with other conditions, such as AS, phosphate diabetes, or longterm isotretinoin treatment9.
Clinical assessment of patients with DISH
Already existing radiographs of the pelvis and results from laboratory tests (i.e., thyroid stimulating hormone, uric acid blood level, HbA1c, cholesterol levels) were obtained because they represent potential risk factors for the development of DISH if pathologic. Moreover, height and weight were measured and information on the presence or absence of HLA-B27 and levels of indicators of inflammation such as C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) were obtained from chart reviews or by contacting the referring physicians. No extra laboratory tests or radiographs were performed. Finally, all patients with DISH underwent a complete clinical back pain assessment including location and duration of pain and the restriction of spinal movement in daily life (present/absent). A rheumatologist (BW) examined the range of motion of the spine using standardized measurements (Schober’s sign, lateral flexion, and cervical rotation). All data were collected in a standardized fashion and enrolled in a case report form designed ahead of our study.
Selection of patients with AS
We sampled patients with AS from our WB-MRI study with complete WB-MRI scans based on age (older than 45 yrs) and fulfillment of the modified New York criteria with and without syndesmophytes on conventional radiographs. All patients with AS included in our study had taken part in previous studies of our center and the collaborating centers10,11,12,13,14. WB-MRI features were assessed in patients classified as having AS by fulfilling the modified New York criteria and by clinical judgment. No selection was made for prior treatment.
Clinical assessment of patients with AS
Detailed clinical data were secured for all patients according to the Outcomes in Ankylosing Spondylitis International Study (OASIS) protocol15 including height, weight, sex, age, inflammation signs (CRP, ESR), HLA-B27 status, the type of AS (primitive, secondary to PsA, Crohn disease, ulcerative colitis), duration of symptoms, range of motion (Bath Ankylosing Spondylitis Metrology Index), patient-reported pain (Bath Ankylosing Spondylitis Disease Activity Index), function (Bath Ankylosing Spondylitis Functional Index), and medical treatment.
In addition to conventional radiographs of the pelvis, radiographs of the lumbar and cervical spine and WB-MRI were obtained. Clinical examination and WB-MRI were performed on the same day.
All data were collected in a standardized fashion and enrolled in a case report form designed ahead of our study.
Exclusion criteria
We excluded patients with AS and DISH with known contraindications for MRI such as pregnancy, pacemaker or vascular clips, or severe claustrophobia. The timepoint with the most complete clinical and radiographic data was selected for inclusion when more than 1 WB-MRI (3 patients) was available.
WB-MRI scan protocol
The WB-MRI scan protocols had previously been validated12 and were approved by 2 experienced radiologists (CP, VZ). The WB-MRI studies were acquired using a MAGNETOM Avanto 1.5 TL MRI scanner (Siemens Medical Solutions). WB-MRI is an MRI of the entire spine with sagittal short-tau inversion recovery (STIR) and T1 SE sequence images as well as MRI of the SIJ with coronal and optional axial STIR and T1 SE sequence images. The detailed WB-MRI protocol has been previously described10.
WB-MRI scoring
All WB-MRI images were scored according to the Canadian-Danish scoring system16 by 1 experienced radiologist (VZ) with extensive training in musculoskeletal radiology who was blinded to patient data and diagnosis. The MR images were evaluated in a random order on an electronic working station of our institution. A data sheet with a selection of scoring items based on the Canadian-Danish scoring system for each patient had been designed previously. Scoring was based on the following items: u-aCIL/LIL (upper anterior corner/lateral inflammatory lesion), u-pCIL/LIL (upper posterior corner/LIL), l-aCIL/LIL (lower anterior corner/LIL), l-pCIL/LIL (lower posterior corner/LIL), u-aFAT (upper anterior corner fat infiltration), u-pFAT (upper posterior corner FAT), l-aFAT (lower anterior corner FAT), l-pFAT (lower posterior corner FAT), NANK (ankylosis vertebral endplate not at the anterior or posterior vertebral corner), NIL (non corner inflammatory lesion), PIL (posterior element IL), FIL (facet joint IL), FANK (facet joint ankylosis), r-sup iliac (right superior iliac) SIJ, r-inf iliac (right inferior iliac) SIJ, r-sup sacral (right superior sacral) SIJ, r-inf sacral (right inferior sacral) SIJ, l-sup iliac (left superior iliac) SIJ, l-inf iliac (left inferior iliac) SIJ, l-sup sacral (left superior sacral) SIJ, l-inf sacral (left inferior sacral) SIJ, and all 8 items of the SIJ were scored for edema, fat infiltration, ankylosis, and ankylosis of the manubrium.
