

Abstract
Objective. To investigate the longterm association of a wide range of comorbidities with physical and mental functioning in patients with rheumatoid arthritis (RA).
Methods. Longitudinal data over a period of 11 years were collected from 882 patients with RA. Somatic comorbidity and comorbid depression were measured at baseline, with a questionnaire including 20 chronic diseases and with the Center for Epidemiologic Depression Scale, respectively. Physical functioning was measured at 5 timepoints with a disease-specific measure [Health Assessment Questionnaire (HAQ)] and a generic measure [physical scales of the Medical Outcomes Study Short Form-36 (SF-36)]. Mental functioning was measured with the mental scales of the SF-36. To determine the association of baseline-specific comorbidities with functioning over time, we performed longitudinal analyses.
Results. At baseline, 72% percent of the patients were women, mean age ± SD was 59.3 ± 14.8 years, median RA disease duration was 5.0 years, and 68% had ≥ 1 comorbid condition. The effect of comorbid conditions was more apparent when physical functioning was measured with SF-36, a disease-generic measure, compared with the HAQ, a disease-specific measure. Circulatory conditions and depression were associated (p < 0.05) with worse physical functioning according to the HAQ. Respiratory conditions, musculoskeletal conditions, cancer, and depression were associated (p < 0.05) with worse physical functioning according to the SF-36. Respiratory conditions and depression were associated with worse mental functioning.
Conclusion. Patients with specific comorbid conditions have an increased risk of low functioning in the long term. Targeted attention for these specific comorbid conditions by clinicians is recommended.
Comorbidity, defined as any additional, coexistent condition in a patient with a particular index disease1, is highly prevalent2 in patients with rheumatoid arthritis (RA) and is involved in determining RA-related outcomes3. Several studies have reported the negative association of somatic comorbidity with physical functioning3,4,5. Somatic comorbidity is, even after 10 years, associated with worse physical functioning and contributes over time to decline in physical functioning2,3,6. The effect of somatic comorbidity on mental functioning is less well known. Comorbid depression is associated with low physical functioning6,7 and mental functioning8,9.
In most studies, comorbidity is measured with a dichotomous6 score, a sum score3, or an index score10,11. In clinical practice, a clinician needs to determine the prognosis of individual patients with specific comorbidities. Evaluating specific comorbidities provides valuable prognostic information about which patients have a higher risk for worse functioning in the long term, and treatments could be adjusted accordingly. Therefore, knowledge is required of the effect of baseline comorbidity on functioning12.
The effects of specific comorbidities on physical and mental functioning will be different. It may be expected that different chronic diseases show varying effects on physical functioning, but do not differ much in their effect on mental functioning because the adaptation process of chronic diseases is comparable13. Few studies have investigated the effect of a specific comorbid condition on physical functioning14,15. To our knowledge, the effect of specific comorbidities on mental functioning has not yet been investigated. Chronic diseases often have a course of slow decline, and therefore it is expected that the effect of comorbidity will be clearer over the longer term. A longtime horizon is needed to investigate which specific comorbidities are associated with worse physical and mental functioning over time.
Therefore, the aim of our study was to investigate the association of a wide range of comorbidities with physical and mental functioning during 11 years of followup in patients with RA. Research questions consisted of (1) which specific comorbidities were associated with low physical functioning, and (2) which specific comorbidities were associated with low mental functioning. More insights into the effect of comorbidity will contribute to optimizing the medical management of patients with RA.
MATERIALS AND METHODS
Study design and population
In 1997, our research group started a longitudinal study on comorbidity and health outcomes in patients with RA16. A sample of 1251 patients was randomly selected from the register of a large rheumatology outpatient clinic in Amsterdam, which included the patients from 7 allied outpatient clinics. For inclusion in the study, patients had to fulfill the following eligibility criteria: (1) a diagnosis of RA according to the American College of Rheumatology criteria for RA, (2) 16 years of age or older, (3) adequate knowledge of the Dutch language, and (4) at least 1 visit to a rheumatologist in the previous 2 years.
Data were collected in 1997, 1998, 1999, 2002, and 2008 by means of self-administered questionnaires. The questionnaires consisted of questions about sociodemographic characteristics (age, sex, educational level, and employment status), clinical characteristics (including comorbidity), and health characteristics (including physical and mental functioning). Information on RA disease duration was retrieved from the patients’ medical records, and disease activity was assessed during clinical examination. In addition, we established whether participants had died during the period 1996–2011 from the mortality register of the Statistics Netherlands17.
