

Abstract
Objective. To estimate the development and potential disproportional distribution of longterm productivity costs (PC) and their determinants leading to work absenteeism and permanent work disability in working-aged patients with early rheumatoid arthritis (RA).
Methods. A cohort of subjects with early RA was created by identifying the new cases of RA from the national drug reimbursement register that had been granted a special reimbursement for their antirheumatic medications for RA from 2000–2007. The dataset was enriched by cross-linking with other national registries detailing work absenteeism days and permanent disability pensions. In the base case, the human capital approach was applied to estimate PC based on subjects’ annual number of absenteeism days and incomes. Hurdle regression analysis was applied to study the determinants of PC.
Results. Among the 7831 subjects with early RA, the mean (bootstrapped 95% CI) annual PC per person-observation year was €4800 (4547–5070). The annual PC declined after the first year of RA diagnosis, but increased significantly in subsequent years. In addition, the PC was heavily disproportionally concentrated in a small fraction of patients with RA, because only around 20% of patients accounted for the majority of total annual PC. The initiation of active drug treatment during the first 3 months after RA diagnosis significantly reduced the cumulative PC when compared with no drug treatment.
Conclusion. The longterm PC increased significantly in parallel with years elapsing after RA diagnosis. Further, the majority of these PC are incurred by a small proportion of patients.
Rheumatoid arthritis (RA) frequently has an adverse effect on a patient’s functional and work capacity, and this has economic implications for both the patient and society as a whole1. The diminished working ability initially appears as reduced work productivity in the workplace (i.e., presenteeism) and later as lost workdays (i.e., absenteeism), and it may eventually lead to the premature termination of the working career [i.e., a permanent work disability (WD)]. This translates into reduced family income and a restricted social network and a reduction in the gross national product for society. For example, in Europe the annual economic burden of RA has been estimated to be around €45 billion; of these, productivity costs (PC) are estimated to account for almost 40%2.
We have previously shown that early suppression of inflammatory activity in RA results in a better maintenance of work capacity3. Many clinical studies have demonstrated that prompt initiation of active drug treatment with a combination of disease-modifying antirheumatic drugs (DMARD) is superior to a more conservative strategy and this approach has become the prevailing routine practice in the clinics since the turn of the millennium. At the same time, biologic agents have become a therapeutic option for those patients experiencing an inadequate response to the traditional antirheumatic drugs. This development has been associated with declining WD among those patients who have been diagnosed with RA during this century4, but the loss of work productivity remains a major socioeconomic issue. Therefore, the goal of our study was to estimate the extent of this problem in monetary terms. In addition, little is known about the distribution of productivity losses because of RA. In healthcare, a minority of patients are commonly responsible for the highest costs. Thus, the primary objectives of our present study were to assess (1) the longterm average PC, (2) the potential disproportional concentration of the PC, and (3) how early and active treatment may be associated with the PC in Finnish patients with RA who were potentially active members of the workforce at baseline.
MATERIALS AND METHODS
Nationwide RA cohort
In our present study, we examined the available nationwide cohort of patients with early RA4. Briefly, a cohort of patients with early RA was created by identifying the new cases of RA from the national special reimbursement register of the Social Insurance Institution (SII) in Finland of individuals who had been granted a special reimbursement for DMARD, glucocorticoids, and biological medications from 2000–2007. To qualify for special reimbursement, the patient must fulfill a set of predefined medical criteria for RA. The special reimbursement status is applied from the SII by the treating physician, who fills out a required certificate. The certificate includes the description of the signs, symptoms, and course of the disease, applied diagnostic procedures, and the relevant International Classification of Diseases, 10th ed (ICD-10) code(s). In addition, the certificate includes a plan for the monitoring and treatment of diagnosed RA. The special reimbursement status approval decisions are recorded in the nationwide special reimbursement register including information about date of reimbursement decisions, specific reimbursement codes, and respective ICD-10 codes. During the study period, the lower special reimbursement covered 72%–75% of the price of the medicine, and the higher special reimbursement covered 100%.