Statistical analysis
Diagnostic variables of WB-MRI and clinical history were identified using a bootstrapping procedure in which presence of AS was considered the dependent variate. Bootstrapping of a stepwise forward procedure was repeated 100 times and the number of times each variable was selected in each of the bootstrapping cycles was counted. By using this procedure, we counteracted possible idiosyncrasies of the underlying data and reduced the risk that a variable was considered important by chance alone. The most important variables, i.e., those chosen in at least 50 out of 100 bootstrapping cycles from WB-MRI and clinical history, were then assessed in multivariate fashion, resulting in 3 diagnostic models: MRI, clinical, and combined. The discriminative capacity was quantified using the area under the receiver-operating characteristic (ROC) curve. The strength of diagnostic variables was quantified with OR.
RESULTS
Patient selection
Of the 53 initially screened participants (35 AS, 18 DISH), 5 fulfilled the exclusion criteria. Two initially included patients with DISH (1 man, 1 woman) were excluded because of equivocal spinal and pelvic radiographs, making the DISH diagnosis doubtful. In total, we excluded 3 patients with DISH.
Two patients with AS were excluded: 1 because of a lack of clinical data and 1 for being aged under 45 years. The study sample thus contained 48 patients (33 AS, 15 DISH).
Patient description
Score values of MRI readings of 48 patients provided 1680 MR readings with 1545 positive features (193 DISH/1352 AS).
The median number of positive MRI signs among patients with AS was 36 [interquartile range (IQR) 14–54, range 8–131]. Among patients with DISH, the median number of positive signs was 11 (IQR 6–15, range 3–61). The exact number of positive items according to the described Canadian-Danish scoring system comparing patients with DISH and AS are summarized in Table 1.
WB-MRI features in DISH (n = 15) and AS (n = 33) according to the Canadian-Danish scoring system in defined regions of the spine and anterior chest wall. Values are n/n (DISH/AS found on WB-MRI).
Clinical information
The age of patients with DISH ranged from 42.8 to 85.3 years (average 65.9 yrs, median 64.5 yrs). Of the 15 patients with DISH, 9 were men and 6 were women. The CRP levels (mg/l, < 5) ranged from 0–13 mg/l (median 3.5), the body mass index (BMI) was between 22.5 and 43.9 kg/m2 (median 28.7), and symptom duration was between 1 and 40 years (median 10 yrs). This shows that all of them had back pain at the time of the WB-MRI, all of them had at least 1 feature of a metabolic syndrome (over-weight/obesity, hypercholesterolemia, diabetes, hypertension, hyperuricemia), 12 out of 15 were HLA-B27–negative, and 3 had not been investigated.
The age of patients with AS ranged from 45 to 72 years (average 53.3 yrs, median 51.7 yrs). Of the 33 patients, 25 were men and 8 were women. The CRP levels (< 5 mg/l) ranged from 0 to 90 mg/l (median 8), the BMI was between 17.8 and 38.8 kg/m2 (median 26), and symptom duration was 6–41 years (median 28 yrs). Twenty-six patients were HLA-B27–positive, 7 were HLA-B27–negative, 27 were diagnosed with AS, 2 with AS secondary to PsA, and 4 with AS secondary to Crohn disease. Nineteen out of 33 had syndesmophytes on conventional radiographs at the time of the WB-MRI. Six out of 33 patients were receiving antitumor necrosis factor (anti-TNF) treatment when they had the WB-MRI, and 27 patients were naive to anti-TNF. Twenty-two out of the 27 patients were receiving nonsteroidal antiinflammatory drugs (NSAID) at the time of WB-MRI, 4 patients took NSAID in combination with sulfasalazine, and 1 patient had no drug treatment. The complete clinical and demographic characteristics of both groups are shown in the Supplementary Tables 1–4 (available online at jrheum.org), as well as in Table 1 with the detailed WB-MRI findings for DISH and AS.