Demographic and clinical variables
The sociodemographic variables included age, sex, and socioeconomic status (SES). SES was indicated by educational level. We divided SES into 3 categories: low SES (no education or education at the primary school level), medium SES (education at the secondary school level), and high SES (college or university level education).
Disease activity was assessed by means of the Disease Activity Score (DAS) in 28 joints, scoring separately swelling and tenderness of 28 joints (and without using the visual analog scale for general health assessment).
Physical and mental functioning
Physical functioning was measured with the validated Dutch version of the Health Assessment Questionnaire (HAQ), a disease-specific measure of physical functioning. The HAQ category score was raised when aids or devices were indicated by the patient. In addition, physical functioning was measured with the physical functioning scales of the Dutch version of the RAND-3618. This is a generic measure of physical functioning, meaning that its concepts are not specific to any disease or treatment group19. Mental functioning was measured with the mental scales of the Dutch version of the RAND-36. Given the reported minimal differences between the RAND-36 and the Medical Outcomes Study Short Form-36 (SF-36), a physical component summary (PCS) and a mental component summary (MCS) were calculated according to the manual for SF-36 health summary scales using Dutch population means, SD, and factor score coefficients20. The summary scores are normally distributed with a mean of 50 and an SD of 1021.
Comorbidity
Comorbidity was assessed at baseline. Somatic comorbidity was measured with a list adapted from the Health Interview Survey of the Statistics Netherlands22, a validated list amenable to self-reporting23. This list covers 20 chronic conditions that are prevalent in the Netherlands; most of them are also prevalent in RA12,24. Respondents were asked to indicate whether they had had any of the conditions in the previous 12 months. The following 9 categories of chronic somatic comorbidity were created based on the body systems involved: (1) circulatory conditions (myocardial infarction or other serious heart disorders, stroke), (2) respiratory conditions (asthma or chronic bronchitis), (3) digestive conditions (disorders of the stomach, disorders of the liver, disorders of the gall bladder, serious disorder of the intestine longer than 3 mos), (4) genitourinary conditions (disorders of the kidneys, kidney stones, inflammation of the bladder), (5) neurological conditions (migraine, dizziness with falling, epilepsy), (6) musculoskeletal conditions (hernia or chronic back complaints), (7) endocrine, metabolic, and nutritional conditions (diabetes mellitus, disorders of the thyroid gland), (8) cancer, and (9) a rest category (hypertension, infection of the nasal cavity or frontal sinus, skin conditions). These 9 categories are in accordance with previous research also using the list about somatic comorbidity from the Health Interview Survey of the Statistics Netherlands25.
Comorbid depression was assessed with the Center for Epidemiological Studies-Depression Scale (CESD)26. The CESD is a short self-administered scale designed to measure depressive symptomatology in the general population. The CESD consists of 20 items and has a range of 0 to 60, with higher scores indicating more depressive symptomatology. Scores of ≥ 16 suggest the presence of depression.
Statistical analyses
To determine the effect of specific comorbid conditions on functioning over time, we performed a longitudinal analysis of how baseline comorbidity predicts longterm physical and mental functioning. Analyses were carried out with the use of a linear random intercept (mixed-effect) model with serial correlation of the residuals27. With this model, we controlled for intersubject correlation, taking into account that this correlation decreases with increasing time, and for differences in duration between measurement moments. A model was used with time and all categories of comorbidity as independent variables and the outcome at baseline, 1-, 2-, 5-, and 11-years followup as dependent variables. The predictors were the categories of comorbidity. Time was entered as a continuous variable. Separate analyses were performed for the outcome physical functioning, measured with a disease-specific measure (HAQ) and with a generic measure (SF-36), and for mental functioning.
Loss to followup might introduce bias into longitudinal studies. In our study, we used a statistical model that took into account the selection bias that may have occurred. The model assumes that nonresponders have the same physical and mental functioning during followup as comparable responders; that is, responders with equal values for all variables in the model. Therefore, the model fills in the data of nonresponders with data of comparable responders (those who have the same physical functioning at baseline and are comparable in other variables used in this model).
All models contained age, sex, RA disease duration, and DAS score to control for possible confounding by these factors. To enhance the interpretability of the regression coefficients, we subtracted mean age from the variable age, median RA disease duration from the variable RA disease duration, and mean DAS score from the variable DAS score. All analyses were carried out using R, package lme428. Results were considered statistically significant when p values were < 0.05.
