

Abstract
Objective. The Canadian Vasculitis research network (CanVasc) is composed of physicians from different medical specialties and researchers with expertise in vasculitis. One of its aims is to develop recommendations for the diagnosis and management of antineutrophil cytoplasm antibody (ANCA)-associated vasculitides (AAV) in Canada.
Methods. Diagnostic and therapeutic questions were developed based on the results of a national needs assessment survey. A systematic review of existing non-Canadian recommendations and guidelines for the diagnosis and management of AAV and studies of AAV published after the 2009 European League Against Rheumatism/European Vasculitis Society recommendations (publication date: January 2009) until November 2014 was performed in the Medline database, Cochrane library, and main vasculitis conference proceedings. Quality of supporting evidence for each therapeutic recommendation was graded. The full working group as well as additional reviewers, including patients, reviewed the developed therapeutic recommendations and nontherapeutic statements using a modified 2-step Delphi technique and through discussion to reach consensus.
Results. Nineteen recommendations and 17 statements addressing general AAV diagnosis and management were developed, as well as appendices for practical use, for rheumatologists, nephrologists, respirologists, general internists, and all other healthcare professionals more occasionally involved in the management of patients with AAV in community and academic practice settings.
Conclusion. These recommendations were developed based on a synthesis of existing international guidelines, other published supporting evidence, and expert consensus considering the Canadian healthcare context, with the intention of promoting best practices and improving healthcare delivery for patients with AAV.
- ANCA-ASSOCIATED VASCULITIS
- DRUG THERAPY
- QUALITY OF HEALTHCARE
- PRACTICE GUIDELINES
- CONSENSUS DEVELOPMENT CONFERENCE
- VASCULITIS
Systemic vasculitides are a heterogeneous group of potentially life-threatening disorders characterized by the inflammation of blood vessels with resultant ischemic events, hemorrhagic events, or both. The 2012-revised nomenclature of Chapel Hill distinguishes small, medium, and large vessel vasculitides according to the caliber of the vessels predominantly affected1,2. Some small vessel vasculitides can be associated with the presence of serum antineutrophil cytoplasm antibodies (ANCA). These vasculitides include granulomatosis with polyangiitis (GPA; formerly known as Wegener’s granulomatosis), microscopic polyangiitis (MPA), and eosinophilic GPA (EGPA; formerly known as Churg-Strauss syndrome). Collectively, these 3 small vessel vasculitides are referred to as ANCA-associated vasculitides (AAV).
The rarity and the heterogeneous feature of AAV mean that the management of individual patients can be extremely challenging and may vary markedly across different geographical regions and medical disciplines. The annual incidence rates of GPA and MPA are each around 5–10 per million inhabitants, and that of EGPA around 1–4 per million inhabitants3,4,5. In the past 7 years, several guidance documents have been developed in Europe, Australia, and Asia in an attempt to outline the optimal evidence-based management of AAV6,7,8,9,10,11,12,13. However, these existing guidelines were initially developed prior to 2010 and most have not yet been updated even though significant therapeutic developments have occurred in recent years, particularly regarding the biologic agent rituximab (RTX). In addition, these existing guidelines obviously cannot take into account the specificities of healthcare system delivery, access to services, and drug treatments in Canada.
The Canadian Vasculitis research network (CanVasc) was created in November 2010 and its core committee includes physicians of different specialties, though primarily rheumatologists and nephrologists. One of the major objectives of CanVasc was the development of recommendations for the management of patients with vasculitis. It was first decided to develop and focus on recommendations for AAV. This document reports the recommendations and statements consensually developed by the CanVasc recommendation working group (all members of this group are listed as coauthors).
These recommendations and statements were based on the highest quality of evidence available at the time when the working group undertook this review, and are intended to promote best practices and improve healthcare delivery for persons with AAV. However, they should not be interpreted as rigid or legal standards, and they are not meant to replace the clinical judgment of specialists and other healthcare providers trained in AAV, who must always act according to the individual needs of the patient and the unique clinical circumstance.
MATERIALS AND METHODS
Precise objective
The aim was to develop a document to provide guidance and structured recommendations for the management of AAV within Canada based on a synthesis of existing international guidelines, supporting evidence, and expert consensus of a national Canadian AAV clinical and research network (CanVasc).
Target patient population
The target patient population for these recommendations is patients with, or suspected of having (for the diagnostic aspects of these recommendations), AAV according to prior and current classification criteria1,2,14,15 and/or by a healthcare provider.
Target audience and users
The target audience of these recommendations is rheumatologists, respirologists, nephrologists, and general internists involved in the management of AAV in community and academic practice settings. This document may serve as a point of reference on the management of AAV in Canada for other specialists, medical students, specialists in training, general practitioners, and all other healthcare professionals occasionally involved in the management of patients with AAV. These recommendations may also be of interest to those involved with AAV management at the provincial and federal government levels, and decision makers.
Health questions covered
These recommendations cover the main domains of the general management strategies for AAV (GPA, MPA, and EGPA), including their diagnosis; treatments with glucocorticoids (GC), traditional immunosuppressants, and biologic agents; and followup. They do not address other non-AAV vasculitides such as polyarteritis nodosa (PAN) or isolated vasculitic peripheral neuropathy.
Needs assessment questionnaire
As done previously for the development of other Canadian recommendations16,17,18, a national needs assessment questionnaire was first disseminated between May and October 2012 to Canadian healthcare professionals from different medical specialties involved in vasculitis patient management. The objectives were to identify the specific areas of need and possible knowledge gaps, and outline key questions, uncertainties, and challenges in the management of patients with AAV.
The key messages were that 89% of respondents did not have hospital/center-written protocols for the management of AAV and 77% of respondents did not refer patients to a vasculitis referral center (at least for second opinion)19. The top 5 issues pertaining to the management of AAV, which respondents said would be helpful if addressed by AAV recommendations, were as follows (in order of priority): (1) remission induction, (2) treatment of refractory patients, (3) treatment of relapses, (4) indications and use of biologics, and (5) remission maintenance therapy.
Review of existing guidelines
The international existing clinical practice guidelines and consensus statements on the management of AAV (exclusively or as part of a general vasculitis guidance document) published in English or French between 2006 and August 2013 were then reviewed. We considered 7 such documents or sources: Kidney Health Australia: Caring for Australasians with Renal Impairment Guidelines (CARI); British Society for Rheumatology (BSR); French Vasculitis Study Group (2007 FVSG); Japanese Circulation Society (JCS); European League against Rheumatism/European Vasculitis Society (EULAR/EUVAS); the International Society of Nephrology/Kidney Disease: Improving Global Outcomes (KDIGO); and the 2011 British recommendations for the use of RTX in ANCA-associated vasculitis (Guerry, et al)6,7,8,9,10,11,12,13. We also included 2 additional guidelines that were published during the development of these recommendations: (1) FVSG recommendations for the use of RTX for the induction and maintenance treatments of adult AAV (2011 FVSG), and (2) the updated BSR guidelines for the management of adults with AAV (2014 BSR)20,21.
Additional literature search
To access the more recent clinical trial data not referenced in published guidelines, we performed a PubMed Medline search using the terms “vasculitis” or “granulomatosis with polyangiitis” or “microscopic polyangiitis” or “eosinophilic granulomatosis with polyangiitis” or “Wegener’s” or “Churg Strauss”, looking for all therapeutic studies (randomized clinical trials, retrospective, and cohort studies) of AAV published since the 2009 EULAR/EUVAS recommendations and until May 2014, in English or in French, excluding case reports. We reviewed the reference lists of our search results to ensure no relevant or important studies were missed. We also performed a manual search of relevant abstracts presented at the American College of Rheumatology (ACR), EULAR/EUVAS, and BSR scientific meetings since 2008 and until May 2014. Finally, we also searched the Cochrane library without date restriction in August 2013 and again in May 2014, citing “vasculitis” as the principal search term22,23.
Development of the recommendations and working group reviews
We first constructed 37 recommendations (Figure 1), specifically addressing the areas of need as identified by the needs assessment questionnaire and additional questions identified from the CanVasc recommendation working group. We described the rationale behind each recommendation, and where relevant, how and why it had been modified according to prescribing regulations and practice setting within Canada. For each recommendation, we also presented existing recommendations/guidance from other societies. The level of evidence available for each recommendation was categorized and graded according to the criteria previously endorsed by EULAR/EUVAS (Table 1A, Table 1B)6,24.
