

Abstract
Objective. To develop an innovative stepped patient decision aid (StDA) comparing the benefits and harms of 13 nonsurgical treatment options for managing osteoarthritis (OA) and to evaluate its acceptability and effects on informed decision making.
Methods. Guided by the Ottawa Decision Support Framework and the International Patient Decision Aid Standards, the process involved (1) developing a decision aid with evidence on 13 nonsurgical treatments from the 2012 American College of Rheumatology OA clinical practice guidelines; and (2) interviewing patients with OA and healthcare providers to test its acceptability and effects on knowledge and decisional conflict.
Results. The StDA helped make the decision explicit, and presented evidence on 13 OA treatments clustered into 5 steps or levels according to their benefits and harms. Probabilities of benefits and harms were presented using pictograms of 100 faces formatted to allow comparisons across sets of options. It also included a values clarification exercise and knowledge test. Feedback was obtained from 49 patients and 7 healthcare providers. They found that the StDA presented evidence in a clear manner, and helped patients clarify their values and make an informed decision. Some participants found that there was too much information and others said that there was not enough on each treatment option.
Conclusion. This innovative StDA allows patients to consider both the evidence and their values for multiple options. The findings are being used to revise and plan future evaluation. The StDA is an example of how research evidence in guidelines can be implemented in practice.
Osteoarthritis (OA) is the most prevalent form of arthritis worldwide and may lead to pain, disability, sleep disturbance, work disability, depression, and fatigue1,2,3,4,5. There is no cure for OA, but a myriad of treatments are available to help manage OA symptoms, including pharmacological and nonpharmacological options6. Patients with OA may have difficulty deciding on the optimal regimen for them, because of the complex array of treatment options6 and the need to weigh benefits and harms. Decisions also need to be reconsidered as the OA severity increases7. Similarly, healthcare providers face challenges in providing support to patients making decisions about their OA treatment8. These include insufficient time to communicate the evidence or to enable patients to clarify their values for a large number of options.
Patient decision aids (DA) are tools that present evidence in formats that are user-friendly and designed to prepare patients for making decisions with their healthcare provider. A systematic review of 115 trials of patient decision aids shows that they improve patients’ knowledge, increase patient participation in decision making, and are more likely to result in choosing options that match their informed values9. However, few DA compare a wide range of treatment options, there is limited evidence on their effect10,11,12, and none are available to assist patients with OA in sifting through all of the available information by presenting the probabilities of benefits and harms for each option.
The objective of our study was to develop an innovative stepped patient DA (StDA) facilitating the comparison of benefits and harms across 13 nonsurgical treatment options for OA, and to assess its acceptability and effects on informed decision making among patients with OA.
MATERIALS AND METHODS
Development of the StDA
The StDA was designed by a multidisciplinary team of researchers, clinicians, and a patient representative with combined expertise in rheumatology, rehabilitation, nursing, clinical epidemiology, DA development, arthritis self-management, and knowledge translation, using the Ottawa Decision Support Framework (ODSF) and following the International Patient Decision Aid Standards (IPDAS)13. Consultations with patients were also conducted before developing the StDA. The ODSF is one of the most commonly used frameworks to develop DA14 (found at https://decisionaid.ohri.ca/odsf.html). The StDA was primarily developed for use in primary care, but could also be used in rheumatology practice to help patients make decisions about OA therapy at the time of diagnosis, as well as over time, as the disease progresses and new treatment options are considered. It compares the benefits and harms of 13 nonsurgical treatment options for OA chosen according to (1) the European League Against Rheumatism and Osteoarthritis Research Society International OA clinical practice guidelines’ expert panels15,16,17,18; (2) the 2012 American College of Rheumatology (ACR) OA clinical practice guidelines6, which used the Cochrane Collaboration methodology and the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) working group approach19; and (3) their commercial availability in Canada and the United States. Outcomes were chosen based on their relevance for patients with OA according to the literature, and their inclusion in the ACR OA clinical practice guidelines6. To improve knowledge and ensure accurate risk perceptions, probabilities of benefits and harms of the options were visually summarized9,20.
Acceptability evaluation and effects on informed decision making
According to the IPDAS, this evaluation represents the α testing of this newly developed StDA. Face-to-face or telephone interviews were conducted with patients with OA recruited from the Ontario Hip/Knee Arthritis Cohort, as well as from the broader community, using newspaper advertisements in both urban and rural areas in the Toronto region. Individuals were eligible if they spoke and understood English and had symptomatic OA diagnosed by their physicians. They were excluded if they were or had been on a list for total joint replacement surgery. Canadian healthcare providers from nursing, pharmacy, physical therapy, occupational therapy, and family medicine with experience in OA management were interviewed.