The identified cohort included all incident adult patients (≥ 18 yrs) of working age (< 64 yrs) at registration (index day) from January 1, 2000, to December 31, 2007, i.e., when for the first time in their life, they had been granted a special reimbursement for medications because they had rheumatoid factor (RF)-positive (identified by ICD-10 code M05 in register) or RF-negative RA (M06; Figure 1). After the identification of the incident cases, the dataset was enriched by crosslinking with the other registries maintained by the SII and the Finnish Centre for Pensions, which has details of durations of work absenteeism (in days) and permanent WD pensions. Because of the administrative design of the applied national registries, only a limited number of patient characteristics were available (i.e., age, sex, RF status based on the ICD-10 codes, and medication during the first 3 mos). According to Finnish legislation, no ethics committee approval was required to conduct the present study because only unidentifiable register data were used and the patients were not contacted.

Flowchart of case identification protocol in the present study. ICD-10 MO5 or MO6: International Classification of Diseases, 10th ed.
Estimation and valuation of productivity loss
The dataset included the personal annual incomes for the patients who were awarded sickness allowances (i.e., allowances were calculated according to the preceding year’s personal income as assessed by the taxation authorities). Therefore, actual daily earnings (including payroll taxes) were available for each patient in terms of PC estimations instead of average daily earnings, which was a more common but less accurate way of estimating productivity losses. The earnings were adjusted to the 2013 level by using the official index of wage and salary earnings determined by Statistics Finland. To obtain the market price of an individual’s work production (gross wages), the annual incomes were multiplied by a factor (1.217) to incorporate the supplementary social welfare expenses paid by Finnish employers.
Costs resulting from absenteeism and permanent WD were estimated from a societal perspective. To value the productivity losses because of absenteeism and permanent WD in monetary terms, we applied a human capital approach (HCA); this is the most commonly used method for valuing PC. According to the HCA, the value of lost workdays is equal to the gross wages and it represents the value of missed work to both the employer and employee, as well as the loss of value of their contribution to society in the form of taxes. Therefore, the monetary value of each patient’s single day’s work production was multiplied by the annual number of WD days from the index day onward5. In addition, the national average (i.e., €137 per day in 2013 according to Statistics Finland) and sex-specific gross wage estimates (i.e., €150 and €124 per day in men and women, respectively) were applied to test whether the use of average valuations led to different PC estimates compared with the base case, where the patient-specific valuation approach was applied (i.e., the earnings that could be expected to be affected by RA, and thus resulting in lower cumulative earnings over time).
In the case of permanent WD, the annual number of permanent WD days was similarly multiplied by a patient’s work production per day. The productivity losses were applied to patients below the age of retirement, which was defined to be 65 years. The estimated PC can be converted to Can$ or US$ by using the European Central Bank annual bilateral exchange rates in 2013 (available at sdw.ecb.europa.eu).
Statistical analyses
The baseline characteristics of our study sample and study results were expressed as means, SD, simple frequencies, percentages, medians, and interquartile ranges (IQR), when appropriate. The PC were estimated and expressed as per patient-observation year, which were obtained by dividing the estimated number of WD days by the corresponding observation time. The observation time was defined as time spent (in yrs) in a predetermined study period, censored only by death or emigration, or the end of the followup period. The 95% CI for estimated mean values were obtained by nonparametric, bias-corrected, and accelerated bootstrapping.
As mentioned above, in healthcare, a minority of patients are commonly responsible for the highest costs, which leads to right-skewed cost distributions. To study this phenomenon in terms of the PC, a cumulative probability plot was applied to graphically reveal the potential disproportional concentration of the PC among the patients with early RA at baseline.
Because of the potentially right-skewed distribution of the PC with an excess of zeros, a hurdle model was applied to study the expected PC and their determinants. Hurdle-count models are 2-component models with a truncated count component for positive counts, i.e., absenteeism day costs in this case were taken as the hurdle component that models the zero counts. In our present study, the logit component was used to predict the zero costs and then the second component was obtained by applying a zero-truncated Poisson regression, and this was used to estimate the conditional expectation of the PC for the subsample of only the patients with non-zero PC.