Diagnostic models
The final MR model contained 6 variables [u-aFAT, OR 2.86, 95% CI 1.13–7.25, p = 0.026; NANK, OR 4.41, 95% CI 0.79–24.54, p = 0.09; FANK, OR 8.68, 95% CI 0.96–78.55, p = 0.05; SIJ edema (SIJe), OR 4.41, 95% CI 1.95–9.99, p < 0.001; SIJ fat infiltration (SIJfi), OR 9.45, 95% CI 1.11–80.50, p = 0.04; and SIJ ankylosis (SIJa), OR 16.30, 95% CI 2.04–130.35, p = 0.008]. The corresponding area under the ROC curve was 0.71 (95% CI 0.64–0.78; Figure 1).

Area under the receiver-operating characteristic curve for magnetic resonance variables.
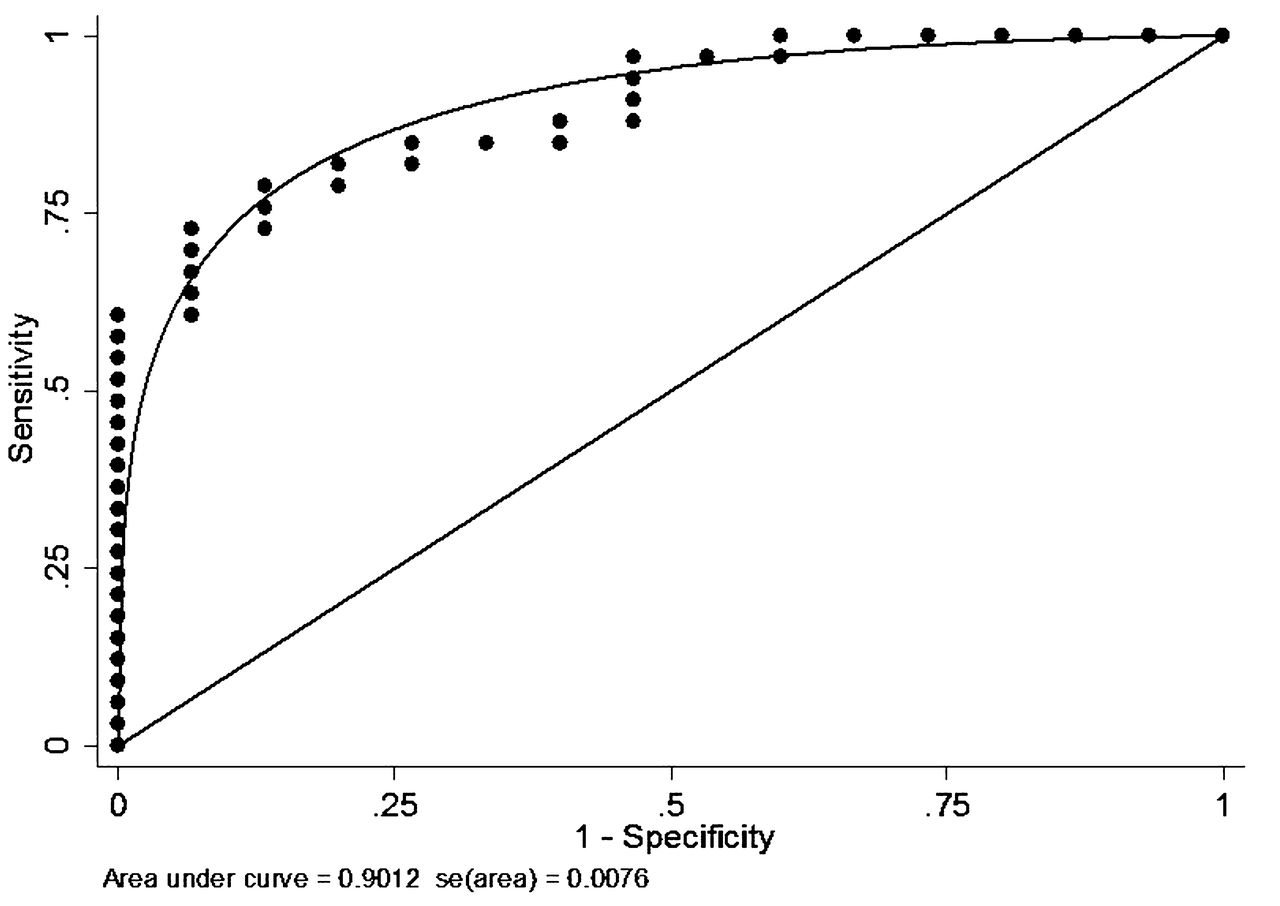
The final model containing only clinical information was based on patient’s age (OR 0.83, 95% CI 0.76–0.91, p < 0.001) and BMI (OR 0.79, 95% CI 0.67–0.93, p = 0.005), and the corresponding area under the ROC curve was 0.90 (95% CI 0.89–0.91; Figure 2).