The StDA was provided to participants and was read aloud by the interviewer. As they were completing it, participants were encouraged to give their impressions on its format and content. The interviewer also asked a series of questions and recorded participants’ answers. Participants answered questions on acceptability, including perceptions of clarity and balance in presentation of benefits and harms21, and preparation for decision making22. Participants provided information on their knowledge about the treatment options and decisional needs based on the SURE (Sure of myself; Understand information; Risk-benefit ratio; Encouragement) screening test23,24. Further information on the measures can be found in the data supplement, available online at jrheum.org. Additional open-ended questions asked about participants’ overall impressions of the StDA, strengths and areas for improvement, and potential helpfulness of the StDA, from patients’ and healthcare providers’ perspectives. The Flesch-Kincaid readability tests were used to assess the readability ease and the US grade level required to understand the StDA.
Data analysis
All data were entered into an Excel spreadsheet and analyses were performed using the Statistical Package for Social Statistics. Quantitative analyses were conducted for closed-ended questions and descriptive statistics were used to summarize the acceptability of the StDA and its effects on informed decision making. Content analysis was used for the open-ended question responses. A transcript of the interviews was read and coded into themes by a team member. They were then analyzed with an initial phase of open coding followed by a process of condensation into overarching themes. Themes were then agreed upon by 2 team members.
RESULTS
Components of the StDA
The StDA contained (1) a self-assessment of severity of OA pain and disability, designed to help patients understand the disease, assess symptoms and their effect on the patient’s life, as well as determine whether their current treatment management is optimal, or if they wished to change their current treatment plan; (2) information on the benefits, harms, and side effects of 13 nonsurgical treatment options for OA, categorized into 5 steps or levels based on the probability of improving pain and function versus the risk of harms/side effects; (3) a values clarification exercise in which common reasons for choosing an option were elicited using a 6-point importance rating scale (0 to 5); (4) a 5-item knowledge test; and (5) a 4-item assessment of decisional conflict.
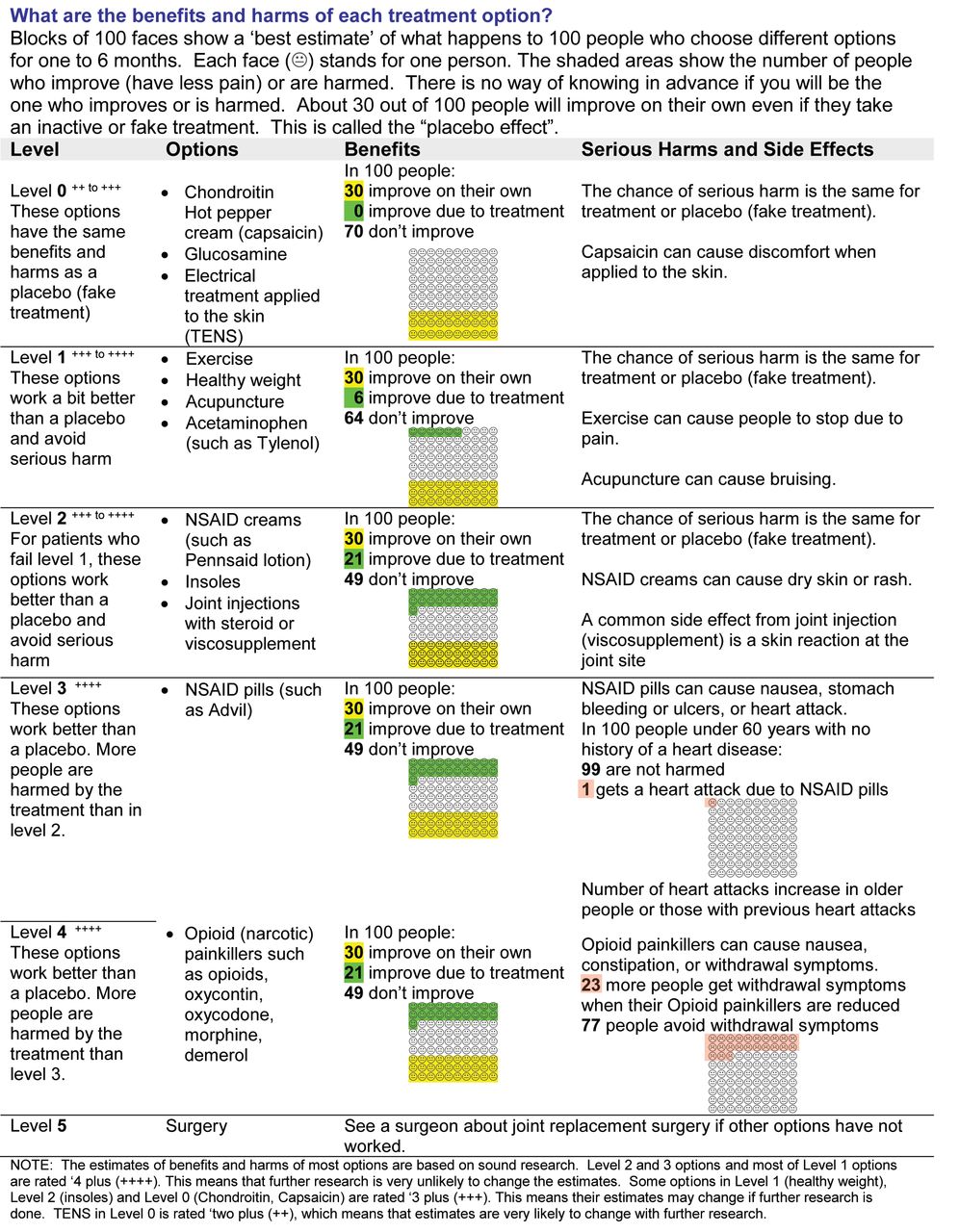
Summary of findings tables presenting the strength and quality of the evidence used in the StDA can be found in the ACR OA clinical practice guidelines’ supplementary documents6. Probabilities were determined by calculating the absolute differences between the treatment and control groups and were represented in pictograms of 100 faces (Figure 1). Although the options were categorized to reflect increasing levels of benefit and risk, patients and practitioners are encouraged to select the options in the order reflecting their personal circumstances, disease characteristics, comorbidities, and values and preferences. When evidence for treatment benefit compared with placebo was equivocal (equivalent to 30% of individuals with clinically reduced pain), and there was no risk of serious harms, treatments were included in Level 0 [e.g., chondroitin, glucosamine, capsaicin cream, and transcutaneous electrical nerve stimulation (TENS)]. Treatments providing small benefits of around 5% over that of placebo and no appreciable risk of serious