P values < 5% level of significance were considered significant. All analyses were performed using STATA 12.0 (Stata Corp.).
RESULTS
Study cohort
The study cohort consisted of 7831 subjects with early RA, who at baseline were potentially available to be in the workforce (Figure 1). The median (IQR) followup time was 4.0 (2.2–6.3) years. The mean (SD) age of subjects was 46 (11) years and 71% were women. Men were slightly older than women at baseline (47.2 yrs vs 45.5 yrs, respectively). Sixty-three percent of men and 60% of women were RF-positive. During the first 3 months after the RA diagnosis, around 7253 (92.6%) of patients received an active drug therapy. A single DMARD was used by 2601 subjects (33.2%) whereas methotrexate (MTX) therapy was provided to 900 patients (11.5%). More of the patients (n = 2879, 36.8%) were undergoing a combination therapy which included MTX. Other types of combination therapies, but not including MTX, were being used by 873 patients (11.1%).
Longterm productivity losses
The RA cohort-specific mean value of daily production (i.e., gross wages) in men was €110 (median €75, IQR 106–135), and slightly less for women at €95 (median €67, IQR 93–113). Thus, the estimated average annual PC per patient-observation year was €4800 (bootstrapped 95% CI 4547–5070). The corresponding values in men and women were on average €6577 (95% CI 6026–7260) and €4071 (95% CI 3799–4358), respectively. The use of the national average gross wage