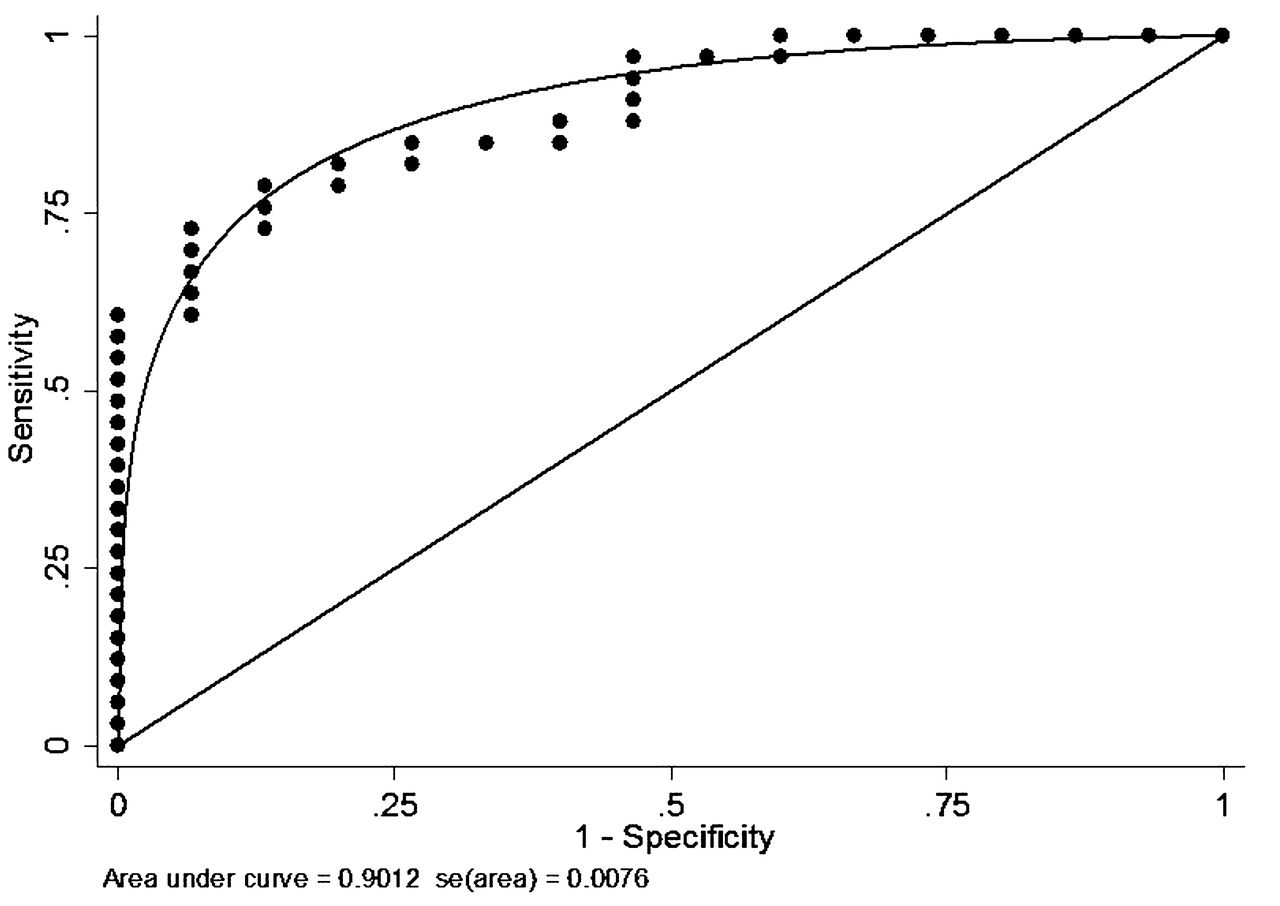
Area under the receiver-operating characteristic curve for clinical information (age, body mass index).