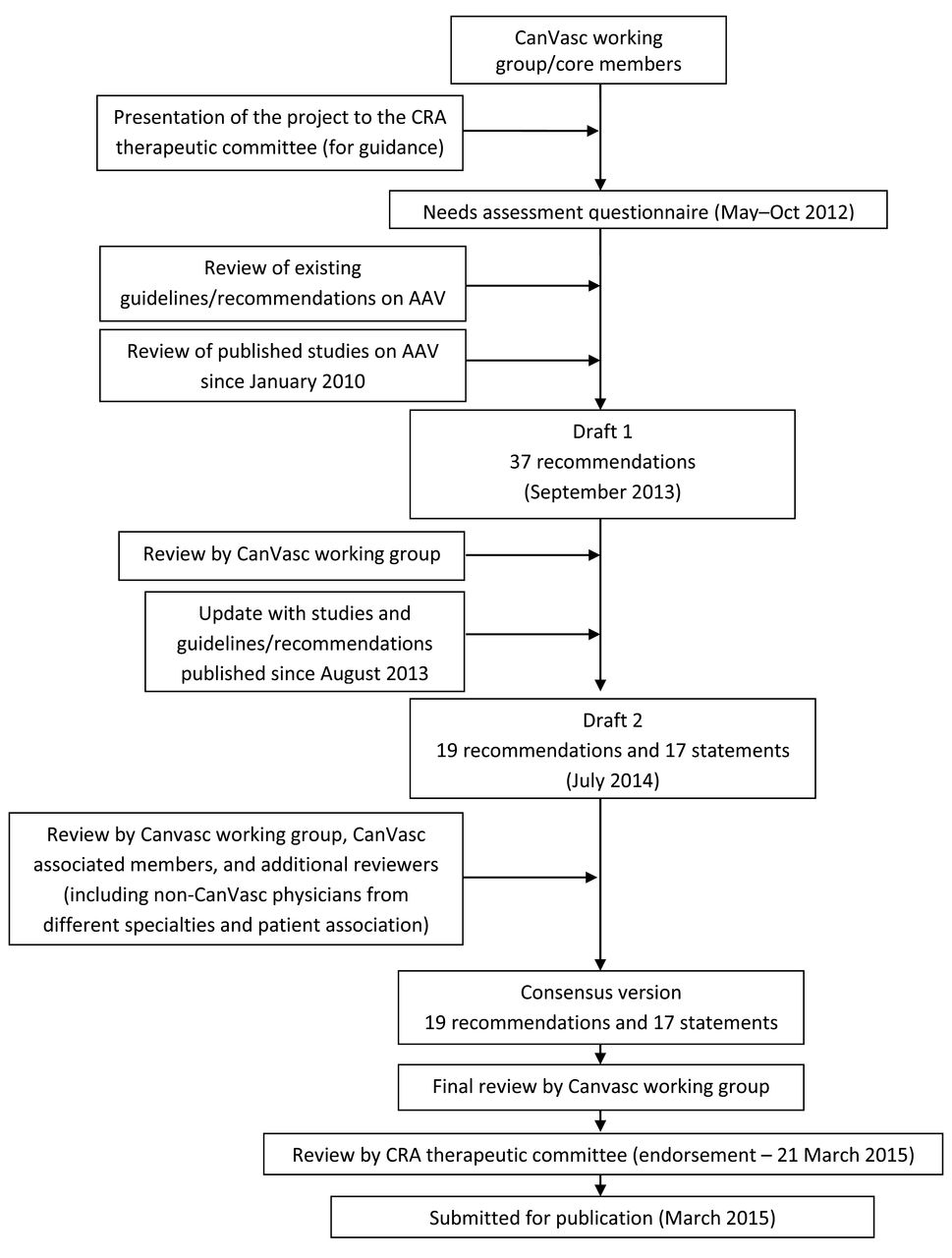
Flowchart of development steps of CanVasc recommendations. CanVasc: Canadian Vasculitis network; CRA: Canadian Rheumatology Association; AAV: antineutrophil cytoplasm antibody-associated vasculitides.
Using a modified Delphi method, each member of the CanVasc recommendation working group was asked to vote, review, and comment on the grading and wording of each recommendation of the first draft of this document. A teleconference was held on November 22, 2013, to review the comments and reach consensus on all debated recommendations, especially those not agreed upon by > 80% of the reviewers. It was agreed that recommendations not related to treatment should not be graded because there was no strong evidence or available studies to support them.
The recommendations were then revised and rewritten, resulting in a total of 19 recommendations (with grading for evidence) and 17 statements (expert consensus without grading for evidence). Information from the FVSG recommendations for the use of RTX for induction and maintenance treatments of adult AAV and the 2014 update of the BSR guidelines for the management of adults with AAV were then added20,21. The revised recommendations and statements were distributed on July 14, 2014, for review to the working group and a broader spectrum of reviewers, including members of several professional medical societies and specialists [the Canadian Rheumatology Association (CRA), Canadian Thoracic Society, and Canadian Society of Nephrology], and the Canadian support group for vasculitis patients (Vasculitis Foundation Canada). Their comments were gathered and discussed with the CanVasc recommendation working group during a second teleconference (October 9, 2014) to reach consensus on the final version of this document. This document was then reviewed by the CRA Guidelines Committee and endorsed on March 21, 2015, for a period of 3 years; it was then submitted for publication to both The Journal of Rheumatology and the Canadian Journal of Kidney Health and Disease.
Appendices
The appendices (Appendix 1; other appendices available online at jrheum.org as supplementary data) include tools for the practicing physicians for diagnosis, assessment, monitoring, and prescribing. The content of these appendices was also reviewed and commented on by the working group. Because local prescribing and monitoring practices for AAV may vary, this Appendix (Appendix 1; other appendices available online at jrheum.org as supplementary data) must be considered as an aid for AAV healthcare providers in implementing the recommendations.
Meeting organization
These recommendations were developed by Internet, through phone conferences and e-mail, as well as during the regular administrative and business meetings of CanVasc core members.
Funding and conflict of interest
The development of these recommendations was entirely self-funded by CanVasc (to cover the costs of the teleconferences and online surveys). None of the authors received any fees, grants, or emoluments for the development of these recommendations. No funding support from pharmaceutical companies was received; no representatives of pharmaceutical companies were involved at any step in the development of these recommendations. Potential conflicts for each working group member including industry funding, consultancies, commercial interests, and direct involvement in any guidelines included in the systematic review are listed in Appendix 9, available online at jrheum.org as supplementary data.
Dissemination strategies and applicability
The present document was prepared following the principles outlined by the AGREE II instrument V1 (Appraisal of Guidelines for Research and Evaluation; www.agreetrust.org)25,26. The recommendations and the Appendix (Appendix 1; other appendices available online at jrheum.org as supplementary data), including tools to aid healthcare providers in the management of patients with AAV, will be made available through the CanVasc (www.canvasc.ca) and CRA websites (www.rheum.ca). The recommendations will be updated by means of a literature search and validation by the expert committee by 2018, or earlier if significant changes occur in the field of AAV.
RESULTS
Key to understanding these recommendations and statements
Each therapeutic recommendation and statement is accompanied by supporting text that reports on the expected health benefits, potential side effects and risks, and Canadian system factors that may influence their applicability. Therapeutic recommendations are presented with a level of evidence and strength (Table 2). Statements are for nontherapeutic recommendations and working group consensus, for which there is no strong supporting evidence from controlled studies; thus they are not graded. For each recommendation and statement, we also present (in the full version of this document, available online at jrheum.org as supplementary data) corresponding recommendations/guidance previously published on the same topic from other societies.
Summary table of the CanVasc recommendations and statements.
Recommendations and statements
1. Diagnosis
Statement 1. ANCA testing with ELISA and indirect immunofluorescence (IIF) methods should be performed for diagnostic purposes in patients in whom there is clinical suspicion of a systemic small- and/or medium-sized vessel vasculitis.
The AAV are systemic vasculitides that predominantly affect small vessels and can manifest in a wide variety of ways depending on the target organ(s) involved and the severity of the disease. There are currently no validated diagnostic criteria for AAV and no precise or specific diagnostic tests. The ACR criteria14,15,27 and the Chapel Hill Consensus Conference1,2 definitions are useful tools in the assessment of a patient with vasculitis, possibly AAV, but it is important to remember that these are classification criteria and nomenclature definitions, respectively, for use in clinical trials and teaching. A study to develop diagnostic and classification criteria for systemic vasculitis is ongoing28.
AAV are often, but not invariably, associated with the presence of circulating ANCA: 60% to 90% of cases of GPA and MPA are ANCA-positive. A cytoplasmic labeling pattern (cANCA) on immunofluorescence and anti-proteinase 3 (PR3) specificity on ELISA are more common in GPA, whereas perinuclear labeling pattern on immunofluorescence (pANCA) and anti-myeloperoxidase (MPO) specificity on ELISA are more common in MPA. Only 30% to 40% of cases of EGPA are ANCA-positive, mostly pANCA with anti-MPO specificity.
In the appropriate clinical setting, ANCA testing can be extremely useful in the diagnosis of AAV and should be performed by IIF, and samples positive for ANCA by IIF should be tested for PR3 and MPO by ELISA2,29,30. The sensitivities and specificities of positive tests for cANCA targeted against PR3 or pANCA targeted against MPO are high. The combination of IIF and ELISA for ANCA testing at diagnosis can be helpful to identify discordant results. For example, a positive pANCA by IIF with PR3-ANCA on ELISA can occur in cocaine-levamisole–induced vasculopathy. A positive ANCA by IIF with ELISA results other than PR3-ANCA or MPO-ANCA in ELISA may also be observed with other conditions, such as inflammatory bowel diseases, cystic fibrosis, or infections31,32,33,34. In the future, other ANCA screening techniques may be used in combination or instead of IIF and conventional ELISA, including automated image analysis of immunofluorescence patterns, “third-generation PR3-ANCA and MPO-ANCA ELISA,” and multiplex technology35.
Barriers to implementation: A diagnosis of AAV cannot be excluded on the basis of a negative ANCA test. Some Canadian centers may not have easy access to both IIF and ELISA.
Previous guidance: 2014 BSR21, CARI9,11, EULAR/EUVAS6
Statement 2. Tissue biopsy should be considered in cases of suspected AAV to confirm diagnosis.
We recommend obtaining a tissue biopsy to confirm the diagnosis and rule out vasculitis mimickers in all patients with suspected AAV, when feasible. Tissue biopsy is particularly important in patients who are ANCA-negative or in whom there is a degree of diagnostic uncertainty. Importantly, tissue biopsy should not delay treatment in obvious cases or life-threatening situations. The proportion of patients with AAV and a “positive” biopsy who demonstrate features of granuloma, vasculitis, or both has been quoted at about 70%36, but the diagnostic yield varies greatly depending on the organ biopsied (Online Appendix 1, available at jrheum.org). It is important to recognize that a negative or “nondiagnostic” biopsy does not exclude a diagnosis of AAV. This is particularly true of ENT biopsies, for which sensitivity is below 53%37. Biopsy can occasionally guide therapeutic decisions and provide valuable prognostic information. For example, a biopsy can help distinguish active renal vasculitis from renal damage in patients with deteriorating renal function and a prior history of renal involvement. However, kidney biopsy goals should be outlined before the biopsy.
