

Abstract
Objective. The aim of the study was to investigate the effect of radiographic spinal progression and disease activity on function and spinal mobility in patients with ankylosing spondylitis (AS) treated with tumor necrosis factor-α (TNF-α) inhibitors for up to 10 years.
Methods. Patients with AS who participated in 2 longterm open-label extensions of clinical trials with TNF-α inhibitors (43 receiving infliximab and 17 receiving etanercept) were included in this analysis based on the availability of spinal radiographs performed at baseline and at a later timepoint (yr 2, 4, 6, 8, and 10) during followup. Spinal radiographs were scored according to the modified Stoke Ankylosing Spondylitis Spine Score (mSASSS). Function was assessed by the Bath Ankylosing Spondylitis Functional Index (BASFI), spinal mobility by the Bath Ankylosing Spondylitis Metrology Index (BASMI), and disease activity by the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI).
Results. After the initial improvement, BASFI and BASMI remained remarkably stable at low levels over up to 10 years despite radiographic spinal progression. In the generalized mixed effects model analysis, no association between the mSASSS and the BASFI change (β = 0.0, 95% CI −0.03 to 0.03) was found, while there was some effect of mSASSS changes on BASMI changes over time (β = 0.05, 95% CI 0.01–0.09). BASDAI showed a strong association with function (β = 0.64, 95% CI 0.54–0.73) and to a lesser extent, with spinal mobility (β = 0.14, 95% CI 0.01–0.26).
Conclusion. Functional status and spinal mobility of patients with established AS remained stable during longterm anti-TNF-α therapy despite radiographic progression. This indicates that reduction and continuous control of inflammation might be able to outweigh the functional effect of structural damage progression in AS.
Function is regarded as one of the most important outcome variables in chronic rheumatic diseases, such as rheumatoid arthritis (RA) and ankylosing spondylitis (AS), and is dependent both on disease activity and structural damage. Early in the course of the disease, function is mostly determined by disease activity, while later on, structural damage becomes an additional relevant component1,2. Structural damage in AS studies is usually quantified by the modified Stoke Ankylosing Spondylitis Spine Score (mSASSS), which accounts for erosions, sclerosis, squaring of the vertebral bodies, and syndesmophytes3. The mSASSS is dominated by syndesmophytes — reflecting new bone formation — but the other abnormalities in the spine also have an effect on function1. It has been shown before that the most often-used score to measure function in AS — the Bath Ankylosing Spondylitis Functional Index (BASFI) — correlates both with the mSASSS and with scores for disease activity such as the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI). In a cross-sectional study of an AS cohort, the Outcome Assessments in Ankylosing Spondylitis International Study (OASIS) cohort, there was a rather strong association of the mSASSS with the BASFI when disease activity (BASDAI) was low while this correlation was poor in patients with a high BASDAI1. The association between the mSASSS and measurement of spinal mobility, the Bath Ankylosing Spondylitis Metrology Index (BASMI), has also been investigated, showing a clear correlation between mSASSS and BASMI4,5 but also an additional dependence of spinal mobility on the level of inflammation, measured by magnetic resonance imaging (MRI) in the spine in 1 study5. Thus, structural damage has an influence on function and spinal mobility in AS.
Tumor necrosis factor-α (TNF-α) inhibitors have been proven to be very effective for the treatment of various measures of disease activity such as patients’ symptoms (BASDAI), C-reactive protein (CRP), and inflammation on MRI, but failed to show inhibition of radiographic spinal progression over 26,7,8 and 4 years9 of treatment. Two studies showed, however, some evidence that longterm10 or early11 treatment with TNF inhibitors might have an effect on radiographic spinal progression. These findings had stimulated an intensive discussion on how to explain this and why this might differ from RA where TNF inhibitors showed a good effect on both disease activity and structural damage12,13,14. At the same time, these findings also raised the highly relevant question about the functional relevance of progression of structural damage seen in AS if at the same time disease activity is reduced so effectively.