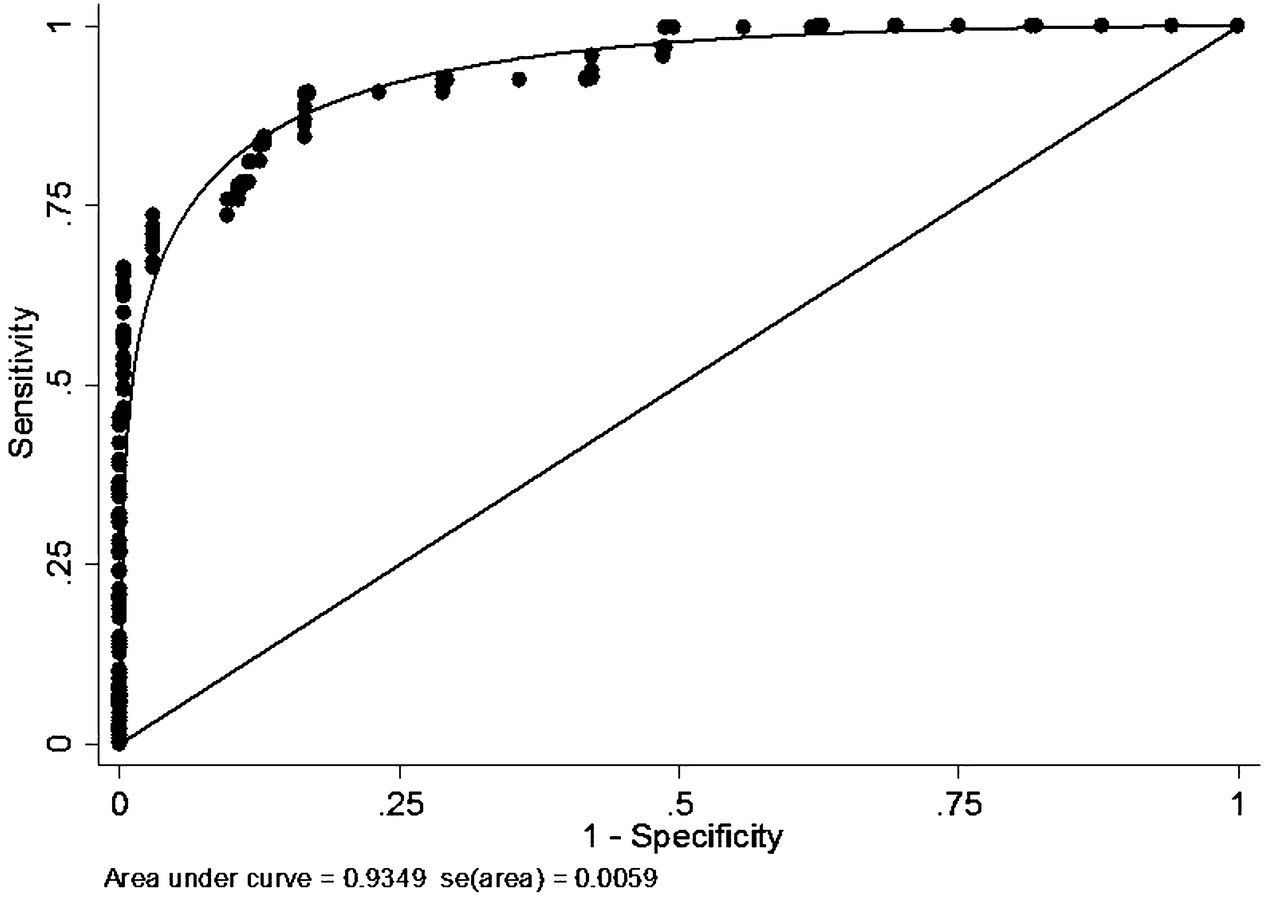
The full diagnostic model containing clinical and MR information had an area under the ROC curve of 0.93 (95% CI 0.92–0.95; Figure 3).
