

To the Editor:
Rituximab (RTX) in combination with glucocorticoids has been recommended for relapsing granulomatosis with polyangiitis (GPA) if the disease remains active after a course of cyclophosphamide (CYC) lasting 3–6 months1. We describe a case of perianal Crohn disease (CD) in a patient with GPA who had been treated with RTX.
A 24-year-old woman with GPA was diagnosed in 2006 with bilateral cavitating pulmonary lesions on computed tomography, pauciimmune glomerulonephritis with crescents and extraglomerular arteritis on renal biopsy, mononeuritis multiplex, and proteinase 3 (PR3)-antineutrophil cytoplasmic antibodies (ANCA) of > 100 U/ml. Six pulses of CYC with methylprednisolone were administered in 2006, but the patient experienced pulmonary and uveal recurrence of her GPA 5 weeks later. She had 1 course of 2 infusions of RTX (1 g per infusion) in combination with CYC in November 2006 (total cumulative CYC dose 7.5 g). In 2008 she developed headaches secondary to GPA recurrence affecting the pituitary gland confirmed by transsphenoidal biopsy and resulting in adrenocorticotropic hormone deficiency and cranial diabetes insipidus. She received 1 further course of RTX infusion in June 2008 with a further relapse (recurrence of headaches) in November 2009. Because azathioprine (AZA), methotrexate, and mycophenolate mofetil had been ineffective maintenance therapy, she began 6-monthly RTX infusions for 2 years. She received single RTX infusions (1 g each) in November 2009, August 2010, January 2011, and July 2011.
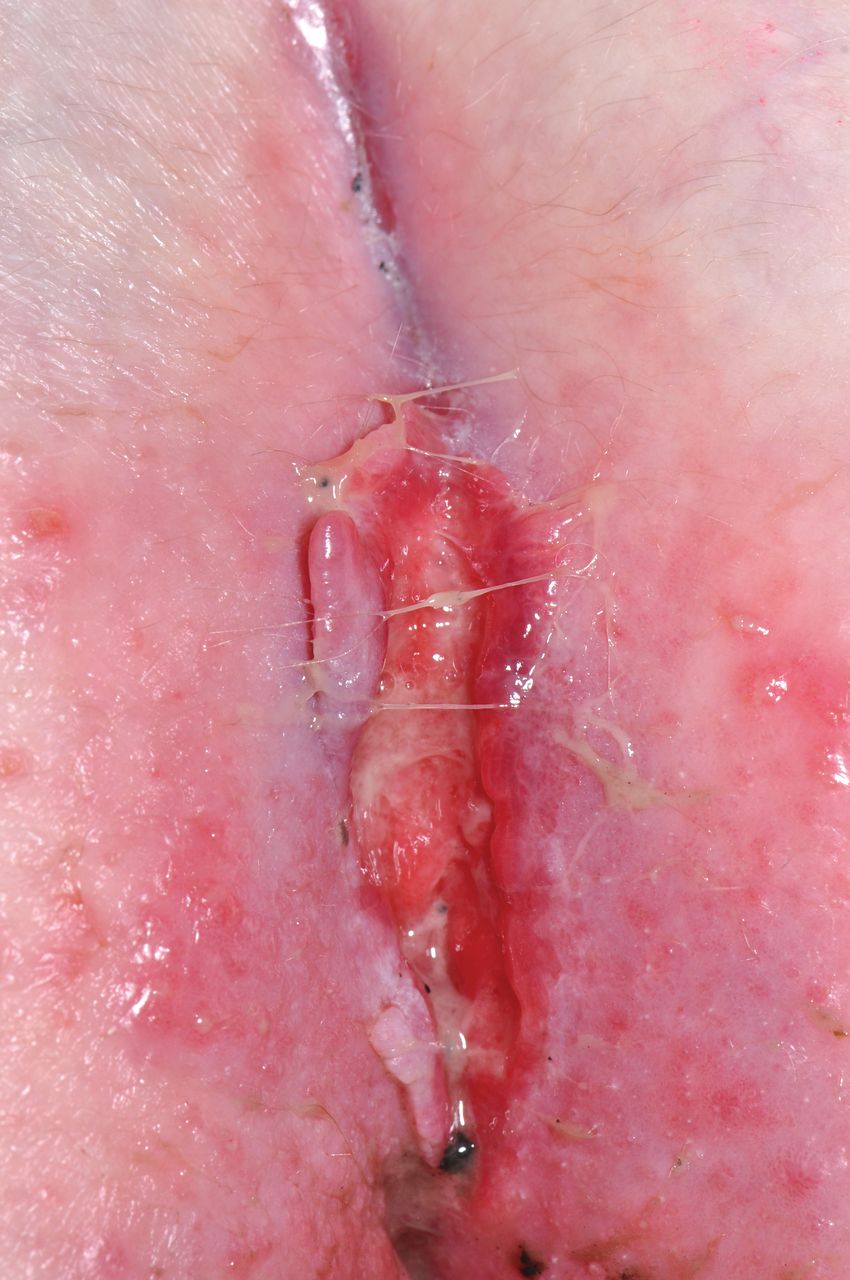