RESULTS
Response
Of the eligible patients, 882 (75%) returned the questionnaire in 1997. Of these patients, 755 (crude response 85%; net response, the response in patients still alive, was 87%) returned the questionnaire in 1998, 683 (crude response 77%, net response 81%) in 1999, 529 (crude response 60%, net response 71%) in 2002, and finally 370 (crude response 42%, net response 62%) in 2008. During the study period, 285 patients died6.
Study population
Patient characteristics are shown in Table 1. Of all the patients with RA at baseline, 72% were women, the mean age was 59.3 years (SD 14.8), and the median RA disease duration was 5.0 years (interquartile range 2.0–14.0). At baseline, 67.9% had ≥ 1 comorbid condition. The most common comorbid conditions were, as expected, those in the rest category (hypertension, conditions of the nasal cavity and frontal sinus, and skin conditions), depression, and musculoskeletal conditions.
Description of RA study population at baseline (n = 882). Values are n (%) unless otherwise specified.
Longterm association between comorbidities and physical and mental functioning
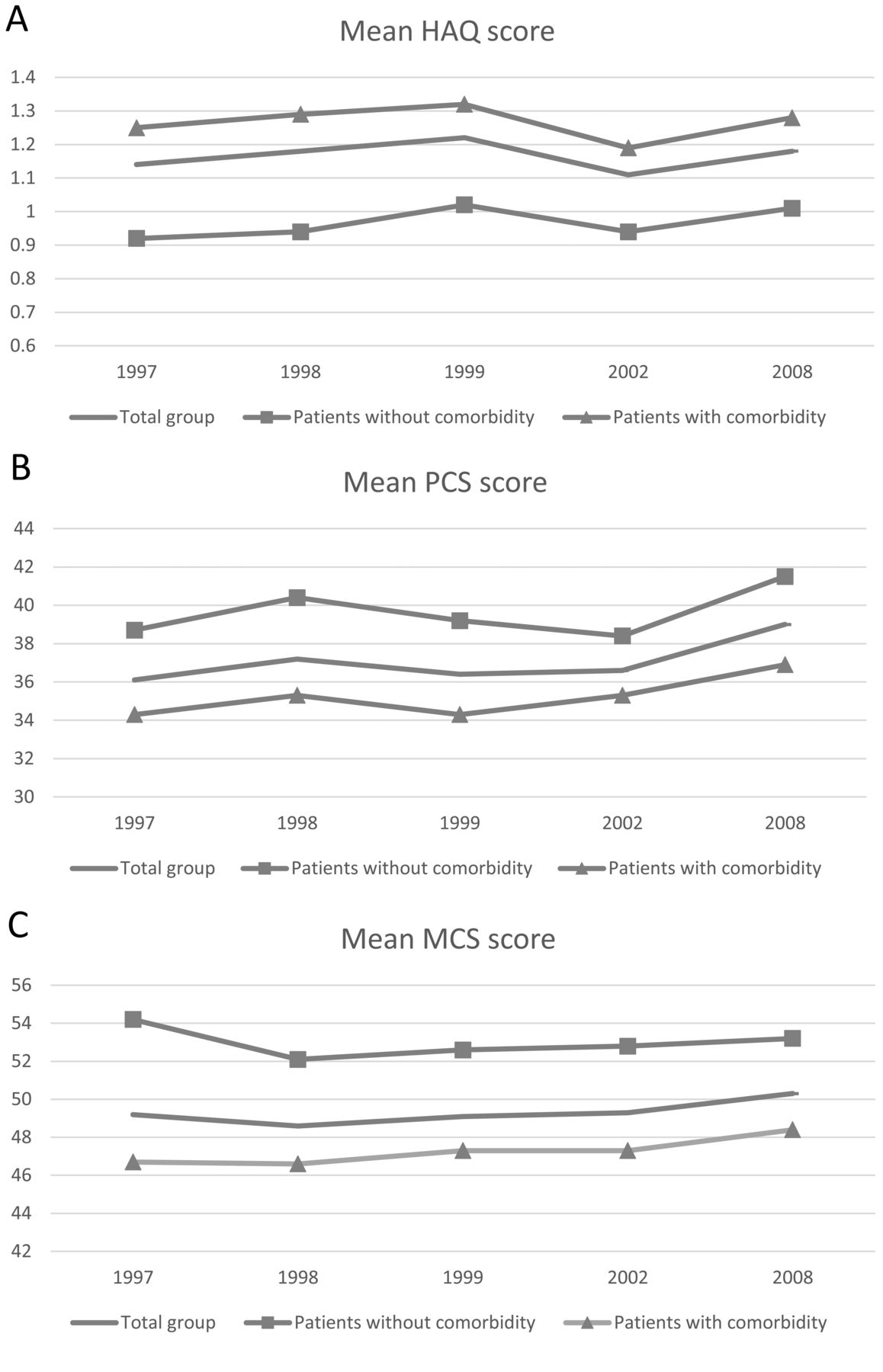
Figure 1 presents the trajectories of physical and mental functioning for the total group of patients, patients without comorbidity, and patients with comorbidity. In addition, Table 2 provides the mean physical and mental functioning scores over an 11-year period, and the difference in physical and mental functioning between patients with RA with a specific comorbid condition and patients with RA without comorbidity. The mean HAQ score for an average patient with RA without comorbidity was 0.99. The same patient with a comorbid circulatory condition at baseline had a mean HAQ score of 0.99 + 0.23 = 1.22. Results showed higher HAQ scores, and thus worse physical functioning in patients with RA with circulatory conditions and depression.