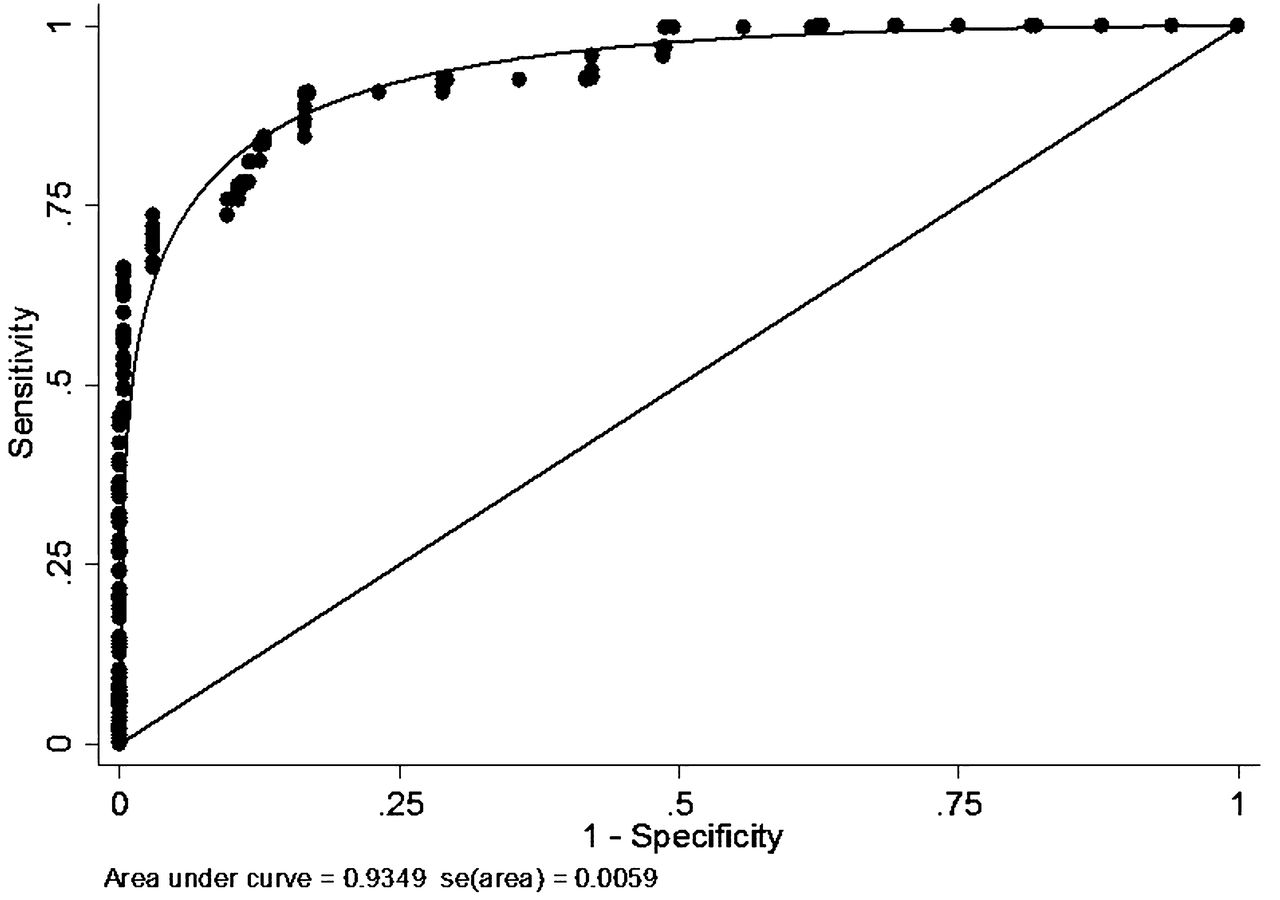
Area under the receiver-operating characteristic curve combined.
Estimated probabilities
Table 2 outlines the probability of AS given a certain set of positive MR scores. The range of probabilities was from 59.5% to 99.9%. The estimated probabilities of AS presence of the combined model were 2.1% to 100%. The estimated probability range for AS presence of the clinical model was 5.7% to 99.6%. Young patients with low BMI had a higher likelihood of AS presence than elderly patients with increased BMI.
Probability of ankylosing spondylitis given a certain set of positive magnetic resonance scores. Values are n.