estimate yielded higher PC estimate per patient-observation year (i.e., €6619, 95% CI 6270–6991). In addition, when applying the sex-specific national gross wage valuations, the corresponding estimates in men and women were €9003 (95% CI 8272–9966) and €5313 (95% CI 4959–5688), respectively.
The annual PC declined after the first year of RA diagnosis, but then increased significantly in the subsequent years (Figure 2). In addition, the cumulative probability plot clearly indicated the disproportional concentration of the PC among the patients with RA, i.e., a mere 20% or so of patients were responsible for the majority of the total annual PC (Figure 3).
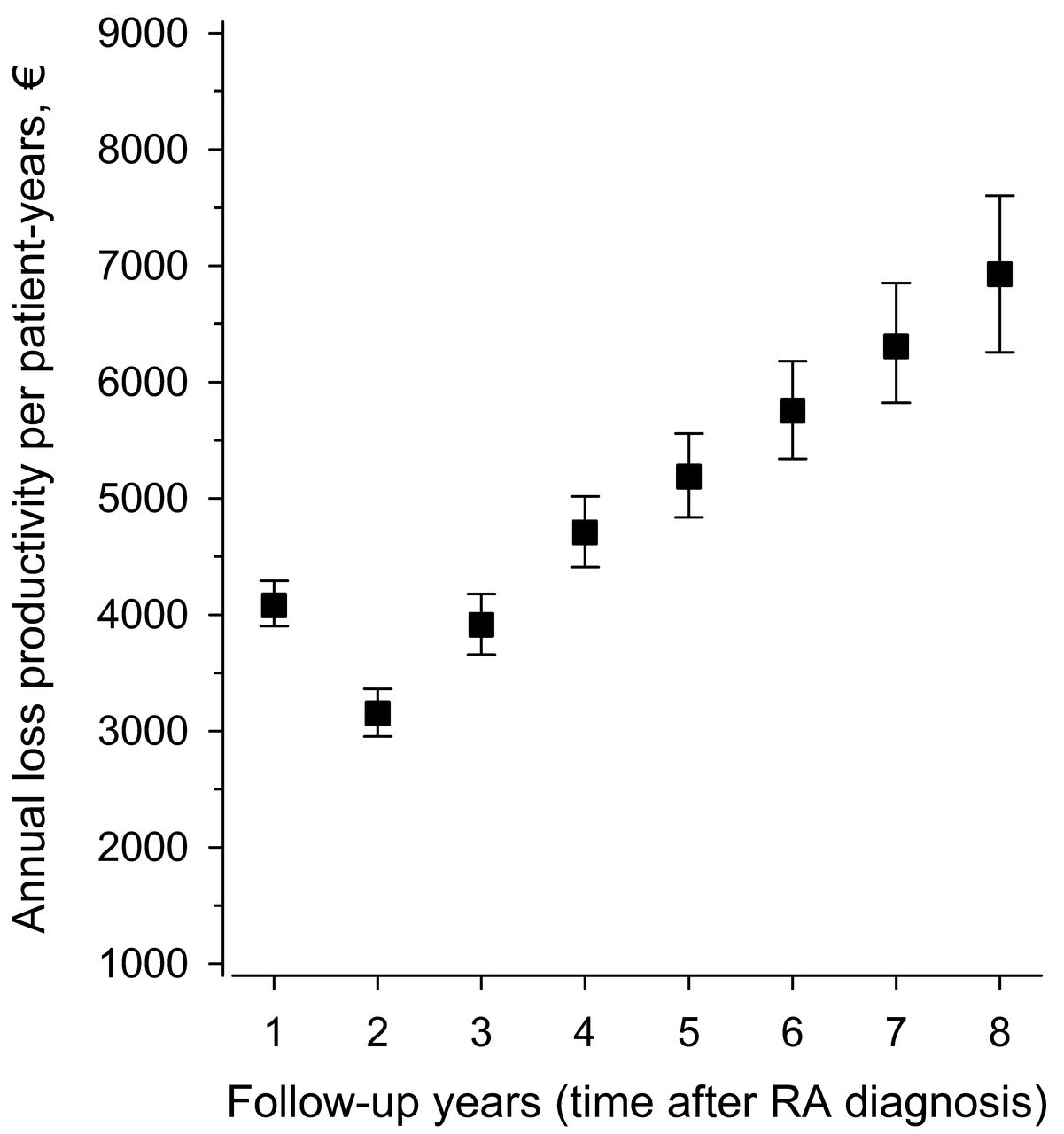
Development of RA-related productivity loss costs (€) with bootstrapped 95% CI over time in patients with early RA at baseline. RA: rheumatoid arthritis.
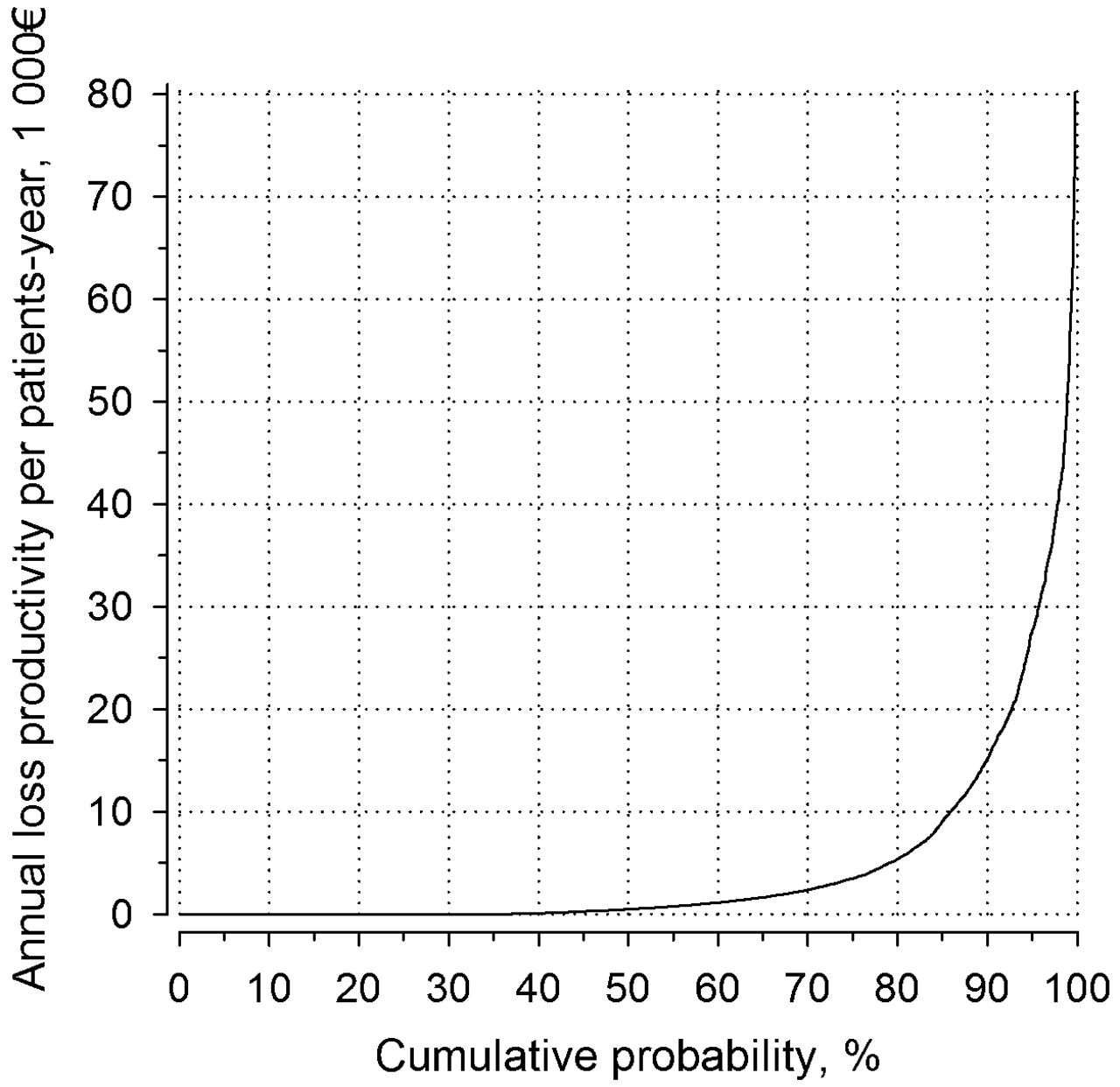
The cumulative probability plot indicating the cumulative percentage of patients with productivity losses and the amount of annual productivity loss.
Associations with productivity losses
Age and positive RF status of patients were significantly associated with the probability of work absence (Table 1). Among those patients with registered absenteeism days, sex difference was observed in the cumulative productivity losses. In addition, the early initiation of active drug treatments significantly reduced (adjusted for sex, age, and positive RF status) the expected PC in comparison with the situation of no active drug treatment during the first 3 months after the RA diagnosis.
Hurdle model of effect of available factors on the probability of work absenteeism (OR) and related cumulative PC costs (IRR) when compared with no treatment during the first 3 months after rheumatoid arthritis diagnosis.
DISCUSSION
Our study showed that the longterm productivity losses because of absenteeism and permanent WD increase significantly in parallel with years elapsing after RA diagnosis. A similar gradually increasing trend has also been observed in previous studies from Sweden, a country with a social security system similar to Finland6,7,8,9. Further, the majority of these PC are incurred by a small proportion of patients. This finding corresponds with a recent previous study also from Sweden, reporting a positively skewed distribution of total costs (i.e., about 13% of the patients with incident RA accounted for 50% of the annual total cost including both direct cost and PC)10. In our study, the majority of these high-cost patients were those who received permanent WD pensions during the followup. From the clinical point of view, these above findings highlight the importance of allocating sufficient resources for early and targeted treatment of RA11, as well as the need for novel (in addition to already known3,12,13,14) subjective and objective predictors that help to recognize those patients with early RA at high risk of permanent WD.