harm were placed in Level 1 (e.g., exercise, healthy weight, acupuncture, acetaminophen). Treatments with over 20% of individuals improving and no appreciable harms were in Level 2 (e.g., nonsteroidal antiinflammatory creams, insoles, joint injections). Levels 3 and 4 represented treatment options with similar benefits to Level 2, but also greater harms (e.g., oral nonsteroidal antiinflammatory drugs with their increased risk of gastrointestinal bleeds and heart attacks). Level 5 consisted of a referral to a surgeon for consultation about joint replacement. No pictogram was used for Level 5 because it was beyond the scope of this StDA. Information about costs was not provided because they vary according to geographic regions and patients’ insurance coverage. However, costs would be mentioned in the values clarification exercise.

Visual summary of the evidence shown in the stepped decision aid. NSAID: nonsteroidal antiinflammatory drugs; TENS: transcutaneous electrical nerve stimulation.
The methodological quality of the evidence appraised with GRADE was indicated in the StDA. Although most options were of high quality, some options in Level 0 (chondroitin, capsaicin), Level 1 (healthy weight), and Level 2 (insoles) were rated as moderate quality. Evidence for TENS in Level 0 is rated as low quality. Low or moderate quality ratings mean that estimates are less certain and are more likely to change with further research. The StDA has a Flesch-Kincaid readability ease of 68.8 and has a grade level of 7.1.
Acceptability and effects on informed decision making
A total of 49 participants (mean age 53.3 yrs) from the Ontario Hip/Knee Arthritis Cohort (n = 26), as well as from the broader community (n = 23), reviewed the StDA (Table 1). These 2 groups showed similar demographic and disease-related characteristics, except for duration of OA. This was shorter in the patients from the cohort compared to the patients from the community [mean (SD): 9.65 (7.87) vs 14.78 (9.21) yrs; mean difference (95% CI): −5.133 (−10.043, −0.222)]. Both groups showed similar results in acceptability of the StDA and effects on informed decision making, and so the results of the 2 groups were merged.
Demographic and disease-related characteristics of individuals with osteoarthritis.
Most participants (89.8%) said that the elements of the StDA were clear, although some considered it too wordy. Half of participants (55.6%) said that the StDA presented the appropriate amount of information, while 40% said information should be added and 4.4% said that there was too much information in the StDA. Half of the participants (50%) said that the information was slanted toward medical therapies, 41.7% said the information was balanced, and 8.3% said it was slanted toward self-care.
Regarding preparation for decision making, most participants (85.4%) stated that the StDA would help them consider the benefits and harms of each option, and 83.3% of participants said that it would prepare them to talk to their doctor about what matters to them. Participants also said that it would help them organize their own thoughts about the decision (77.1%) and prepare them to make a better decision (75%). They said that it would have helped them to recognize that a decision needed to be made (68.1%), that it would have helped them to realize that the decision depends on what matters most to them (58.7%), and that it would be useful in helping them to think about how involved they wished to be in the decision (50%). Just over half of participants (57.4%) thought that the StDA would have been useful when making a decision about OA therapy and 55.3% would recommend it.