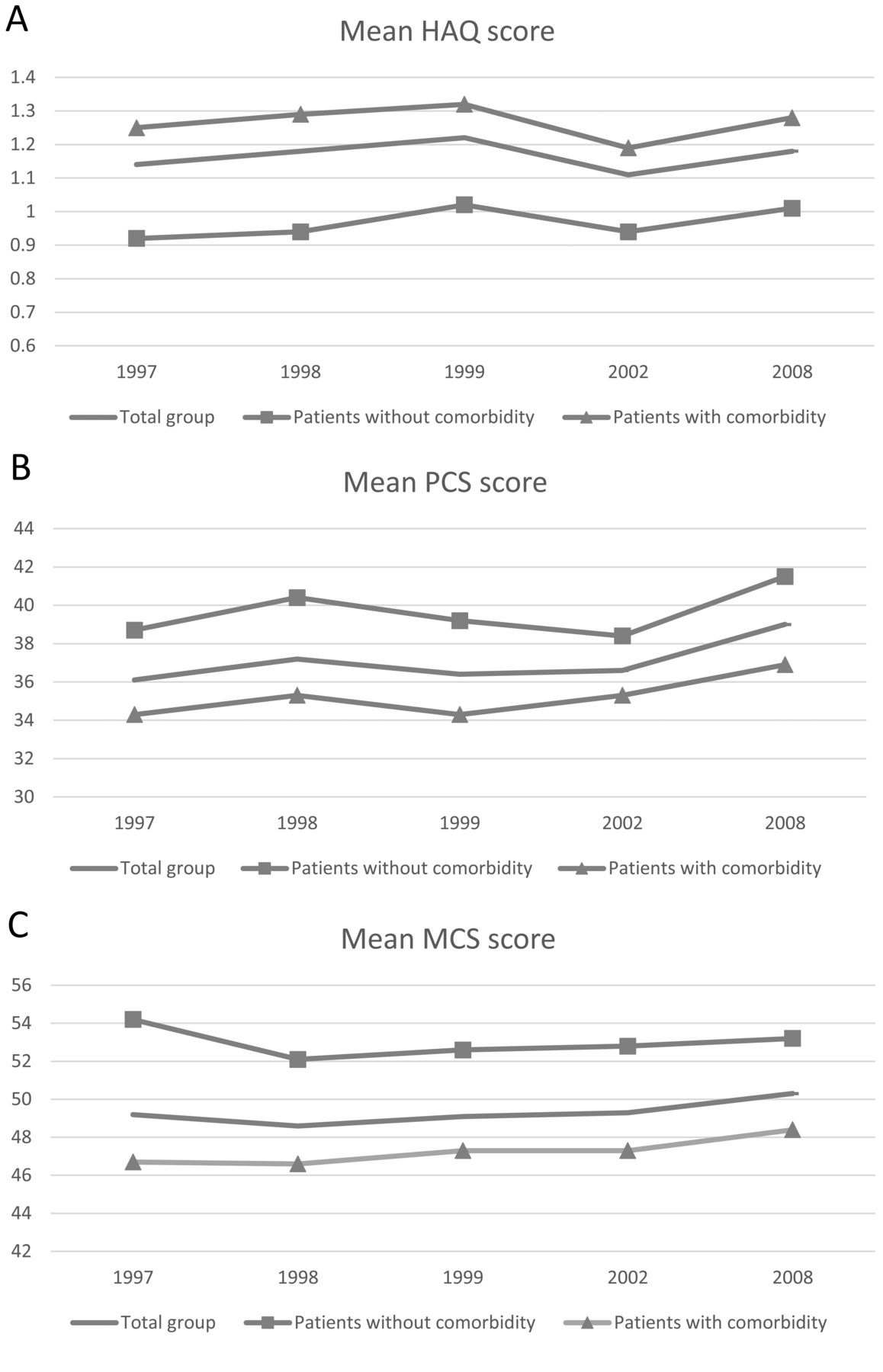
A. Physical functioning according to the HAQ over 11 years for the total group of patients, patients without baseline comorbidity, and patients with baseline comorbidity. A lower HAQ score indicates better physical functioning. B. Physical functioning according to PCS of the SF-36 over 11 years for the total group of patients, patients without baseline comorbidity, and patients with baseline comorbidity. A higher PCS score indicates better physical functioning. C. Mental functioning according to the MCS of the SF-36 over 11 years for the total group of patients, patients without baseline comorbidity, and patients with baseline comorbidity. A higher MCS score indicates better mental functioning. HAQ: Health Assessment Questionnaire; PCS: physical component summary; SF-36: Medical Outcomes Study Short Form-36; MCS: mental component summary.
Differences in physical functioning and HAQ between patients with RA with specific comorbidities and patients with RA without comorbidity. Adjusted for age, sex, disease duration, disease activity, and all other comorbidities. Range 0–3; higher score indicates worse physical functioning.
Physical functioning and SF-36. Adjusted for age, sex, disease duration, disease activity, and all other comorbidities. Range 0–100; lower score indicates worse physical functioning.
Mental functioning and SF-36. Adjusted for age, sex, disease duration, disease activity, and all other comorbidities. Range 0–100; lower score indicates worse mental functioning.
Scores on the SF-36 were lower, and thus showed worse physical functioning in patients with RA with respiratory conditions, musculoskeletal conditions, cancer, and depression. For example, an average patient without comorbidity had a mean PCS of 37.85. The same patient with a comorbid respiratory condition and with comorbid depression had a mean PCS of 37.85 – 2.12 – 2.76 = 32.97.
Patients with RA with respiratory conditions and depression presented lower scores and thus worse mental functioning. For example, a patient without comorbidity had a mean MCS score of 53.02. A patient with a comorbid respiratory condition had a mean MCS of 53.02 – 2.21 = 50.82.
DISCUSSION
Our study provides information about which specific comorbid conditions are associated with worse longterm physical and mental functioning in patients with RA. Knowledge about the effect of specific comorbidities provides clinicians information about target groups who are at risk for worse longterm functioning, facilitating early referral and treatment of these specific groups.