DISCUSSION
Main findings
The combination of results from WB-MRI readings in conjunction with clinical information (BMI, age) leads to an excellent discrimination between patients with DISH and patients with AS. MRI features showing the best discrimination of DISH and AS included ankylosis [non corner ankylosis (4 DISH/60 AS), facet joint ankylosis (4 DISH/49 AS), SIJa (2 DISH/119 AS) besides alterations of the SIJ such as edema (10 DISH/91 AS) and fat infiltration (2 DISH/114 AS)], and upper corner fat infiltration of the spine (32 DISH/181 AS). Generally, the number of items found in the WB-MRI of patients with AS by far exceeded the number found in patients with DISH (median 36 AS/11 DISH).
Results in the context of the existing literature
Our description of the MRI features DISH compared with AS and the diagnostic model assist clinicians in the clinical investigations of the 2 conditions. In accordance with previous papers, the specific fat infiltration of the SIJ (with distinct border and homogeneity)13 as well as the ankylosis of the synovial part of the SIJ of patients with AS are not normally found in patients with DISH17. Edema of the SIJ is uncommon in DISH, but if present manifests mainly in the upper sacral and iliac part (Supplementary Data available online at jrheum.org). Acute upper anterior corner inflammatory lesions of the spine are found in the WB-MRI of patients with AS and DISH, and according to our results do not discriminate between DISH and AS (Figure 4; Supplementary Data available online at jrheum.org). This finding is in agreement with a recent study of the incremental diagnostic value of spinal MRI compared to MRI of SIJ alone in different study groups. According to this study, CIL was also found in patients with nonspecific back pain as well as in healthy controls18. In a more descriptive way, Table 1 and Supplementary Table 3 (available online at jrheum.org) also suggest that posterior acute inflammatory or fatty lesions in the thoracic spine and posterior element inflammatory lesions as well as facet joint ankylosis in the thoracic spine are not normally found in patients with DISH. In patients with AS, these positive findings tend to be localized in the middle and lower part of the thoracic spine (Th5–Th8, Th9–Th12). This is also in accordance with a paper investigating the inflammatory lesions of the posterior element of the spine with MRI in patients with active AS19.

Diffuse idiopathic skeletal hyperostosis, short-tau inversion recovery sequence. Arrows indicate bone marrow edema on the upper anterior vertebral corners.
Not surprisingly, regarding the existing literature, our final clinical model for DISH consists of age and BMI20. Interestingly, all patients with DISH in our study had back pain at the time of the WB-MRI. Although we cannot exclude that our tertiary referral center sees selected patients with more disabling disease (back pain) than in private practice, there is valid evidence in the literature that DISH can be associated with back pain and postural abnormalities, even mimicking AS5,21. Nevertheless, our results have to be interpreted cautiously in patients with DISH without clinical symptoms.
Strengths and limitations
The strengths of our study include a structured consecutive patient inclusion with defined outcome measures, the standardized execution of the WB-MRI using an established protocol, and the completeness of extensive clinical data for both patient groups11. We designed our DISH/AS study in accordance with WB-MRI studies in AS, using physician expert opinion in evaluating conventional radiographs and in clinical assessment with application of established diagnostic criteria (Resnick criteria, Modified New York criteria) for the classification of DISH and AS. To meet the challenge of differences in the distribution of variables between the group of patients with AS and DISH, we restricted the age of patients with AS to > 45 years, making allowance for the older age of the patients with DISH. We also corrected for differences in the age and sex distribution between the 2 groups statistically using multivariate analyses.
Moreover, the use of a structured data sheet to assess the MRI findings according to the Canadian-Danish recommendations and the reading by an experienced radiologist trained to work with this system14 are assets of our study.