In our current study, we investigated functional status and spinal mobility in relation to structural damage progression and disease activity in patients with AS treated with TNF-α inhibitors for up to 10 years.
MATERIALS AND METHODS
Patients
For the purpose of our study, we selected 60 patients with AS who were treated with TNF-α inhibitors [infliximab (IFX), n = 43, or etanercept (ETN), n = 17] in longterm extensions (up to 10 yrs) of 2 randomized controlled trials (IFX, n = 69, ETN, n = 30)15,16,17,18 based on the availability of at least 2 sets of spinal radiographs (baseline and followup) obtained at least 2 years apart. Both trials had identical design during the longterm extension with clinical examination and safety assessment every 12 weeks and radiographic examination of the spine every 2 years up to Year 10. No switch of a TNF-α inhibitor was allowed; discontinuation of the initially started TNF-α inhibitor resulted in study discontinuation. Besides TNF-α inhibitors, which were provided as a study drug, patients were treated according to the standard of care. The baseline characteristics of the included patients are presented in Table 1.
Baseline and Week 12* characteristics of the included patients. Values are mean ± SD unless otherwise specified.
Clinical assessment
Clinical assessment at each visit during the longterm followup included assessment of disease activity with the BASDAI19 and CRP, of the functional status applying the BASFI20, and of the axial mobility by use of the BASMI (a 2-step definition)21.
Radiographic assessment
Collected spinal radiographs (up to 6 sets consisting of cervical and lumbar spine radiographs, lateral views) were digitized (if necessary), anonymized, and subsequently scored according to the mSASSS (0–72)3 independently by 2 trained readers (DP and AF) blinded for all clinical data, but not for the timepoint.
Statistical analysis
The main purpose of our work was the evaluation of the effect of radiographic progression on physical function and spinal mobility in patients with AS continuously treated with TNF-α inhibitors up to 10 years. We aimed to investigate whether an initial improvement of BASFI and BASMI caused by the start of a treatment with IFX or ETN was weakened at followup in patients with radiographic progression. For that reason, we compared the BASFI and BASMI status initially achieved under treatment with IFX or ETN after 12 weeks with timepoints at which followup assessments of the mSASSS were available. We calculated differences in BASFI and BASMI between Week 12 and the corresponding timepoints at followup, and compared these change scores with the corresponding change scores in the mSASSS. To estimate the effect of radiographic progression on function and spinal mobility, we further had to control for disease activity (BASDAI). Besides methods of descriptive statistics, we applied a generalized linear mixed effects model (GLM) analysis. Outcome variables were change in BASFI and change in BASMI, and covariables were change in mSASSS and change in BASDAI. The GLM methods take the dependency of repeated assessments within an individual patient into account. These models further allow an adjustment for missing data, especially those caused by patients lost to followup. The dependency of the outcome values from the baseline status (mSASSS at baseline, BASDAI, BASFI, and BASMI at Week 12) was also considered by including these variables as covariables into the GLM models. An agreement on the mSASSS score between 2 readers was evaluated using an intraclass correlation coefficient.
Ethical approval
Both study protocols were approved by the ethics committee of the Charité Universitätsmedizin Berlin, Berlin, Germany, and by all local ethical committees of the participating centers. Written informed consent was provided by all included patients.
RESULTS
Starting with 60 patients who had spinal radiographs at baseline, Year 2 complete sets of radiographs were available in 57 patients (95.0%), Year 4 in 41 patients (68.3%), Year 6 in 34 patients (56.7%), Year 8 in 23 patients (38.3%), and Year 10 in 17 patients (28.3%; Table 2).
Status scores for the mSASSS, BASDAI, BASFI, and BASMI in patients who completed a 2-, 4-, 6-, 8-, and 10-year followup. Values are mean ± SD unless otherwise specified.