At the beginning of our study, 75% of the patients returned the questionnaire. Rupp, et al investigated in a previous study for this cohort whether respondents differed at baseline from nonrespondents29. For this purpose, nonrespondents were approached by telephone interview. Results showed that respondents were in general comparable to nonrespondents. Nonrespondents did have less pain and used specific healthcare services less often.
To study the effect of somatic comorbidities on functioning, we used a list that covers the chronic conditions that are most prevalent in the general population in the Netherlands. Most of these comorbidities are also prevalent in patients with RA12,14,24. The effect of 2 comorbidities, osteoporosis and infection, which are specifically highly prevalent in patients with RA24,30 but not specified in the National Health Interview Survey, could not be addressed in our study. Future research should also specifically address the effect of osteoporosis and infection on functioning.
We used a statistical model that assumes that the outcomes of nonresponders (dropouts) are equal to the outcomes of responders who are comparable in baseline characteristics. This statistical method minimizes the risk of selection bias in case of difference between nonresponders and responders31. Although this model reduces the risk of selection bias, this type of bias cannot completely be ruled out.
Comorbid circulatory, respiratory, musculoskeletal conditions, cancer, and depression impaired the longterm physical functioning of patients with RA independent of age, disease duration, and disease activity. The HAQ is often used in RA to survey the severity of the disease. Pope, et al found that a HAQ score of −0.21 corresponded to a minimally important difference32. If we apply these results to our study, circulatory conditions and depression showed not only a statistically significant but also a clinically significantly worse score on the HAQ32,33. Scores of the SF-36 physical functioning showed that patients with RA without comorbid conditions still had a much lower physical functioning than the mean score of 50 for people in the general population21. When patients with RA also had a respiratory or musculoskeletal condition, cancer, or depression, their physical functioning was even worse. Kosinski, et al found that a PCS score of 3.1 indicates a minimally important change34. If we apply these results to our study, patients with cancer showed not only statistically significant but also a clinically significantly worse physical functioning.