The PC estimates reported in our present study are on average (i.e., €4800 per patient-yr) somewhat smaller than previously reported. However, the use of the national average gross wage estimate yielded a higher productivity loss estimate (i.e., €6619 per patient-yr in 2013 euros). This estimate is relatively close to an estimate reported in a previous systematic review by Franke, et al15, where PC because of absenteeism and early retirement were estimated to be on average €6467 (in 2006 euros) per patient-year. Discrepancy between our patient-specific and national average estimates may indicate that the earning capabilities of the patients were affected by RA, resulting in a lower earnings trajectory than what would have been seen if they never had the disease.
To date, the majority of the PC studies has been based on cross-sectional data15. In this respect, our study, including all Finnish patients with early RA between years 2000–2007, provides additional evidence about the longitudinal economic burden of RA as a function of disease duration. However, we are aware that use of the friction-cost method as an alternative valuation method16, which takes account of productivity loss only within a defined friction period if absent workdays exceed the period, would lead to a reduction in the estimated costs of the productivity losses. Nevertheless, the observed trends and associations are still apparent regardless of the valuation method used. In addition, using registered rather than self-reported data for the estimation of PC eliminated the potential effect of recall bias17. On the other hand, the available national registers provide no data about short sick leaves (≤ 10 days) because the sickness allowance is only paid after the completion of a waiting period consisting of the first day of work incapacity and the following 9 weekdays (including Saturdays). Thus, in that respect, our results may underestimate the total productivity loss burden of RA. Therefore, there is a clear need for further studies assessing the involvement of short-term absenteeism in Finnish patients with early RA. Further, we were not able to estimate the PC caused by presenteeism, which is potentially one of the main cost drivers in the early course of RA18. One further limitation is that we were not able to estimate the effects of multiplier effects or compensation mechanisms on the PC19.
We found that several factors, i.e., age, positive RF status, and early initiation of drug therapy, were significantly associated with the expected longterm PC. The age of patients increased the odds of incidence of PC by 2% for every year of increased age. The amount of PC loss increased even more, i.e., by 5% for every year of increased age. This apparent discrepancy may exist partly because salaries usually increase with age and competence of workers, but also by the worsening of RA symptoms as an individual ages. In fact, this association between older age and the magnitude of productivity losses has also been reported previously20.
We did not find any significant difference in productivity losses between men and women. However, among those who had observed PC (i.e., PC > €0), significant sex difference was found to indicate higher PC losses among men. A similar numerical trend was observed in the Finnish Rheumatoid Arthritis Combination Therapy Trial including 162 patients with RA who were available for the workforce20. The initiation of drug therapy during the first 3 months after RA diagnosis significantly reduced the expected longterm PC (when compared with no active drug treatment during the same period). This is an interesting finding, because delay of active drug therapy during the first 3 months after the RA diagnosis could be assumed to be an indication that the patient has less debilitating inflammatory activity (i.e., these patients could be expected to have a better work ability and hence a lower risk for productivity losses), but in the long run, these patients do seem to experience a higher risk for work absenteeism and permanent WD. One factor that may increase the significance of this finding is that all plausible confounding (i.e., patients with more severe disease are more likely to receive more intensive treatment) would have been expected to reduce this apparent effect of the benefits of early drug therapy. However, this was not observed in our present study (i.e., patients with more severe disease should also have more absenteeism days, and thus more PC). Naturally, this finding needs to be interpreted with caution since there are many potentially uncontrolled confounders that may modify the obtained results, i.e., no clinical, radiographic, or details of employment data were available to analyze these observed associations more closely. Nevertheless, the finding gives support for the concept that there is “a window of opportunity” in early RA11, and that prompt initiation of active therapy seems to exert positive effects in the long run, not only to relieve the patient’s symptoms but also to improve economic productivity.
The longterm PC because of absenteeism and permanent WD increase significantly in parallel with years elapsing after RA diagnosis. Further, the majority of these PC are incurred by a small proportion of patients, highlighting the importance of identifying those patients located in the heavy right tail of the skewed PC distribution.
Footnotes
Supported by a grant from the Yrjö Jahnsson Foundation (grant number 6575).
- Accepted for publication August 27, 2016.








{kind=link}
{kind=link}
{kind=link}