There was good agreement between readers for the mSASSS status scores at all timepoints: the intraclass correlation coefficients were 0.946 at baseline, 0.937 at Year 2, 0.930 at Year 4, 0.948 at Year 6, 0.920 at Year 8, and 0.972 at Year 10. The agreement between the change scores was moderate: the intraclass correlation coefficients for change in the mSASSS from baseline to years 2, 4, 6, 8, and 10 were 0.445, 0.554, 0.727, 0.562, and 0.565, respectively.
The dynamics of the means for mSASSS, BASFI, BASMI, and BASDAI in patients who completed 4, 6, 8, and 10 years of observation are presented in Table 2 and Figure 1. The results were robustly consistent in all completer subgroups: despite ongoing radiographic spinal progression (about 6 mSASSS points over 10 yrs or about 1.2 mSASSS points every 2 yrs), BASFI and BASMI remained stable on a low level starting from Week 12 (which was taken as a baseline for the clinical outcome variable to exclude initial improvement from baseline related to initiation of anti-TNF therapy) up to Year 10. The same was also true for the mean BASDAI that remained constantly below 3 over a period of up to 10 years.

Courses of radiographic spinal progression (mSASSS), disease activity (BASDAI), functional status (BASFI), and spinal mobility (BASMI) in patients who completed (A) 4, (B) 6, (C) 8, and (D) 10 years of anti-TNF treatment. Patients were included only if clinical and radiographic data were all available at all timepoints shown. * Week 12 was considered as baseline for BASDAI, BASFI, and BASMI to exclude initial improvement related to initiation of anti-TNF therapy. mSASSS: modified Stoke Ankylosing Spondylitis Spine Score; BASDAI: Bath Ankylosing Spondylitis Disease Activity Index; BASFI: Bath Ankylosing Spondylitis Functional Index; BASMI: Bath Ankylosing Spondylitis Metrology Index; anti-TNF: antitumor necrosis factor.
Figure 2 shows a cumulative probability plot of (A) BASFI and (B) BASMI change in relation to change in mSASSS. Depending on the number of available followup measures, each patient contributed to the plots with up to 5 values of mSASSS and BASFI/BASMI (change from baseline/week 12 to years 2, 4, 6, 8, and 10). Figure 2A demonstrates that BASFI change values are symmetrically distributed around 0 irrespective of the mSASSS change observed at the same timepoint even in patients with substantial progression in mSASSS of 4 points and more, indicating no clear relationship between these 2 variables. For the BASMI change (Figure 2B), only a slight trend toward BASMI worsening with mSASSS progression could be observed.
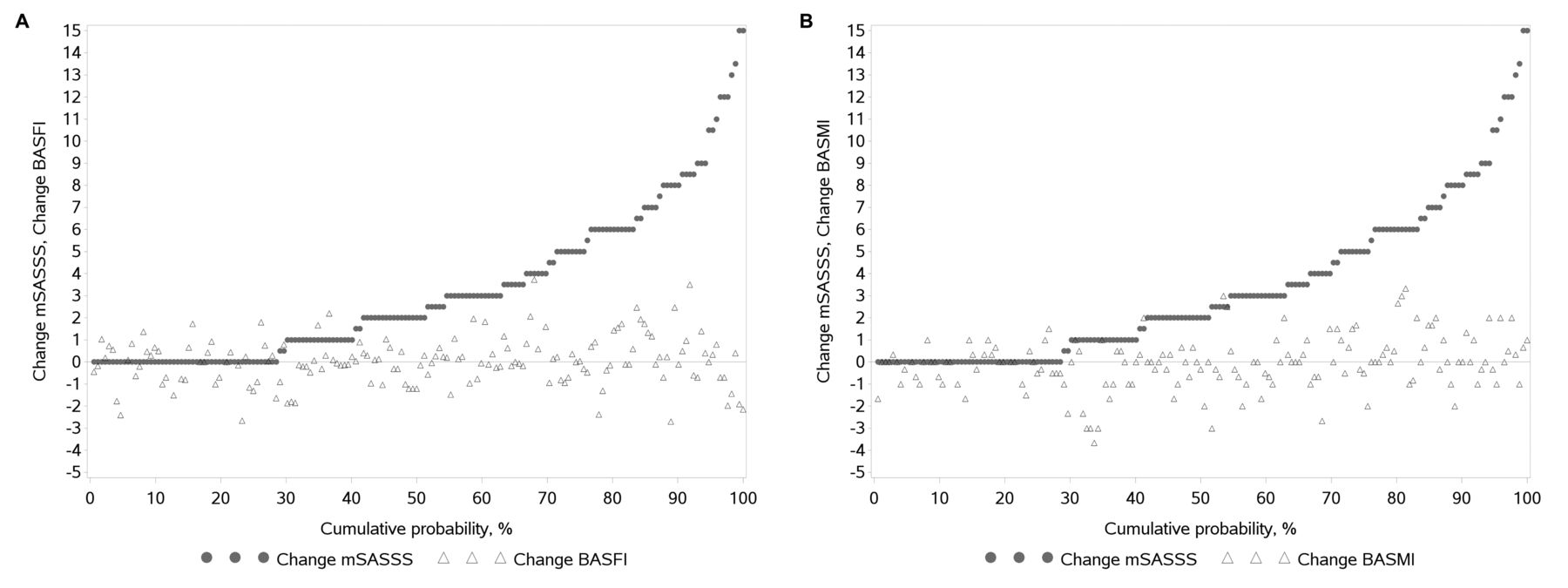