Barriers to implementation: Limitations in the timely access to biopsy and biopsy results.
Previous guidance: EULAR/EUVAS6
2. Classification of disease severity in AAV
Statement 3. Patients with AAV should have the extent and severity of their disease categorized as “severe” at the time of diagnosis and in case of subsequent relapse if they have life- or major organ-threatening manifestations, to allow therapy to be tailored accordingly.
The AAV are a heterogeneous group of disorders and the clinical course can be extremely varied. Therapy should be tailored according to disease extent and severity, and we therefore propose that patients with AAV be classified according to disease severity because this will affect therapeutic indications and contraindications.
For the purpose of these Canadian recommendations, the working committee defines severe AAV by the presence of life- or major organ-threatening manifestations, including severe and progressive kidney involvement; severe alveolar hemorrhage; severe gastrointestinal, cardiac, central nervous system (CNS), and/or eye involvement(s); or any other manifestations considered severe enough to require induction treatment with cyclophosphamide (CYC) or RTX. Importantly, the recommendation working committee recognizes that these definitions are wide-ranging and not constrained.
The use of existing tools may help to classify disease severity, but should not be restrictive because there are situations in which it remains difficult to readily classify disease severity. Two tools have been previously used for classifying GPA disease extent and severity in trials: the classification into “limited” or “severe” used by the Wegener’s Granulomatosis Etanercept Trial (WGET) research group36,38, and that adopted by the EUVAS group with localized, early systemic, generalized, severe, and refractory diseases (Online Appendix 2, available at jrheum.org)39. These 2 classifications have many similarities and there are currently no data to demonstrate that either classification system is superior to the other, although the binomial WGET classification appears to the recommendation working committee to be simpler to use.
In the Rituximab for ANCA-associated Vasculitis (RAVE) trial40, patients with GPA and MPA were categorized according to the Birmingham Vasculitis Activity Score for Wegener’s granulomatosis (BVAS/WG), with severe disease being defined as the presence of 1 or more of the major BVAS/WG items or disease severe enough to require treatment with CYC. The original (1996 version) 5-factor score (FFS) is a prognostic scoring system that was developed by the FVSG and uses 5 distinct disease features that have been proven in uni- and multivariate analyses to be valuable prognostic markers in EGPA and PAN41, and has been further validated in MPA42. These 5 prognostic factors include vasculitis-related cardiomyopathy, CNS involvement, severe gastrointestinal tract symptoms, renal insufficiency (creatinine > 1.58 mg/dl or 140 μmol/l), and proteinuria (> 1 g/day). An FFS = 1 was associated with a 25.9% 5-year mortality and a FFS ≥ 2 (2 or more factors present) was associated with a 45.9% 5-year mortality rate (Online Appendix 2, available at jrheum.org). The 2009-revised FFS has yet to be validated and therefore cannot be used similarly to score disease severity in EGPA to guide therapy (Online Appendix 2, available at jrheum.org)43.
Finally, it is important for treating physicians to regularly assess disease severity because a patient’s disease characteristics may change from their baseline presentation and therapy may have to be adjusted accordingly.
Barriers to implementation: None.
3. The role of referral centers for vasculitis
Statement 4. Patients with AAV, particularly those with challenging disease, should be managed at or in collaboration with a referral center for vasculitis.
The AAV are a heterogeneous and rare group of disorders and it can be difficult for general internists, rheumatologists, nephrologists, and other subspecialists to maintain expertise in their management. We therefore recommend that patients with vasculitis be managed in collaboration with a referral center for vasculitis when possible (see Online Appendix 8 for list and location of all CanVasc centers, available at jrheum.org). Patients presenting with unusual manifestations of AAV and those with refractory disease may especially benefit from the direct input of a referral center for vasculitis, where there may be better access to subspecialists as well as access to clinical studies and trials. There is a continuous need for such studies on these diseases. As an integral part of this document, 2 areas of uncertainty in which observational, mechanistic, and/or therapeutic randomized controlled trials (RCT) would significantly inform clinical practice and increase knowledge are described in the following section.
Barriers to implementation: There is a shortage of healthcare providers trained in the assessment and management of patients with AAV in Canada. The creation of CanVasc and the identification of CanVasc centers and collaborators across Canada (Online Appendix 8, available at jrheum.org) aimed to decrease the lag between identification and referral of patients with AAV.
4. Remission induction for newly diagnosed disease
4.1 Remission induction in severe (organ- and/or life-threatening) newly diagnosed disease
Recommendation 1. We recommend remission induction therapy with a combination of high-dose GC and CYC in patients with severe newly diagnosed GPA, MPA, or EGPA.
We recommend remission induction with CYC administered either orally or intravenously (IV) for 3–6 months (see Online Appendix 3 for CYC prescribing protocols, available at jrheum.org). A metaanalysis of the 3 RCT that compared continuous oral versus pulsed IV CYC concluded that remission was achieved equally with one or the other22,44,45,46,47, but continuous oral CYC is associated with a lower rate of relapse on longer-term followup48. The use of oral CYC results in higher cumulative doses of the drug and may be associated with a worse side effect profile.
Treatment with IV CYC pulses should be accompanied by adequate oral or IV hydration and oral or IV antiemetic agents. Patients receiving oral CYC should also be advised to ensure adequate oral hydration. Oral and/or IV mesna binds and eliminates acrolein, the metabolite of CYC that can be toxic for the bladder mucosa, and can be considered in patients receiving CYC. The risk of bladder toxicity is greater with the highest cumulative doses and prolonged use of daily oral CYC49. However, evidence for the effectiveness of mesna in preventing cystitis remains limited and there is no direct evidence for its effectiveness in preventing bladder cancer in humans49.
Evidence 1B, Strength of recommendation A
Barriers to implementation: The choice of IV or oral CYC remains with the treating physician and the patient, and is often determined in Canada by the ease of access to each preparation.
Previous guidance: BSR8, 2014 BSR21, EULAR/EUVAS6, JCS10, KDIGO13
Recommendation 2. We recommend using high-dose GC with RTX as first-line remission induction therapy in patients with severe GPA or MPA in whom CYC is contraindicated or in whom CYC presents an unacceptable risk of infertility.
Two RCT have shown RTX (375 mg/m2 × 4 weekly infusions) to be noninferior to CYC at inducing remission in adults with organ- or life-threatening disease40,50. In the RITUXVAS trial (Rituximab versus Cyclophosphamide in ANCA-Associated Renal Vasculitis; n = 44), remission at 6 months was achieved in 91% and 82% of patients treated with CYC and RTX, respectively (a nonsignificant difference). In the RAVE study (n = 197), 64% of the RTX group of patients were in remission and not taking GC at 6 months compared with 54% of the CYC group (a nonsignificant difference). In both RCT, there was no evidence that RTX was a safer alternative to CYC (comparable rate of adverse events in both treatment groups, including infections). For patients in whom CYC is not tolerated or there is a valid contraindication to CYC, we recommend presenting a case for the funding of RTX, which is more expensive. We believe that preservation of fertility, when there are no clearly effective methods of doing so, is a valid justification for the use of RTX in certain individuals, especially patients of child-bearing age. The approved regimen for RTX in Canada is that used in the RAVE and RITUXVAS trials: 4× weekly infusions of 375 mg/m2. An alternate regimen of 2 × 1 g RTX infusions administered 14 days apart [as used in the treatment of rheumatoid arthritis (RA)] may be of comparable efficacy based on retrospective studies only51,52,53. We therefore recommend using the former regimen when feasible. See Online Appendix 3 for RTX prescribing protocols (available at jrheum.org).
Evidence 1B, Strength of recommendation A
Barriers to implementation: In August 2012, the Canadian Drug Expert Committee approved RTX for the induction of remission in adult patients with severely active GPA or MPA who have a history of severe reaction to CYC, in whom CYC is contraindicated, or who have failed an adequate trial of CYC. RTX is currently approved according to these criteria in Ontario, British Columbia, Alberta, Saskatchewan, Nova Scotia, and Newfoundland (Online Appendix 6, available at jrheum.org). The drug approval process is under way in the other provinces.
Previous guidance: 2014 BSR21, Guerry, et al7, 2011 FVSG20, KDIGO13
Recommendation 3. CYC dose should be adjusted in patients > 60 years of age and in those with renal impairment.
In clinical trials, CYC doses are adjusted in patients over 60 years of age and in those with renal impairment47,54,55, and this has therefore become standard practice. For oral CYC, we recommend reducing the dose by 25% for those > 60 years of age and by 50% in those > 75 years of age, as suggested in the EULAR recommendations6. Guidance for dose reductions for pulsed IV CYC is detailed in Online Appendix 3 (available at jrheum.org). Results of a French trial [CORTAGE (CORTicosteroid and cyclophosphamide-based induction therapy for patients AGEd ≥ 65 years with systemic necrotizing vasculitis)] also showed that an induction regimen with CYC pulses at a fixed dose of 500 mg per pulse was effective and safe when compared with 500 mg/m2 per pulse in patients aged over 65 years of age56.
Evidence 1B, Strength of recommendation B
Barriers to implementation: None.