In April 2013 she developed perineal ulceration with granulation tissue on biopsy. The perineal disease progressed over the next year and developed into marked perianal ulceration by April 2014. Biopsy of the perineal skin showed mixed inflammatory cell infiltrate and colonoscopy was macroscopically normal. Microscopy revealed mild inflammatory changes with focal cryptitis, a preponderance of eosinophils not typical for inflammatory bowel disease (IBD), and crypt abscess formation. Magnetic resonance imaging (MRI) of the pelvis showed acute inflammation only. It was thought that the perianal ulceration was because of a recurrence of GPA and a further course of RTX was given in May 2014 (total cumulative RTX dose 10.8 g). The patient was readmitted in September 2014 with worsening perianal pain, ulceration, and discharge (Figure 1). The perianal skin showed evidence of fissures and progressive ulceration. Repeat MRI pelvis revealed extensive fistulating disease with a marked rectovaginal fistula, and perianal skin biopsies showed granulomata, consistent with CD. Repeat colonoscopy and colonic biopsies were normal. Swabs grew perineal skin commensals and tuberculosis and herpes simplex virus swabs were negative. The patient is currently receiving treatment with AZA and infliximab for her CD with good effect (complete resolution of the 3 fistula).
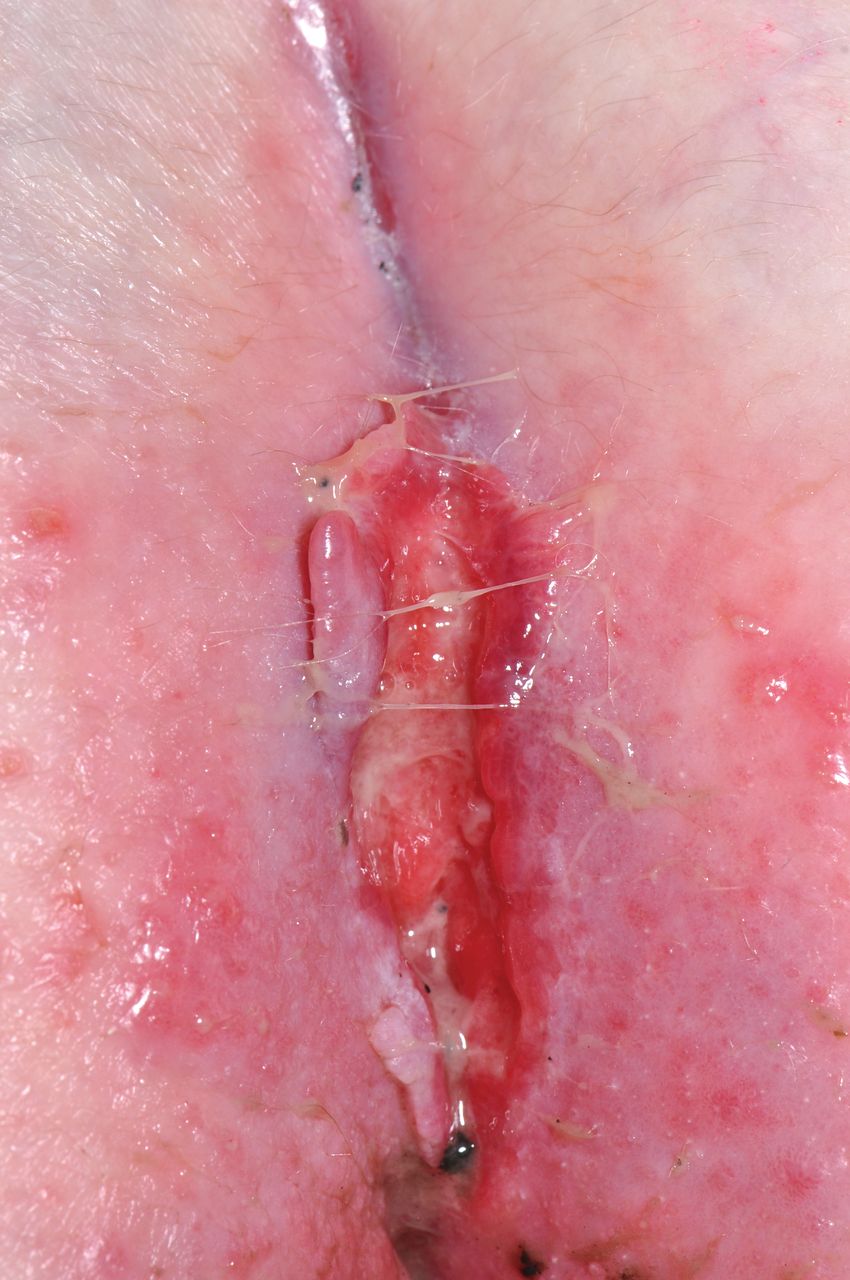
Perineal ulceration.
ANCA are common in both GPA and IBD, and cytoplasmic-staining ANCA reacting with PR3 is predominantly found in GPA, but may be found in CD2. GPA can present similarly to CD and CD can mimic GPA, but it is thought that the presence of both conditions is exceptionally rare, with 1 case report series identifying only 13 patients over 20 years2.