Cumulative probability plots of (A) BASFI and (B) BASMI changes in relation to radiographic spinal progression (mSASSS change) over up to 10 years of anti-TNF treatment. Change values between the followup timepoint and baseline for mSASSS, and between the followup timepoint and Week 12 for BASFI and BASMI are shown. BASFI: Bath Ankylosing Spondylitis Functional Index; BASMI: Bath Ankylosing Spondylitis Metrology Index; mSASSS: modified Stoke Ankylosing Spondylitis Spine Score; anti-TNF: antitumor necrosis factor.
To take the dependency of repeated assessments of the variables within an individual patient and a possible bias caused by patients lost to followup into account, the GLM analysis was performed. The GLM confirmed the lack of association between the mSASSS change and BASFI change over time during anti-TNF treatment, and at the same time a significant and meaningful effect (β coefficient of 0.64 indicating that 1-point change in BASDAI results in a 0.64-point change in BASFI) of BASDAI change on the change in the functional status (Table 3). Regarding the spinal mobility, there was some effect of both mSASSS change and BASDAI change on the change in the BASMI score over time (Table 3). These results were not biased by a dependency of the change scores of the BASFI and BASMI from the BASFI (p = 0.71) and BASMI (p = 0.23) status at Week 12. Therefore, these Week 12 variables were excluded from the final GLM models.
Variable estimates from the generalized linear mixed effect model analysis of the effect of radiographic spinal progression (mSASSS) and disease activity change (BASDAI) on the change in the functional status (BASFI) and spinal mobility (BASMI) during longterm treatment with TNF inhibitors.
In the following analysis, we grouped the followup measures of changes in mSASSS and BASDAI according to the degree of radiographic progression and the change in disease activity. Based on these groups, the GLM analysis resulted in mean changes in BASFI corresponding to 3 groups of radiographic progression (< 2, 2–5.5, or ≥ 6 mSASSS points) by taking simultaneous changes in BASDAI into account. Whereas the mean BASFI changes were similar across subgroups with different radiographic progression rates, a significant effect was again found for the change in BASDAI. A BASDAI improvement by ≥ 1 point corresponded to a mean improvement of BASFI by 0.85 points, and a BASDAI worsening by ≥ 1 point corresponded to a mean BASFI worsening by 1.05 points (Figure 3A). Regarding spinal mobility, there was a trend toward increase in the mean BASMI change score with increasing mSASSS changes (−0.21, 0.04, and 0.23 BASMI points for the mSASSS change by < 2, 2–5.5, and ≥ 6 points, respectively, p = 0.043; Figure 3B). A similar trend (p = 0.049) was observed for the mean BASMI change scores related to the BASDAI change (−0.26, −0.01, and 0.34 BASMI points corresponding to the BASDAI change by ≤ −1, −0.9 to 0.9, and ≥ 1 points, respectively; Figure 3B).