Previous guidance: BSR8
Statement 5. Complete blood count (CBC) and serum creatinine level must be monitored in patients treated with CYC. In patients with abnormal CBC results, temporary withholding of CYC and subsequent dose adjustments may be necessary depending on the degree of leukopenia.
We suggest monitoring CBC and renal function at 1–2 weekly intervals initially in patients receiving oral and IV CYC. The nadir white blood cell count usually occurs 10–14 days post-CYC infusion. CYC dosing should be adjusted according to serial creatinine measurements. Online Appendix 3 details an example of a schedule for CYC monitoring (available at jrheum.org), which can be adapted based on the characteristics of each patient (e.g., age, renal disease, and comorbidities).
Barriers to implementation: None.
Previous guidance: BSR8, 2014 BSR21
Recommendation 4. We recommend that the remission induction therapy with CYC, combined with GC, last a minimum of 3 to a maximum of 6 months. Once remission is achieved, CYC should be stopped and the patient switched to a different maintenance therapy.
Remission is defined by EULAR/EUVAS as the “complete absence of disease activity attributable to active vasculitis”39. The main RCT of remission induction therapy have achieved successful remission within 3–6 months40,47,54,57, and a maximum of 6 months of CYC is now considered the norm. We recommend that patients be switched to maintenance therapy after 3–6 months of remission induction therapy with CYC, providing that remission has been achieved. If remission is delayed beyond this time, then the disease should be considered refractory and alternate therapies sought.
Evidence 1B, Strength of recommendation A
Barriers to implementation: None.
Previous guidance: BSR8, 2014 BSR21, JCS10, KDIGO13
Recommendation 5. We recommend that GC be given in adults at an initial dose of 1 mg/kg/day prednisone (PRED)-equivalent for remission induction purposes. This may be preceded by pulsed methylprednisolone (0.5 g/day to 1 g/day for 1 to 3 days) in patients with life-threatening disease and/or major organ involvement.
Most of the RCT looking at remission induction and maintenance immunosuppression therapies in adults with AAV have used an initial GC dose of 1 mg/kg/day (with maximum doses at 60–80 mg/day)32,33,34,35, and this has become standard practice, although there have been no RCT comparing different initial doses of GC. We recommend continuing 1 mg/kg/day for a maximum of 1 month with a subsequent gradual taper, which should be adjusted according to the patient’s clinical course. Examples of GC taper regimens are given in Online Appendix 3 (available at jrheum.org). In life-threatening disease and/or in patients with major organ involvement where rapid onset of action is needed, oral GC may be preceded by pulsed IV methylprednisolone 0.5–1 g/day for 3 consecutive days.
Evidence 2A, Strength of recommendation B
Barriers to implementation: None.
Previous guidance: BSR8, 2014 BSR21, EULAR/EUVAS6
Recommendation 6. Prophylaxis against Pneumocystis jirovecii infection should be given to patients receiving CYC or RTX. This prophylaxis consists, in the absence of allergy, of trimethoprim/sulfamethoxazole compounds (800/160 mg 1 tablet 3 times per week or 400/80 mg daily).
While there are no RCT evaluating the benefit of P. jirovecii infection prophylaxis in the patients with AAV treated with CYC, there are numerous reports of this infection in patients with AAV treated with GC and CYC58,59 or RTX60, and several studies that assessed the effectiveness of P. jirovecii pneumonia (PJP) prophylaxis among non-human immunodeficiency virus immunocompromised patients61. There are also several case reports of PJP occurring in patients several months after withdrawal of induction immunosuppression and we therefore suggest PJP prophylaxis be continued for at least 3 months after cessation of CYC60,62. The optimal duration of PJP prophylaxis after RTX-based induction when no reinfusion is planned is unknown. There is no consensus for PJP prophylaxis in patients receiving high-dose GC alone.
It should be noted that trimethoprim/sulfamethoxazole compounds used at these low doses for PJP prophylaxis are usually safe in combination with methotrexate (MTX), but not when used at higher therapeutic doses (i.e., 800/160 mg twice daily). Patients in whom trimethoprim/sulfamethoxazole compounds are contraindicated (e.g., because of sulfa allergies) should be given alternate prophylaxis with dapsone (100 mg daily) or atovaquone (1500 mg daily). Dapsone is often the most practical alternative to trimethoprim/sulfamethoxazole compounds in Canada, but prescribers must be aware of its potential complications, in particular the risk of hemolytic anemia, even in the absence of glucose-6-phosphate dehydrogenase deficiency. Aerosolized pentamidine (300 mg given monthly through a nebulizer) may not be as effective as trimethoprim/sulfamethoxazole for PJP prophylaxis63.
Evidence 3, Strength of recommendation C
Barriers to implementation: Atovaquone use is restricted in Canada owing to its high cost.
Previous guidance: 2014 BSR21, EULAR/EUVAS6, 2011 FVSG20, JCS10
Recommendation 7. There is insufficient evidence to support a recommendation that plasma exchange be used as first-line therapy in any patients with AAV. Plasma exchange may be a reasonable adjuvant therapy for patients who clinically deteriorate because of active vasculitis despite ongoing remission induction therapy with high-dose GC and CYC or RTX.
There is controversy around the efficacy of adjuvant plasma exchange in patients with AAV. Small RCT report conflicting evidence of improved renal survival and mortality64,65,66. The largest trial to date, the MEPEX trial (High-Dosage Methylprednisolone or Plasma Exchange as Adjunctive Therapy for Severe Renal Vasculitis), provides insufficient evidence of any sustained benefit, was limited to very ill patients nearing or requiring dialysis [with a serum creatinine 500 μmol/l (5.8 mg/dl)], and did not directly address the issue of plasma exchange as an adjuvant because MEPEX compared plasma exchange with pulse steroids67. Further, a contemporary metaanalysis demonstrated that even with MEPEX added to all other randomized trial results, it contained insufficient evidence to support a definite treatment effect of plasma exchange in AAV. Uncontrolled, retrospective data suggest a role in severe pulmonary hemorrhage, but are unconvincing66,67,68,69. The PEXIVAS study (plasma exchange and glucocorticoid dosing in the treatment of antineutrophil cytoplasm antibody associated vasculitis) is an international study with participating centers throughout Europe, the United States, Canada, Mexico, Japan, Australia, and New Zealand70, and addresses the safety and efficacy of plasma exchange as an adjuvant to GC and standard remission induction immunosuppression in patients with renal disease or pulmonary hemorrhage. Until the final results of the study are known (likely in 2017), patients with either renal manifestations of AAV resulting in a reduced glomerular filtration rate (GFR) or those with pulmonary hemorrhage may be referred to centers participating in PEXIVAS. In centers where this is not feasible, the use of plasma exchange can be restricted to patients who have refractory disease activity despite standard remission induction therapy with high-dose GC combined with CYC or RTX. We do not recommend that plasma exchange be used as an alternative to pulsed methylprednisolone as previously investigated in the MEPEX trial64. Plasma exchange may increase the risk of infections and bleeding, and physicians should be aware of these possible complications of therapy. If plasma exchange is used, we recommend 7 plasma exchanges (of 60 ml/kg or 1 plasma volume exchange) within 14 days using albumin as the replacement fluid, except in patients bleeding or with a high risk of bleeding (e.g., after renal biopsy). For such patients, consideration should be made to using either a full or partial exchange with fresh frozen plasma (e.g., with full fresh frozen plasma replacements in patients with pulmonary hemorrhage and until acute bleeding stops, gradually replaced thereafter by albumin only with 50% fresh frozen plasma and 50% albumin replacements the day and the following day of a renal biopsy) or monitoring and replacement of fibrinogen with cryoprecipitate.
Evidence 4, Strength of recommendation D
Barriers to implementation: Limitations in access to centers at which plasma exchange treatment is available.
Previous guidance: BSR8, 2014 BSR21, CARI9,11, Cochrane Review of Renal Vasculitis22, EULAR/EUVAS6, JCS10, KDIGO13
4.2 Remission induction for limited or nonsevere (nonorgan- and nonlife-threatening) newly diagnosed disease
Recommendation 8. In patients with limited and/or nonsevere GPA that is nonlife-threatening and without any major organ involvement, remission induction regimen with MTX in combination with GC can be used.
In patients with nonsevere (“limited”) GPA, MTX (20–25 mg per week, orally or subcutaneously, adjusted to renal function; Online Appendix 3, available at jrheum.org) can be used as an alternative to CYC, in combination with GC, and continued for longer than 12 months if effective. Few studies have found that MTX is noninferior to CYC at inducing remission in these patients71,72, although the time to remission may be longer with MTX if started initially at a lower starting dose of 15 mg per week [NORAM (nonrenal Wegener’s Granulomatosis Treated Alternatively with Methotrexate), with a gradual increase of the dose up to 20–25 mg per week at Month 3]73. The longterm followup data of the NORAM study suggest also that there is a higher rate of relapse in patients following MTX-based induction if it is stopped after 12 months74.
The use of mycophenolate mofetil (MMF) as an alternative to CYC in nonsevere GPA was investigated in a trial [MYCYC (mycophenolate mofetil versus cyclophosphamide for remission induction of ANCA-associated vasculitis); ClinicalTrials.gov Identifier: NCT00414128]. Preliminary results suggest a similar rate of remission, but a higher rate of subsequent relapse as well75. The data remain limited on the use of trimethoprim/sulfamethoxazole, alone or with GC, for very limited GPA without any major organ involvement and can therefore not support a recommendation that it be used as an alternative to CYC or MTX76.
Evidence 1B, Strength of recommendation A
Barriers to implementation: None.