Depression was associated with clinically significantly worse physical functioning, measured with both the HAQ and the SF-36. This corresponds to other studies. Moussavi, et al found that the combination of depression and arthritis was cross-sectionally associated with lower health status, more than depression alone, arthritis alone, or 2 somatic conditions35. Morris, et al found that depression and even intermittent depression over time was associated with low self-reported health status and disability after 18 years36. Depression is linked to RA and physical functioning by biological, behavioral, cognitive, and social pathways37,38,39,40. Psychological interventions have been shown to have a favorable effect on physical functioning in patients with RA41,42.
The baseline prevalence of depression was, in comparison with the somatic comorbidities, relatively high (28.5%). It is difficult to compare the prevalence of comorbid depression and the somatic comorbidities, because these prevalences were estimated using different measures. The high prevalence of depression is, however, in accordance with the literature24.
To provide both disease-specific and a generic overview of physical functioning, we used both the HAQ and the physical scales of the SF-36. The HAQ is disease-specific; it asks for specific activities which are often related to RA, while the SF-36 is a generic measure, meaning that functioning is assessed in a general way — not specific to any age, disease, or treatment group19. Our results showed that the effect of comorbid conditions is more apparent when physical functioning is measured with the SF-36. Given the high prevalence of comorbidity in patients with RA (in this cohort, more than two-thirds of the patients had ≥ 1 comorbid condition at baseline), we recommend adding the SF-36 to the HAQ to identify a full spectrum of functioning.
Respiratory conditions and depression were associated with worse mental functioning. To our knowledge, ours is the first study in patients with RA that investigated the association between specific comorbidities and mental functioning. A study that compared mental functioning among patients with different chronic diseases also showed that patients with respiratory conditions had the lowest mental functioning43. This could be because of the loss of independence, low control over disease, and physical disability. In addition, it seems that in respiratory diseases, because of the limited exercise tolerance and dyspnea, anxiety is involved44.
Considerations
The strengths of our study were its longitudinal design and its longterm followup period. Moreover, a wide spectrum of somatic comorbid conditions and comorbid depression was investigated, and both physical and mental functioning were investigated.
In our study, the goal was to investigate the effect of a specific comorbid condition on the longterm functioning. We did not investigate the association of combinations of comorbidities with functioning, although it is likely that many patients had > 1 comorbid condition. However, scores of patients having > 1 condition can be calculated from the data in Table 2.
The associations between specific comorbidities and functioning might differ for patients depending on age, sex, or the presence of other comorbidities. Therefore, additional analyses were performed. No significant interactions were found between comorbidities with significant main effects and age, between these comorbidities and sex, and among these comorbidities (data not shown). This indicates that the associations between specific comorbidities and functioning do not depend on age, sex, or the presence of other comorbidities. Treatment strategies as well as the classification of RA changed in the years our study was conducted. As a consequence, it is possible that the effect of the specific comorbidities on functioning changed over time. The short-term effect of baseline predictors on functioning could differ from the longterm effect. We tested this assumption by 2 additional linear regression analyses, in which we studied the effect of baseline predictors on functioning in 1998 and in 2008. The results of these 2 linear regression analyses were similar to the results of the longitudinal analyses (data not shown). This indicates that the effect of the baseline predictors on functioning is stable over time.
Clinical relevance
Our RA study demonstrates that comorbid circulatory conditions, respiratory conditions, musculoskeletal conditions, cancer, and depression were associated with low physical functioning, while respiratory conditions and depression were associated with low mental functioning. Patients with these comorbidities had an increased risk of worse functioning in the long term. Moreover, physical functioning was also clinically significantly worse for patients with circulatory conditions, cancer, and depression, and mental functioning was clinically significantly worse for patients with depression.
A recent study showed that the detection and management of comorbidities in RA is far from optimal24. We recommend that clinicians assess comorbidity systematically in medical management because of the longterm effect of comorbidity on functioning. Raising the awareness of the importance of comorbidity in patients with RA could contribute to increasing the quality of care for these patients.
- Accepted for publication October 29, 2015.








{kind=link}