There are, however, some limitations. Whereas study variables in AS are well established (OASIS or the SpondyloArthritis Research Consortium of Canada protocols), no standardized protocol for studies of DISH currently exists. We therefore established a protocol in analogy to the protocol for AS, collecting clinical, radiographic, and laboratory data. Second, the sample size was rather small and the MRI scans were not assessed in duplicate. However, previous studies of our group in collaboration with other centers showed a very good intraobserver reliability of the radiologist (ZV) assessing MR scans with the Canadian-Danish scoring system, also used in our study13,14,22. Previous MR studies from the Canadian Group evaluating the scoring system used in our paper also showed excellent intraobserver reliability, especially for radiologists23,24. Finally, the classification of DISH and AS was based on physicians’ expert opinion. Clinician expert opinion has also been the accepted gold standard for deriving 3 sets of classification criteria over the past 2 decades (Amor, European Spondylarthropathy Study Group, ASAS criteria). However, misclassifications cannot fully be ruled out. It is possible that 1 patient (No. 4 DISH, Supplementary Table 1, available online at jrheum.org) had 2 conditions, which according to the literature may coexist in the same patient: DISH and SpA without fulfilling the modified New York criteria. Although we followed the described stringent inclusion criteria, we cannot rule out that this patient was misclassified.
Implications for research
Replication of our study confirming the findings in a new set of patients would be useful. Although combined MRI and clinical findings appear to distinguish very well between AS and DISH, further studies should assess whether the high yield of discrimination reported in our study remains when assessing patients with AS secondary to PsA. These patients typically tend to be older and are more prone to metabolic diseases than patients with AS25. Although 6 of our patients with AS either had AS secondary to PsA or secondary to inflammatory bowel disease (Crohn disease, ulcerative colitis), we were unable to address this issue in a subgroup analysis.
Implications for practice
Previous research and clinical practice show that DISH typically develops in patients with a metabolic syndrome (obesity, arterial hypertension, Type 2 diabetes, hypercholesterolemia, and hyperuricemia26) and is more common in elderly men, showing signs of inflamed entheses (enthesitis)27. On the other hand, nonradiographic SpA and radiographic axial SpA (AS) tend to affect younger persons and are highly linked to HLA-B27 positivity, and patients show radiologic features of systemic inflammation. Both entities share the presence of enthesitis and male preponderance28. Moreover, both diseases show new bone formation in a slow process29.
Because some of our described MRI criteria differentiating the 2 diseases (ankylosis of facet joints, SIJa) also confirm the diagnostic classification criteria of Resnick (relative preservation of disc height, absence of extensive degenerative disc disease, absence of apophyseal joint bony ankylosis, and absence of sacroiliac erosion, sclerosis, or bony fusion), performing a thorough clinical and radiographic examination by conventional radiographs as the first step in a diagnostic process is recommended. Ankylosis of the SIJ might be seen in the upper (ligamentous) portion of the joint, and an ossification of the joint capsule on the anterior surface of the joint in the lower two-thirds (synovial part) sometimes leads to misinterpretation17,30.
Our diagnostic case-control study comparing WB-MRI findings in patients with DISH to WB-MRI findings in patients with AS also showed several WB-MRI features occurring in both patient groups such as aCIL/LIL, aFAT in the whole spine as well as pCIL/LIL, and pFAT in the lumbar spine (Table 1).
It should also be kept in mind that this is a diagnostic case-control study with a small patient group (DISH/AS: 15/33) whose results need to be treated with caution and should be confirmed in a larger study.
When discrimination between DISH and AS remains unclear after a thorough conventional investigation, these WB-MRI features may contribute to the correct diagnosis: edema of the lower part of the SIJ in patients with AS and absence of acute or chronic posterior inflammation and of the posterior element as well as facet joint ankylosis in the thoracic spine of patients with DISH.
To our knowledge, this is the first cross-sectional study that investigates MRI and clinical features of DISH in comparison with AS, and describes the most discriminating MRI (u-afat, NANK, FANK, SIJe, fat infiltration, ankylosis) and clinical findings. This first description of WB-MRI features differentiating between DISH and AS may contribute to finding the right diagnosis in difficult cases in which a thorough conventional investigation has not yielded an unequivocal diagnosis.
ONLINE SUPPLEMENT
Supplementary data for this article are available online at jrheum.org.
Acknowledgment
We thank all Swiss rheumatologists, internists, and primary care physicians for referring their patients and all the patients who participated in our study. The authors thank F. Brunner, MD, PhD, for his support of our study.
Footnotes
Funded by the Walter L. and Johanna Wolf Foundation, Zurich, Switzerland, and the Foundation for Scientific Research at the University of Zurich, Switzerland.
- Accepted for publication October 6, 2015.








{kind=link}
{kind=link}
{kind=link}
{kind=link}