Previous guidance: BSR8, 2014 BSR21, CARI9,11, EULAR/EUVAS6
Recommendation 9. Patients with nonsevere EGPA or nonsevere MPA without renal involvement can be treated with GC alone for remission induction. At present, there is no consensus on the use of any immunosuppressant agents in combination with GC in patients with EGPA or MPA that are nonsevere (including those with mononeuritis multiplex).
Patients with EGPA and MPA with nonsevere disease (FFS of 0 and no renal disease) have a 5-year mortality rate of 11.9%41, and so this subset of patients may not require an additional immunosuppressant agent to induce remission. A study of patients with MPA, EGPA, and PAN found that GC alone induced remission in almost 80% of patients, although this remission was sustained in less than 50% of patients77,78. It is acceptable to treat patients with nonsevere, nonlife-threatening disease without renal disease or any other major organ involvement with GC alone, introducing additional immunosuppressant therapy for relapsing, deteriorating, or GC-resistant disease. Close monitoring of patients treated with GC alone is mandatory to detect any such early deterioration of their condition and promptly add an immunosuppressant as needed.
The optimum treatment strategy in patients with nonsevere disease but peripheral nervous system (PNS) involvement remains a subject of debate. There is insufficient evidence to support a recommendation that the systematic prescription of an immunosuppressant, in combination with GC, as first-line therapy is more effective then GC alone on the neurologic recovery. Nevertheless, PNS involvement, particularly mononeuritis multiplex, can be severe and/or rapidly progressive, with a risk of significant longterm disability; in such cases, a more aggressive treatment with additional immunosuppressant therapy [e.g., with azathioprine (AZA), MTX, or in the most severe and progressive cases, CYC] must be considered79. The results of the FVSG CHUSPAN2 trial [New Treatment Strategy for Patients With Microscopic Polyangiitis, Polyarteritis nodosa (PAN) or eosinophilic granulomatosis with polyangiitis (CHUrg Strauss syndrome) Churg Strauss Syndrome Without Poor Prognosis Factors-trial 2; expected in late 2015], which looked at the treatment of patients with EGPA, MPA, and PAN with an FFS of 0 (including some patients with PNS involvement) with GC alone or GC with AZA, may provide further insight into the treatment of this subgroup of patients.
Evidence 2B, Strength of recommendation C
Barriers to implementation: None.
Previous guidance: General comments in the 2007 FVSG12.
5. Remission maintenance therapy
Remission is defined by EULAR/EUVAS as the complete absence of clinical disease activity, including vasculitis and granulomatous manifestations whether receiving immunosuppressive therapy or not39 (Appendix 1).
Recommendation 10. In patients with severe AAV in remission after a combined CYC-GC–based induction treatment, maintenance therapy can be based on AZA or MTX, initially in combination with low-dose GC. Leflunomide (LEF) or MMF may be alternative agents in patients not tolerating or with contraindications to AZA and MTX.
Longterm toxicity makes CYC an unattractive option for maintenance of remission after successful remission induction in AAV. Following remission induction therapy with CYC, the CYCAZAREM trial (cyclophosphamide vs azathioprine for early remission phase of vasculitis) found that AZA (2 mg/kg/day) was as effective as continuous CYC at maintaining remission and was associated with fewer side effects54. MTX (20–25 mg/week) was proven to be of comparable efficacy to AZA after remission induction with CYC55,80. MTX should be used with caution in patients with renal impairment. The use of LEF in maintaining remission is less well studied, but results of 1 prematurely ended randomized study indicated that, at a dose of 30 mg/day, LEF was more effective than MTX at preventing relapse despite being associated with a higher rate of adverse events81. At present, in parallel with practice in RA, a dose of 20 mg/day can be used and is likely associated with a lower frequency of side effects82. MMF (2–3 g/day) has been studied in this setting, but has been found in 1 randomized controlled study to be less effective than AZA at maintaining remission and should therefore not be used as a first-line agent for maintenance57.
Evidence 1B, Strength of recommendation B
Barriers to implementation: None.
Previous guidance: BSR8, 2014 BSR21, CARI9,11, EULAR/EUVAS6, JCS10, KDIGO13
Recommendation 11. In patients with severe AAV in remission after a combined CYC-GC–based induction treatment, maintenance therapy with RTX infusions is an alternative to AZA, especially for those patients with PR3-ANCA–positive GPA.
Results of several retrospective studies on the preemptive use of RTX for maintenance following induction with RTX or CYC in combination with GC in patients with GPA or MPA have suggested that it is safe and effective53,83,84,85. The results of these studies indicate that it may even be superior to AZA or MTX in preventing relapses84,85. The results of the FVSG MAINRITSAN trial (Maintenance of Remission using Rituximab in Systemic ANCA-associated Vasculitis) showed that RTX 500 mg at remission, 2 weeks later, and then every 6 months up to Month 18, is superior to AZA in preventing relapses (relapse rates of 5.3% vs 29.3% at 28 mos postremission, respectively), with a comparable safety profile86. Because the patients in the FVSG MAINRITSAN study were predominantly patients with PR3-ANCA–positive GPA, the findings could not be generalized to all patients with AAV. The role of RTX in patients with MPA or MPO-ANCA–positive GPA, or who are ANCA-negative, has to be further studied. The optimal duration, dose, and interval between each RTX infusion have to be further investigated. Whether the monitoring of CD19 B cell count, ANCA titer, or other biological variables may guide the need for RTX reinfusion is also under study (MAINRITSAN 2; ClinicalTrials.gov Identifier: NCT01731561)53.
Evidence 1B, Strength of recommendation A
Barriers to implementation: RTX maintenance funding is not yet approved by Health Canada.
Previous guidance: 2014 BSR21, 2011 FVSG20
Statement 6. To date, there is no definitive evidence to guide decisions for maintenance therapy after remission induction with RTX.
At least theoretically, 4 possible strategies for maintenance therapy after RTX induction exist: (1) patients, at least those with PR3-ANCA–positive GPA, may be retreated with RTX at regular intervals, similarly to what can be done after CYC-based induction therapy87; (2) patients may be retreated with RTX in response to laboratory variables, i.e., repopulation of peripheral CD19 B cell counts or rising ANCA titers53; (3) patients may be retreated with RTX (or another remission-inducing agent) only on the grounds of clinical relapse88,89; and (4) patients may be maintained on conventional maintenance immunosuppressant drugs such as AZA, MTX, MMF, or LEF83,90. It is not yet known which of these strategies is optimal. The RITAZAREM trial [rituximab (RTX) or azathioprine (AZA) for remission after RTX induction; ClinicalTrials.gov Identifier: NCT01697267; results expected in 2018] is comparing AZA versus RTX (1 g every 4 mos for 20 mos) for maintenance in patients with relapsing ANCA-associated GPA or MPA who achieve remission with RTX (4 × 375 mg/m2).
Barriers to implementation: RTX maintenance funding is not yet approved by Health Canada.
Previous guidance: Guerry, et al7, 2014 BSR21
Statement 7. Low-dose GC should be part of the initial remission maintenance therapy after remission is achieved; there is not enough evidence yet to support further recommendation on the optimal duration of low-dose GC.
GC should be gradually tapered to a dose of 5–10 mg/day within 3 to 6 months of achieving remission (see Online Appendix 3 for examples of GC regimens used in RCT, available at jrheum.org). No RCT have yet assessed the optimum duration of GC in remission maintenance. One large metaanalysis looked at previous AAV studies that incorporated GC into their treatment protocols. Relapse rates were higher in patients who discontinued GC within 12 months of achieving remission91. Results of another single-center study from Chapel Hill have indicated that longterm PRED treatment even at a low dose does not limit the risk of relapse, but can increase the risk of infections92. The VCRC TAPIR study [Vasculitis Clinical Research Consortium — The Assessment of Prednisone In Remission Trial; ClinicalTrials.gov Identifier: NCT01940094] aims at evaluating the effects of continuing low-dose PRED as compared with stopping PRED treatment entirely in patients with GPA in remission after a disease flare that occurred within the past 12 months (results expected in late 2016).
Barriers to implementation: None.
Previous guidance: 2014 BSR21, EULAR/EUVAS6
Recommendation 12. We recommend the use of AZA, MTX, or their alternatives (as per Recommendations 10 and 11) for remission maintenance therapy to be continued for a minimum of 18 months after successful remission induction. There is not yet enough evidence to support further recommendation on the optimal duration of their use for maintenance.
To date, the optimum duration of maintenance immunosuppressant therapy is not known. There are retrospective studies suggesting that relapse rates are lower in patients continuing on maintenance therapy beyond 36 months93. The REMAIN study (REmission MAINtenance therapy in AAV) is a EUVAS RCT that has randomized patients, after successful remission induction therapy, to receive 24 months of low-dose GC and AZA or 48 months low-dose GC and AZA (results expected in 2015). In the future, there may be data to support tailoring the duration of maintenance therapy according to clinical and biological predictors of relapse, such as the presence of PR3 versus MPO ANCA, but at present, work is ongoing in this field and no firm conclusions have been reached that can affect practice94,95,96. Until these results are available, we recommend that maintenance therapy be continued for at least 18 months after successful remission induction, then subsequently discontinued or not at the physician’s discretion and according to the individual patient’s characteristics, treatment tolerance, and understanding of their subsequent risk of relapse.
Evidence 3, Strength of recommendation C
Barriers to implementation: None.
Previous guidance: BSR8, 2014 BSR21, EULAR/EUVAS6, KDIGO13, 2011 FVSG20
Recommendation 13. The use of trimethoprim/sulfamethoxazole (800/160 mg twice daily) as remission maintenance therapy can be considered in GPA as an adjuvant to immunosuppressant or after the cessation of maintenance immunosuppressive treatment.