Adjusted mean changes (least square means) of (A) BASFI and (B) BASMI in relation to radiographic spinal progression (mSASSS change) and changes in disease activity (BASDAI change). BASFI: Bath Ankylosing Spondylitis Functional Index; BASMI: Bath Ankylosing Spondylitis Metrology Index; mSASSS: modified Stoke Ankylosing Spondylitis Spine Score; BASDAI: Bath Ankylosing Spondylitis Disease Activity Index.
DISCUSSION
Effective suppression of disease activity and stopping structural damage are the 2 most important aims for the treatment of chronic inflammatory diseases such as RA and axial spondyloarthritis (axSpA) including AS, both outcome variables determining function and level of disability. In our current study, we investigated for the first time, to our knowledge, longitudinally the association between disease activity, function, spinal mobility, and radiographic spinal progression in patients with AS treated for up to 10 years with a TNF inhibitor addressing the question of the functional relevance of radiographic progression if there is a good treatment effect on disease activity.
We could indeed confirm earlier findings that during TNF inhibitor therapy there was a continuous radiographic spinal progression over 10 years on the group level with an increase in the mean mSASSS score from 11 at baseline to 17 at Year 10, a biannual progression rate of slightly more than 1 mSASSS point. Our data are in line with the data from the Groningen Leeuwarden Ankylosing Spondylitis cohort, in which a mean biannual progression rate of 1.3 during 6 years of followup of patients with AS treated with TNF blockers was recorded22.
In our study, patients who continued drug treatment over time showed a very good and consistent reduction of the BASDAI from about 6 at baseline to about 2 at all timepoints up to Year 10. The same was also true for function and spinal mobility: BASFI and BASMI remained after initial improvement on a low level during the entire treatment period, very much in parallel to the BASDAI and not being influenced by the increase of the mSASSS.
Even more important, the mixed-model analysis demonstrated that individual variation in the functional state (BASFI) over time was nearly independent of radiographic spinal progression, but dependent on the variation in clinical disease activity (BASDAI). Interestingly, axial mobility (BASMI) demonstrated some dependency on both radiographic spinal progression and disease activity. This difference between the BASFI and the BASMI correlations might be related to the fact that BASMI is a rather objective measure while function might be influenced by additional not well-defined subjective factors. In the absence of pain and stiffness in patients treated with anti-TNF, BASFI seems to remain on a low level despite some limitation in axial mobility.
Previous studies addressing the question of the relationship between structural damage development in the spine and function/spinal mobility used mostly cross-sectional data4,5. The only study that used longitudinal analysis of the data (2-yr data from the OASIS cohort — all patients were naive to TNF inhibitor)1 found that relevance of radiographic spinal progression for the worsening of function was rather low after adjusting for disease activity: progression in about 18 mSASSS points was responsible for a change in BASFI in 1 point. However, in patients with a higher extent of structural damage at baseline (mSASSS > 36 points), radiographic progression was more functionally relevant than in patients with an initially low level of damage1.
Such a relationship is not unique for AS. Worsening of function in patients with RA treated with conventional (synthetic) disease-modifying antirheumatic drugs alone [such as methotrexate (MTX)] was also calculated to be rather slow: about 0.13 points of the Health Assessment Questionnaire score (scale between 0 and 3) only over 5 years (and 0.03 for the combination therapy of a TNF inhibitor and MTX for comparison)23. Therefore, the long observation period of up 10 years in our study is necessary for this kind of investigation. Our data clearly indicate that there is no or at most only a small effect of radiographic progression on function (and spinal mobility) in patients with AS treated effectively with TNF-α inhibitors. Interestingly, such an effect was also small in patients with more rapid progression, as can be seen from the probability plot shown in Figure 2.