RTX is a chimeric anti-CD20 monoclonal antibody that targets B cell lymphocytes. Both B and T cells have been implicated in the pathogenesis of GPA3,4 and IBD. It has been suggested that B cells may not have a proinflammatory role in IBD and may have a protective effect, reducing inflammation by producing the antiinflammatory cytokine IL-105. There are only a few reports in the literature of induction or exacerbation of IBD by RTX.
A report of a 58-year-old man who underwent RTX salvage therapy for severe ulcerative colitis (UC) resulted in greatly depleted local and systemic CD20+ B cells, but the patient experienced a severe exacerbation of UC5. Two similar reports describe a 62-year-old woman with disseminated B cell lymphoma and a 67-year-old man with follicular lymphoma who both developed fulminant colitis after RTX therapy6,7. Both patients required surgery after not responding to medical therapy. Other reports describe UC in a 4-year-old boy after receiving RTX for nephrotic syndrome, which responded to corticosteroids8, and a 45-year-old woman with Grave disease with new-onset UC and arthritis following RTX9.
Conversely, RTX was not associated with worsening of UC in a double-blinded randomized controlled trial consisting of 24 patients with moderately active UC10.
Colitis may be associated with hypogammaglobulinemia. This has been reported with cytomegalovirus colitis in a patient with rheumatoid arthritis11, and in association with common variable immunodeficiency12. Our patient had normal immunoglobulin (Ig) levels prior to RTX therapy. However, thereafter the patient had low IgM (0.11–0.22 g/l) following the first RTX course until April 2012, when the level normalized. Low IgG (5.6 g/l) was noted after the last RTX course in May 2014.
RTX is effective in relapsing, refractory GPA. As shown in our case, RTX could induce or exacerbate IBD. Our patient had a normal colonoscopy with mild inflammatory changes on biopsy and perianal granulomata.








{kind=link}