The use of full-dose trimethoprim/sulfamethoxazole (800/160 mg twice daily) as remission maintenance monotherapy has been associated with a higher overall relapse rate than that observed with conventional remission maintenance agents97,98. Full-dose trimethoprim/sulfamethoxazole has demonstrated efficacy at preventing upper airway/ENT disease relapse76,99, but has no proven benefit at reducing any other form of disease relapse. It should only be used as an adjunct agent or after completion of the maintenance immunosuppressive therapy. It should not be used as remission maintenance monotherapy. Because of important drug interactions, it should not be used at this high dose in conjunction with MTX, but is safe as an adjunct with AZA and LEF.
Evidence 3, Strength of recommendation C
Barriers to implementation: None.
Previous guidance: BSR8, CARI9,11, EULAR/EUVAS6, KDIGO13
Recommendation 14. Topical therapies may be considered, in combination with the systemic therapy and in collaboration with ENT subspecialists, to alleviate the symptoms of upper airway and ENT disease.
The consequences of upper airway and ENT disease often continue to manifest (as damage) despite achieving successful disease remission. It should be noted that such persistent upper airway symptoms, such as nasal crusting or congestion, and symptoms due to stenosis of nasal passage or upper airway are thus not always attributable to active granulomatous disease and therefore do not necessarily require additional immunosuppressant therapy. Therapies aimed at managing these symptoms are often essential for patient well-being. Nasal and sinus rinses with saline may be helpful. Topical antibiotic creams and ointments, such as mupirocin or fusidic acid, can also be considered, but are usually of limited benefit. There are no clinical trial data to support their use for patients with symptomatic nasal crusting and ulcers, including those with chronic nasal carriage of Staphylococcus aureus. These local therapies have not been shown to lower the risk of relapse or progression from a limited ENT to a more systemic form of the disease in patients with GPA.
Evidence 3, Strength of recommendation C
Barriers to implementation: There is a shortage of ENT subspecialists trained in the assessment and management of patients with AAV in Canada.
6. Relapsing disease
Relapsing disease is defined by EULAR/EUVAS as the reoccurrence or new onset of disease activity attributable to active vasculitis-related inflammation (Appendix 1)39. It is useful to define the severity of disease at the time of relapse to guide treatment decisions. It must be recognized, however, that no classification criteria or scoring systems (including the FFS or BVAS) have been validated in the context of relapsing disease as opposed to newly diagnosed disease. In the context of clinical trials, EULAR/EUVAS suggest that relapses should be recorded as either minor or major. A major relapse is defined as the reoccurrence or new onset of potentially organ- or life-threatening disease activity that cannot be treated with an increase of GC alone and requires further escalation of treatment. All other relapses should be classified as minor. This classification strategy has not been validated, but may prove to be a useful tool in the setting of relapsing disease. In RAVE, severe GPA or MPA flares or relapses were defined as with a BVAS/WG score of 3 or more (≥ 3 minor items or 1 major item)40.
Recommendation 15. We recommend remission induction of a major organ- or life-threatening relapse with either CYC or RTX in conjunction with high-dose GC. In patients who already received CYC for initial remission induction or a previous disease flare, we recommend using RTX for remission reinduction.
The RAVE study showed that RTX was more effective at Month 6 than CYC for remission induction in relapsing disease (67% vs 42% of relapsing patients achieved remission with RTX vs CYC, respectively)40. At 18 months, without any maintenance therapy after RTX-based induction, this difference with the conventional staged CYC-AZA treatment persisted, though it was no longer a significant difference88. We therefore recommend using RTX for remission reinduction in patients previously treated with CYC (irrespective of the cumulative dose previously received), those in whom CYC is contraindicated or in whom CYC was previously ineffective or not tolerated, and for patients wishing to preserve fertility (see Online Appendix 3 for RTX prescribing, available at jrheum.org). For the patients in whom RTX is contraindicated or who fail to respond to RTX, given at appropriate doses, retreatment with CYC can still be considered (in the absence of a clear contraindication, such as severe allergy). Such patients presenting with complex refractory disease may especially benefit from the direct input of a referral center for vasculitis (Statement 4).
Evidence 1B, Strength of recommendation A
Barriers to implementation: Current funding approval in Canadian provinces (Online Appendix 6, available at jrheum.org) for the use of RTX for remission induction is for patients with newly diagnosed or relapsing disease only in the context of a contraindication to CYC, including the previous administration of > 25 g of cumulative dose of CYC.
Previous guidance: BSR8, 2014 BSR21, EULAR/EUVAS6, 2011 FVSG20, KDIGO13
Recommendation 16. There is insufficient evidence to support a recommendation that plasma exchange be used as first-line therapy in all patients with relapsing AAV with severe renal (GFR < 50 ml/min) or pulmonary hemorrhage. Plasma exchange may be a reasonable adjuvant therapy for patients who clinically deteriorate because of active relapsing vasculitis despite ongoing remission induction therapy with high-dose GC and CYC or RTX.
See Recommendation 7 for more details on plasma exchange.
Evidence 4, Strength of recommendation D
Barriers to implementation: Limitations in access to centers at which plasma exchange treatment is available.
Previous guidance: BSR8, 2014 BSR21
Recommendation 17. We recommend that relapses that are nonsevere, i.e., nonlife– and nonorgan-threatening, be treated with an increase in GC dose in addition to optimizing the patient’s concurrent immunosuppressant agent.
The treatment of nonlife- and nonorgan-threatening disease relapses should include increasing the GC dose and optimizing the patient’s concurrent immunosuppressant agent. There is no evidence to suggest superiority of MTX over AZA, and data on LEF, MMF, abatacept, or RTX is very limited in this setting and mostly related to GPA100,101. Further, it is not known whether patients with disease relapse after cessation of maintenance therapy should be treated with a more prolonged course of maintenance immunosuppressant therapy following their relapse. We therefore cannot make further or specific recommendations regarding the choice or change of immunosuppressant agent and the duration of therapy following a nonmajor disease relapse.
Evidence 3, Strength of recommendation C
Barriers to implementation: None.
7. Refractory disease
The term “refractory disease” applies to patients who fail to attain remission following “standard” induction therapy, which is tailored according to the severity and extent of disease. The precise timing of when disease should be labeled as refractory is less clear. EULAR/EUVAS propose that refractory disease is defined as (1) unchanged or increased disease activity after 4 weeks of appropriate-dose CYC with GC, (2) lack of response defined as ≤ 50% reduction in the Disease Activity Score and/or lack of improvement in at least 1 major item after 4–6 weeks of treatment, or (3) chronic persistent disease defined as the presence of at least 1 major or 3 minor items on the BVAS list despite 8 weeks of treatment39. These EULAR/EUVAS definitions of refractory disease are complex and difficult to apply in everyday clinical practice. We therefore propose a simplified version: refractory disease being disease that is unchanged or worsened despite 6 weeks of appropriate remission induction therapy or the presence of persistent disease activity after 3 months of appropriate remission induction therapy.
Consideration should be given to the referral of patients with refractory disease to a center for vasculitis. In all cases of apparent refractory disease, it is imperative to reevaluate the patient to ensure the following: (1) the diagnosis is correct, (2) alternate infectious/neoplastic diagnoses have been excluded, and (3) the treatment, including choice of drug(s), dosage, and duration, was appropriate.
Having considered the above and confirmed a patient has refractory disease, the following recommendations should be taken into account for the ongoing management of this challenging patient group.
Recommendation 18. We recommend the use of RTX in combination with GC in patients with severe GPA or MPA who fail to respond to CYC as remission induction therapy.
The RITUXVAS50 and RAVE40 trials demonstrated that RTX is noninferior to CYC at inducing remission in patients with severe or life-threatening manifestations of AAV. Several retrospective series have reported the efficacy of RTX in patients with refractory disease51,53. We recommend that patients who have an inadequate response to either 6 infusions of an appropriate dose of IV CYC (Online Appendix 3, available at jrheum.org) or 3 months of oral CYC be treated with RTX (see Online Appendix 3 for RTX prescribing advice, available at jrheum.org).
Evidence 3, Strength of recommendation C
Barriers to implementation: RTX is approved in Canada for these patients, but access may be limited by the delay in obtaining timely approval for the drug coverage, which can vary according to the province.
Previous guidance: BSR8, 2014 BSR21, EULAR/EUVAS6, 2011 FVSG20, Guerry, et al7, KDIGO13
Statement 8. Patients with refractory disease should be managed in a referral center for vasculitis in collaboration with subspecialists with experience in managing such patients.
Because of the rarity of these diseases, it can be difficult for all physicians to achieve and maintain skills in managing patients with refractory disease. We therefore suggest that these patients be referred to a center for vasculitis. These patients usually also require the input of different sub-specialists who work regularly in close collaboration with referral centers for vasculitis. Granulomatous head and neck manifestations of GPA, such as subglottic stenosis and retro-orbital pseudo tumors, are examples of disease manifestations that are frequently resistant to systemic treatments and may require other specific treatments to improve symptoms and quality of life102,103,104,105,106.
Barriers to implementation: There is a shortage of healthcare providers trained in the assessment and management of patients with AAV in Canada. The creation of CanVasc and the identification of CanVasc centers and collaborators across Canada (Online Appendix 8, available at jrheum.org) aimed to decrease the lag between identification and referral of patients with AAV.
Previous guidance: 2014 BSR21
Statement 9. Patients with EGPA and persistent asthmatic symptoms, despite remission of their vasculitic manifestations, should be managed in collaboration with a physician subspecializing in asthma management.