The mean score on the knowledge test was 82.6% (95% CI: 76.3%–88.8%; Table 2). According to the SURE test16,17, 84.8% of participants were clear about which benefits and harms matter most to them, 69.2% had enough information, 64.4% had enough support to make a decision, and 60% felt sure about the best choice for them after using the StDA. Half of participants gave positive answers to all 4 questions of the SURE test.
Results of the knowledge test given at the end of the decision aid.
Information about participants’ currently used OA treatments, values and preferences, preferred treatment option, and confidence in following the plan are shown in the data supplement, available online at jrheum.org. It shows that participants mostly used low-risk treatments (e.g., exercises, insoles, healthy weight, over-the-counter treatments) to manage their OA. Many participants wished to avoid side effects of medications (e.g., bleeding ulcers, heart attack) and valued pain relief.
Healthcare provider feedback
Seven healthcare providers, in the fields of nursing (n = 2), pharmacy (n = 2), physical therapy (n = 1), occupational therapy (n = 1), and family medicine (n = 1) participated in interviews. Four of them stated that the StDA included an adequate amount of information, 2 said that treatment options were not described fully enough (e.g., brand names of drugs, various types of exercises), and 1 found that some elements of the StDA were not described enough while others were too detailed. All 7 healthcare providers supported the potential of the StDA to help patients consider the benefits and harms of each option, assess what matters most to them, and prepare them for discussion with their doctor. Six healthcare professionals said they would recommend these for all patients; the remaining one would recommend it only if used with guidance from a healthcare provider.
DISCUSSION
An StDA comparing 13 nonsurgical treatment options for OA and guiding patients on how to clarify their values was developed using recognized frameworks and evaluated for its acceptability and effects on informed decision making. To our knowledge, this StDA is the first to use a stepped approach to presenting evidence-based information with benefit/harm probabilities for multiple nonsurgical options for managing OA. It presents probabilities not only for pharmacological treatment options, but also nonpharmacological ones that are often underused but nevertheless important for patients to manage their OA. This StDA represents an innovative way to present evidence from multiple options presented in guidelines for use in clinical practice, while concurrently taking into account patients’ values and preferred option. Further, assessing evidence for quality using the GRADE approach19 helps to make it understandable to patients and healthcare providers25.
Most participants found that the StDA was clear and that it helped them to clarify their values and to make an informed decision. To be supported through their journey with OA, it was important for patients to be able to compare the benefits and harms of a wide range of treatment options that may be used over the course of the disease. As one participant said, the StDA is a way to “walk you through a journey with OA,” because it presents options in a logical progression.
The clear visual presentation of evidence-based information seems to improve knowledge about treatment benefits and harms, which may help to prevent or correct misconceptions about these options. The readability was adequate because the IPDAS suggest that DA be written at a grade 8 level or lower.
The proportion of patients recommending the StDA was lower than expected, indicating that future versions will need to address issues. For example, there is too much general information but not enough on each specific treatment option. Patients highlighted the need for more personalized information and decision support from a coach or healthcare provider. These results suggest that participants in our study may be too educated and experienced (i.e., high education level, longer disease duration, high use of low-risk treatments) to fully appreciate the value in this tool, a possibility that is consistent with another study26. Further, it may be difficult for patients to integrate the information presented in probabilities to make a decision, especially when there are many treatment options.
Because OA management is complex and changes according to the stage of disease, an online version of the StDA may make it easier to deliver more layered levels of information. Patients are at different steps in the treatment spectrum, and so we recognize that not all of them would be interested in seeing more detailed information for all the options. Parsing the information about options into sections that can be selected by the patient and healthcare provider will help address individual needs and reduce the complexity of the StDA. Further, with these briefer, somewhat more detailed patient decision aids, providing access to a healthcare provider to review the StDA can verify understanding and provide the opportunity for patients to communicate their values and preferences for managing OA.
The next steps consist of modifying the StDA according to this feedback, and evaluating it in a real-life community setting to monitor its effect on decision making at the time of diagnosis as well as over time. Future studies should also evaluate how people cope with uncertainty, especially stemming from using probabilities. Results will need to be evaluated among a wide variety of patients in terms of age, education level, sex, and stages of the disease. Incorporating feedback from patients with OA and healthcare providers in the iterative development of this StDA will help ensure its integration into clinical practice.
ONLINE SUPPLEMENT
Supplementary data for this article are available online at jrheum.org.
Acknowledgment
The authors thank Melissa French for coordinating data collection in Toronto, Andrea McClintock for interviewing the patients, and Anton Saarimaki for designing the format and visual presentation of the tool.
Footnotes
Study funded by the Canadian Arthritis Network Discovery Advancement Program.
- Accepted for publication June 7, 2016.








{kind=link}