Our study has limitations. First, there was a high proportion of patients who dropped out over the years; it was likely that, preferentially, the good responders remained in our study. However, even in patients considered good responders because they remained in our study, variation in disease activity and not radiographic spinal progression had a major effect on function and to a lesser extent on spinal mobility. Further, as shown in Figure 1, duration of the complete followup had no effect on the revealed association.
Second, spinal radiographs were scored by 2 readers who were not blinded for the timepoint. Such a method increases the sensitivity for change of scoring results (as shown in the OASIS cohort for instance24), but is associated with an increased risk of overestimation of radiographic spinal progression. However, the mean biannual progression rate was 1.2 mSASSS points in our study, which is in line with a biannual progression rate of 1.0–1.3 found in studies with a blinded reading of images6,7,8,25.
Third, function and spinal mobility in AS are not influenced only by inflammation and structural damage, but also by, for example, the effects of physical therapy. Thus, we cannot exclude that there might be even a further improvement of function and spinal mobility in patients with AS receiving a therapy that would stop radiographic progression if undertaking an intensive exercise program after reduction of inflammation. Therefore, finding treatments that suppress inflammation and stop new bone formation at the same time is still of interest for the future.
Finally, our study had no control group, i.e., patients receiving treatment other than TNF-α inhibitors. We would suggest, however, that retention of good functional status should not be attributed specifically to TNF-α inhibition, but should be considered as an effect of any effective antiinflammatory treatment, including nonsteroidal antiinflammatory drugs (NSAID) and interleukin 17 blockade, for instance. In our study, we could not specifically assess the effect of NSAID, which also might have an effect on inflammation and radiographic spinal progression26,27,28, because information on NSAID intake (dose, frequency) was not systematically collected during the longterm followup.
In our study, we demonstrated for the first time that good control of disease activity under longterm TNF-α inhibiting therapy was able to counterbalance the effect of radiographic spinal progression on functional status, and to a latter extent, on spinal mobility in patients with AS. These data allow a clear ranking of our treatment aims in AS and axSpA in general: good continuous control of active inflammation (and therefore of pain and stiffness) should be considered as a primary therapeutic goal also regarding preservation of function in the longterm perspective.
Acknowledgment
We thank the following rheumatologists for the inclusion and followup of their patients: R. Alten, J. Brandt, E. Gromnica-Ihle, H. Kellner, A. Khariouzov, A. Krause, M. Rudwaleit, M. Schneider, H. Sörensen, and H. Zeidler, and all of the physicians, study nurses, pharmacists, and technicians in the study centers who helped in the successful implementation of the trials. We are grateful to Beate Buss, Renate Pauli, and Annegret Langdon for the overall coordination of the studies; Hanna Dyck, Johanna Callhoff, and Anja Weiss for their support in the statistical analysis; and Claudia Fritz for the data management support. Further, we thank Torsten Karge (Clinical Guideline Service) for establishing the scoring interface for the reading of images.
Footnotes
The study with infliximab was funded by a grant from the German Ministry of Education and Research (through the Kompetenznetz Rheuma project) and by Essex Pharma/MSD Sharp and Dohme. The study with etanercept was funded by a grant from the German Ministry of Education and Research (through the Kompetenznetz Rheuma project) and by Wyeth Pharma/Pfizer Pharma. The work of AF on this project was supported by a fellowship from the Assessment of Spondyloarthritis International Society. JB received research grants, honoraria, speaker fees, and consultancy payments from Abbvie (Abbott), Novartis, and UCB. JS received research grants, honoraria, speaker fees, and/or consultancy payments from Abbvie, Janssen, Eli Lilly, MSD/Merck, Novartis, Pfizer, and UCB.
- Accepted for publication September 29, 2016.








{kind=link}
{kind=link}
{kind=link}