Patients with a diagnosis of EGPA may have resurgence of their asthma symptoms while taking maintenance immunosuppressant therapies or after discontinuing such therapies107. If the vasculitic manifestations of the disease are in remission, we do not recommend that worsening asthmatic symptoms be regarded as refractory disease. Although the escalation or reintroduction of immunosuppressant therapy is not necessarily warranted, it (including AZA, MTX, LEF, or MMF) may be considered as a way to avoid taking or limit the use of GC. There is very little evidence looking at the optimal management of these patients. Followup with an asthma specialist to ensure adherence with asthma management guidelines should be systematically considered. Referral of patients to a referral center for vasculitis for further assessment should also be considered because therapeutic trials may exist for these patients.
Barriers to implementation: There is a shortage of physicians subspecializing in asthma management and trained in the assessment and management of patients with AAV in Canada. The creation of CanVasc and the identification of CanVasc centers and collaborators across Canada (Online Appendix 8, available at jrheum.org) aimed to decrease the lag between identification and referral of patients with AAV.
Previous guidance: No specific guidelines.
8. Additional and experimental therapies
Statement 10. In patients in whom the aforementioned therapies are ineffective, contraindicated, or poorly tolerated, consideration can be given to alternate, additional, and/or experimental therapies in collaboration with a referral center for vasculitis.
IV immunoglobulin (IVIG). A few series and open-label studies suggested that IVIG can help achieve remission, in combination with GC, in patients with refractory disease (in addition to immunosuppressants) and/or in those with contraindication to immunosuppressants108,109. There has been only 1 RCT studying the use of IVIG therapy in AAV. Patients with active AAV despite immunosuppressant therapy were randomized to receive IVIG or placebo in addition to “standard” therapy: 82% versus 35% of patients demonstrated a 50% reduction in disease activity in the IVIG versus placebo groups, respectively110. This difference was observed up to 3 months following therapy, but no differences were noted beyond this time. The benefit of IVIG does not appear to be sustained after the cessation of the infusions. On the basis of the limited evidence, IVIG (see Online Appendix 3 for IVIG prescribing advice, available at jrheum.org) is not a substitute for more conventional immunosuppressant therapies. IVIG could, however, be a useful therapy in certain patient subgroups: as an adjunct in those with refractory disease, in pregnant patients in whom alternate immunosuppressants are contraindicated, in patients with active vasculitis, and in those with a current severe infection or high recurrence rate of severe infections.
Evidence 3, Strength of recommendation C
Antitumor necrosis factor-α (anti-TNF-α) agents. The WGET studied 180 patients with GPA who received standard induction therapy with either CYC followed by maintenance with MTX or AZA (severe disease) or MTX for both induction and maintenance (limited disease), in combination with GC, and either etanercept (ETN) or placebo during induction and maintenance therapies38. At 27 months, only 50% of patients achieved a sustained remission, and there was no difference in sustained remission rates between the ETN and placebo groups. Further, there was a significantly higher rate of occurrence of solid tumors in both groups compared with the general population and in the ETN group compared with the placebo group during the study period. However, the latter difference between study groups was no longer significantly different during poststudy closure followup111. Data on other anti-TNF-α agents are limited with only retrospective and open-labeled studies, which showed possible efficacy in selected patients. One small controlled study112 of infliximab (IFX) versus RTX for refractory GPA showed that RTX was superior at inducing and maintaining remission during longterm followup113,114,115. We therefore recommend that ETN not be used in regular practice for the treatment of AAV. The use of other anti-TNF-α agents, such as IFX, should be limited to very specific cases of refractory disease when other alternative therapeutic options have failed or cannot be used, and they should not be given in combination with CYC.
Evidence 1B, Strength of recommendation A
Mepolizumab. A few series showed promising results for IV mepolizumab, a monoclonal antibody directed against interleukin 5 for patients with EGPA GC-dependent and/or refractory to other immunosuppressants116,117. The MIRRA trial (Mepolizumab Treatment In Relapsing or Refractory EGPA; ClinicalTrials.gov Identifier: NCT02020889) aims at studying subcutaneous mepolizumab for patients with EGPA who cannot taper PRED below 7.5 mg/day without the reappearance of disease manifestation(s).
Evidence 3, Strength of recommendation D
Anti-CD52 therapy. Alemtuzumab is a humanized monoclonal antibody to CD52 with antilymphocyte activity and has been shown in a case series to induce remission in AAV, although relapses and adverse events are common; its use in GPA is considered experimental118 and there is no approval for this drug for vasculitis in Canada.
Evidence 3, Strength of recommendation D
Barriers to implementation: There is a shortage of healthcare providers trained in the assessment and management of patients with AAV in Canada. The creation of CanVasc and the identification of CanVasc centers and collaborators across Canada (Online Appendix 8, available at jrheum.org) aimed to decrease the lag between identification and referral of patients with AAV. Access to the aforementioned therapies is not possible in every province and none of them is approved by Health Canada for AAV (access is restricted, with provincial formularies and/or the need to apply for provincial exceptional access program approval).
Previous guidance: BSR8, Cochrane Review of IVIG23, EULAR/EUVAS6, KDIGO13
9. Followup of patients with AAV
Statement 11. Patients with AAV should be followed regularly for many years with full clinical assessment and routine laboratory work to assess disease course and track for disease activity and disease- or treatment-related damage.
Patients receiving remission induction and maintenance therapy require regular clinical assessment to monitor their disease course, response to treatment, and the potential adverse effects of treatments. The frequency at which this is done depends on the individual patient, the characteristics and history of their disease, and the therapies required. We suggest that patients receiving remission induction therapy be seen on a monthly basis and those receiving maintenance therapy be seen on a 3-monthly basis for the first 2 years. The frequency of subsequent followup visits could be tailored to the individual patient in continued and close collaboration with the patient’s family physician and other subspecialists possibly involved. Given that relapses of AAV can occur at any stage, we recommend that all patients be reviewed longterm, at least annually, to monitor for signs of relapse, to assess for potential longterm toxicities of immunosuppressant therapies, and in some cases to manage the repercussions of vasculitis-induced damage. At each visit, irrespective of the disease state, we recommend patients undergo a full clinical assessment and routine laboratory work (see Online Appendix 1 for suggested blood tests at followup, available at jrheum.org).
There is currently no evidence to suggest that rising ANCA titers alone warrant therapeutic changes, and therefore the need for serial ANCA testing is debatable119,120,121. The value of monitoring CD19 B cell count in patients treated with RTX also remains to be determined because currently available data do not support that it is sensitive or specific enough to help predict relapses.
Barriers to implementation: There is a shortage of healthcare providers trained in the assessment and management of patients with AAV in Canada. The creation of CanVasc and the identification of CanVasc centers and collaborators across Canada (Online Appendix 8, available at jrheum.org) aimed to decrease the lag between identification and referral of patients with AAV.
Previous guidance: BSR8, 2014 BSR21, KDIGO13
Statement 12. All patients previously treated with CYC should have a urinalysis every 3–6 months as a lifelong means of screening for CYC-induced bladder toxicity. If micro- or macroscopic hematuria is present, in the absence of an alternate explanation, the patient should be referred for consideration of a cystoscopy.
It is widely recognized that the use of CYC is associated with bladder toxicity, namely hemorrhagic cystitis and bladder cancer49,122,123. The risks have lessened somewhat over recent years, perhaps because of the more frequent coprescription of mesna (at least for hemorrhagic cystitis) and the lower cumulative doses of CYC used in patients with AAV. Nevertheless, we suggest that all patients previously treated with CYC, especially those who received high total cumulative doses of CYC, have urine dipstick testing at least every 3–6 months as part of their regular followup (cumulative doses given to patients in whom bladder cancer developed varied widely, above 30 gm in almost all cases and above 100 gm in the majority of them). If hematuria is present, the quantification of hematuria and urine cytopathology may be helpful. In the absence of an alternate explanation, such as infection, active renal disease, or renal damage of AAV, screening cystoscopy may be indicated and the patient should be referred for cystoscopy.
Barriers to implementation: None.
Previous guidance: BSR8, 2014 BSR21
Statement 13. As part of their lifelong annual followup, cardiovascular (CV) risk factors [including smoking status, diabetes, hypercholesterolemia, hypertension (HTN), and obesity] and risk for osteoporosis should be systematically assessed, with treatment as needed according to the current respective guidelines for each of these conditions.
There is good evidence that chronic inflammatory disorders such as RA or systemic lupus erythematosus are associated with an increased risk of longterm CV events124,125. Publications in GPA and MPA describe a rate of CV events around 10% over a median 4.3-year followup period48,126. The longterm use of GC increases the risk of osteoporosis. The presence of renal impairment in patients with AAV adds a level of complexity in the therapeutic decisions for the prevention of osteoporosis.
As part of their longterm annual followup, patients with AAV should thus also be assessed, in collaboration with their primary care provider and/or subspecialist comanaging them, for osteoporosis and CV risk factors, including smoking status, diabetes, hypercholesterolemia, HTN, and obesity, and be appropriately counseled and treated, irrespective of the state of their vasculitis. There is not enough evidence at present to recommend a standardized list of investigations to perform in all patients or an optimal frequency, other than annual CV (risk) assessment. The prevention of osteoporosis should rely on the last updated and available Canadian guidelines (available at www.osteoporosis.ca)127,128,129.
Barriers to implementation: Collaborations with patient’s family physician and other healthcare providers specialized in the prevention and management of CV risk factors or osteoporosis must be encouraged to optimize this mandatory longterm followup.
10. Special patient groups
Statement 14. Women with AAV should not consider pregnancy earlier than 6 months after sustained remission of their disease has been achieved. Women with AAV planning pregnancy and those pregnant should be managed in close collaboration with an obstetrician with expertise in this field and/or in high-risk pregnancies.
In the past, the high morbidity associated with AAV and the toxic feature of the available treatments meant that pregnancy was unusual in this patient group. Thus, there are limited data available on pregnancy, its management, and outcomes in women with AAV. Retrospective reports suggest that while significant worsening of the patient’s vasculitis is unusual during pregnancy, there are reports of pregnancy complications related to previous vasculitis-induced damage, such as cardiac decompensation, or problems related to chronic impairment of renal function. There may also be a higher rate of first trimester miscarriage, preterm labor, and the need for Cesarean section deliveries in these patients130,131,132. Therefore, we suggest that these patients be seen before conception and monitored closely throughout pregnancy in close collaboration with the obstetric team. Published case series suggest that worsening vasculitis is less likely to occur in patients in sustained remission at the time of conception. Patients should therefore probably wait for at least 6 months after achieving sustained remission before attempting to conceive130,131,133,134, and those stable on maintenance immunosuppression should be receiving pregnancy-safe options (i.e., AZA but not MTX, MMF, LEF, or any other teratogenic drugs). In view of the known teratogenicity of some of the drugs used in the management of AAV, including CYC, MTX, LEF, and MMF, it is imperative to advise patients to take appropriate contraceptive measures when treated with those immunosuppressants.
Barriers to implementation: There is a shortage of physicians subspecializing in high-risk pregnancies and trained in the assessment and management of patients with AAV in Canada. The creation of CanVasc and the identification of CanVasc centers and collaborators across Canada (Online Appendix 8, available at jrheum.org) aimed to decrease the lag between identification and referral of patients with AAV.
Previous guidance: None specifically.
Statement 15. There are no pediatric-specific management guidelines for pediatric AAV yet, and most knowledge in pediatric AAV is adapted from adult research. Management of children with AAV should be provided by pediatric physicians at an academic healthcare center in collaboration with referral centers for vasculitis and/or centers with special interest in pediatric vasculitis.
Because of the rarity of pediatric AAV, there have been no studies from which to develop pediatric-specific guidelines, and most knowledge has been adapted from adult literature and experience. For the same reason, few pediatricians have experience in diagnosing and managing children with AAV. Notwithstanding, children should be managed at a pediatric academic healthcare center by pediatric physicians who have an understanding of the potential effects of disease and treatments on growth and development. If necessary, there should be close collaboration with centers having a special interest in pediatric vasculitis. All patients should be invited to participate in national or international registries of childhood vasculitis with a view to improving pediatric-specific knowledge and care.
Barriers to implementation: There is a shortage of pediatric physicians subspecializing and/or trained in the assessment and management of patients with AAV in Canada. The creation of CanVasc and the identification of CanVasc centers and collaborators across Canada (Online Appendix 8, available at jrheum.org) aimed to decrease the lag between identification and referral of patients with AAV. Several pediatric referral centers for vasculitis are participating in the CanVasc research network.
Previous guidance: None.
Statement 16. AAV in children should be classified at the time of diagnosis based on the childhood EULAR/Paediatric Rheumatology International Trial Organization (PRINTO)/Paediatric Rheumatology European Society (PReS) criteria so that therapy can be tailored accordingly.
GPA is the most common of these rare childhood AAV, followed by MPA, and EGPA is extremely rare. A pediatric adaptation of the ACR criteria taking into account common pediatric manifestations and the presence of ANCA has enabled a specific classification for pediatric GPA, validated using a cohort of pediatric patients — EULAR/PRINTO/PReS criteria135,136,137. Systematic use of pediatric classification and adopting adult systems for “disease severity classification” will provide a framework for tailoring therapy (see Statement 3) and will provide the cornerstone for subsequent development of pediatric-specific management guidelines.
Barriers to implementation: None.
Previous guidance: None.
Statement 17. Children with newly diagnosed AAV should be treated according to adult recommendations for induction of remission and then maintenance, with medication dose adjusted for this specific population.
Induction treatment for children with severe GPA or MPA should rely on a combination of high-dose GC plus either CYC or RTX. The dose of CYC must be adjusted in children with renal impairment and therapy should be monitored according to adult recommendations. Consideration should be given to RTX as first-line remission induction therapy in children with severe GPA or MPA in whom CYC is contraindicated or in whom CYC presents an unacceptable risk of infertility. An international open-label study is ongoing to assess the involvement of RTX in children with severe GPA or MPA (ClinicalTrials.gov Identifier: NCT01750697; results expected in mid-2017).
Plasma exchange should be considered in children with rapidly progressive, severe renal disease or severe pulmonary hemorrhage despite induction therapy with GC and CYC or RTX. In children with limited nonsevere disease, induction therapy regimen with MTX in combination with GC may be considered.
As in adults, prophylaxis against P. jirovecii infection should be given to children receiving CYC or RTX.
Remission induction therapy with CYC should be switched to maintenance treatment within 3–6 months. Maintenance treatment after remission induction through GC and CYC is based on adult recommendations of a combination of low-dose GC plus AZA or MTX for a minimum of 24 months. There is no evidence to guide decisions regarding the duration of GC therapy.
Barriers to implementation: In Canada, RTX is approved for induction therapy in adults with severe ANCA-positive GPA or MPA, but is not yet approved for children.
Previous guidance: None.
Recommendation 19. In children, severe relapsing AAV or severe AAV refractory to the combination of CYC and GC (with major organ involvement or life-threatening manifestations) should be treated with RTX in combination with GC.
Because AAV are relapsing conditions and a previous relapse is a risk factor for another and subsequent one95, limiting the exposure to CYC in children is crucial. Children may experience multiple flares during their lifetime and repeated or sustained exposure to CYC can induce infertility, bladder cancer, or lymphoma138,139. The use of RTX in combination with GC as first-line treatment for disease relapses should therefore be considered in children, especially if they have already received CYC, independent of their cumulative dose. However, it must be remembered that data on the longterm safety of RTX in children in AAV are lacking.
Evidence 4, Strength of recommendation D
Barriers to implementation: In Canada, RTX is approved for induction therapy in adults with severe ANCA-positive GPA or MPA, but is not yet approved for children.
Previous guidance: None.
DISCUSSION
Seventeen statements and 19 recommendations were developed by the CanVasc working group. These were based on a synthesis and reappraisal of international guidelines on AAV, supporting evidence from observational studies and RCT, and consensus from healthcare professionals from different medical specialties, taking into account the present Canadian healthcare specificities. We anticipate that this document and practical appendices (Appendix 1; other appendices available online at jrheum.org as supplementary data) will serve as useful knowledge to support decision making for any physician involved in the care of patients with AAV, including adults and children. Best clinical judgment must, however, always prevail when confronted with each specific patient.
The guidelines were developed following an adaptation of the process previously used for the CRA-endorsed recommendations for the management of RA and with guidance from the CRA therapeutic committee16,17,18. Along with the needs assessment questionnaire, the existence of earlier published international guidelines helped the working group to delineate the set of recommendations and statements addressed in this document. Supporting evidence from observational studies and RCT linked to each recommendation were reviewed and graded. However, as for many sets of guidelines and recommendations, it appears that strong evidence is lacking for many of the addressed points. We opted to list those nontherapeutic points as statements without grading them to simply reflect that these represent working group consensus.
Limitations include the fact that a systematic review of original literature prior to 2010 was not performed. It had already been completed by other groups, including the EUVAS/EULAR group when devising their recommendations6,140. We therefore indirectly incorporated the earlier literature by reviewing other existing guidelines in our process. Second, although more up-to-date than those previously published recommendations or guidelines on AAV, basic, clinical, and therapeutic research in the field of AAV is currently progressing at a fast pace. Therefore, new information from ongoing research may already have become available by the time the present document is published. Regular updates will thus be mandatory. It is our hope that this document will support decision making by healthcare professionals, promote and harmonize best practices throughout Canada, and ultimately improve patient outcomes.
ONLINE SUPPLEMENT
Supplementary data for this article are available online at jrheum.org.
Acknowledgment
The following persons also participated in the development of these recommendations (reviewers): Drs. Corisande Baldwin, Maria Bagovich, Claire Barber, Joanne Bargman, David Barth, Sankalp Bhavsar, Ken Blocka, Gilles Boire, M. Boussier, Robert Ferrari, Michele Hladunewich, Susan Huang, Jacob Karsh, Kim Legaut, Emil Nashi, Maxime Rhéaume, Nathalie Roy, Evelyn Sutton, Yves Troyanov, and Pearce G. Wilcox; and for the Vasculitis Foundation Canada: John Stewart, Katherine Smith, and Barbara Tuntoglu (administrative board). The working group also thanks Sandra Messier, who provided administrative coordination support during all steps of the development of these recommendations, and Dr. Shahin Jamal and the Canadian Rheumatology Association therapeutic committee for their support and guidance throughout the development of these recommendations.
APPENDIX 1.
EULAR/EUVAS definitions of disease states. From Hellmich, et al. Ann Rheum Dis 2007;66:605–17; with permission.
- Accepted for publication July 28, 2015.
REFERENCES
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.↵
- 106.↵
- 107.↵
- 108.↵
- 109.↵
- 110.↵
- 111.↵
- 112.↵
- 113.↵
- 114.↵
- 115.↵
- 116.↵
- 117.↵
- 118.↵
- 119.↵
- 120.↵
- 121.↵
- 122.↵
- 123.↵
- 124.↵
- 125.↵
- 126.↵
- 127.↵
- 128.↵
- 129.↵
- 130.↵
- 131.↵
- 132.↵
- 133.↵
- 134.↵
- 135.↵
- 136.↵
- 137.↵
- 138.↵
- 139.↵
- 140.↵








{kind=link}