

Abstract
Objective. To report on the progress of an ongoing research collaboration on magnetic resonance imaging (MRI) in juvenile idiopathic arthritis (JIA) and describe the proceedings of a meeting, held prior to Outcome Measures in Rheumatology (OMERACT) 12, bringing together the OMERACT MRI in JIA working group and the Health-e-Child radiology group. The goal of the meeting was to establish agreement on scoring definitions, locations, and scales for the assessment of MRI of patients with JIA for both large and small joints.
Methods. The collaborative work process included premeeting surveys, presentations, group discussions, consensus on scoring methods, pilot scoring, conjoint review, and discussion of a future research agenda.
Results. The meeting resulted in preliminary statements on the MR imaging protocol of the JIA knee and wrist and determination of the starting point for development of MRI scoring systems based on previous studies. It was also considered important to be descriptive rather than explanatory in the assessment of MRI in JIA (e.g., “thickening” instead of “hypertrophy”). Further, the group agreed that well-designed calibration sessions were warranted before any future scoring exercises were conducted.
Conclusion. The combined efforts of the OMERACT MRI in JIA working group and Health-e-Child included the assessment of currently available material in the literature and determination of the basis from which to start the development of MRI scoring systems for both the knee and wrist. The future research agenda for the knee and wrist will include establishment of MRI scoring systems, an atlas of MR imaging in healthy children, and MRI protocol requisites.
Between the Outcome Measures in Rheumatology (OMERACT) 11 and 12 meetings, 2 international initiatives on standardizing outcome measures in the field of magnetic resonance imaging (MRI) in juvenile idiopathic arthritis (JIA) combined forces. This resulted in a collaboration for ongoing research that enabled followup on the research agenda as set in the previous article1. The formation and progress of this collaboration within the field of MRI in JIA are further elaborated upon below.
JIA is a chronic autoinflammatory disease in childhood, affecting around 1 in 1000 children under the age of 162. MRI plays an increasingly important role in the diagnosis and monitoring of JIA, because of its multiplanar reconstruction capabilities and depiction of all possibly involved structures3. However, MRI is still underused in patients with JIA, partly because of the lack of standardized protocols for image acquisition and interpretation.
Although an internationally validated and accepted scoring system for MRI in JIA is not yet available for any joint, great efforts have already been made by different national and international study groups, e.g., the Health-e-Child radiology group and the OMERACT MRI in JIA working group. The Health-e-Child radiology group has focused on MRI of the wrist and hip joint, while the OMERACT MRI in JIA working group has aimed for 3 joint MRI scales, respectively, for large joints (knees and ankles), small joints (wrist and hands), and temporomandibular joints (outside the scope of this article)1.
From 2006 onward, the Health-e-Child radiology group, which involved the collaboration of pediatric musculoskeletal radiologists and clinical rheumatologists from 4 large pediatric centers, has aimed at developing an MRI scoring system for wrist involvement in JIA. The scoring system included 4 independent imaging features: bone edema4, bony erosions (Boavida, manuscript submitted), synovitis5, and tenosynovitis6. Validation of the scoring system showed that all features, except for the bone erosion score, had acceptable repeatability for clinical use. The development of an MRI scoring system for the large joints has been validated at a single center so far. The Juvenile Arthritis MRI scoring (JAMRIS) system is the only JIA-specific MRI scoring system for the knee and is proven to be feasible, reliable, and responsive to change7.
To continue with the research agenda as set at OMERACT 11 and described in a previous article1, the so-called Amsterdam November Meeting (ANOME) was attended by 10 participants from both the Health-e-Child radiology group and the OMERACT MRI in JIA working group. The goal of the ANOME as part of an ongoing research collaboration was to establish agreement on scoring definitions, locations, and scales for MRI assessment of JIA for large and small joints.
We report on the preparation for this meeting and the results of group discussions regarding the organization and content of the international consensus for standardization of MRI acquisition and interpretation in JIA.
MATERIALS AND METHODS
The program of the ANOME consisted of premeeting surveys, presentations, consensus on scoring methods, pilot scoring, conjoint review, and discussion of the future research agenda. Ten experts from 4 different countries participated in the ANOME: 2 pediatric rheumatologists, 1 musculoskeletal radiologist, 4 pediatric radiologists, and 3 research fellows.
Two surveys (i.e., on the knee and wrist) on MRI scoring systems consisting of multiple-choice questions on terminology, definitions, locations, and scale were sent to the participants before the meeting. The purpose of this survey was to get an overview of the participants’ point of view beforehand and to serve as a basis for the group discussions during the meeting.
In the initial meetings (Friday afternoon and Saturday morning), presentations of the MRI appearance of healthy and pathologic (JIA) findings in children constituted the basis for the subsequent group discussions. These discussions aimed at agreeing on a preliminary scoring system to be used for the pilot reading session during the ANOME, which was scheduled on Saturday afternoon. Sunday morning, in the conjoint review session, the incongruent cases were discussed in a plenary session, and adjustments were made to compose an improved, proposed scoring system.
RESULTS
Imaging Protocol
Preliminary statements on requisites for the MR imaging protocol of the JIA knee and wrist are summarized in Table 1. An inventory on the imaging protocol and corresponding specific parameters will be made by means of a survey. The next face-to-face meeting will lead to a final consensus on the requisites of the MR imaging protocols.
MR imaging protocol.
MRI Scoring System for JIA
First, the group agreed that the previous reliability studies served as an excellent basis for further development of scoring systems. Further, it was deemed important to be broadly “inclusive” in this stage of development, i.e., discuss whether we have included all relevant features available in the existing scoring systems4,5,6,7. Knowledge of the difference between healthy joints and JIA pathology on MRI is still limited and the accuracy of the findings on MRI is not yet determined8,9. Therefore it was considered important to be descriptive rather than explanatory regarding the definitions and terminology of the items of the scoring systems (e.g., synovial thickening instead of synovial hypertrophy). Further, the group agreed that well-designed calibration sessions were warranted before any scoring exercises were conducted.
Large joints
The development of an MRI scoring system for the large joints was based on the JAMRIS system for the knee7. JAMRIS comprises 4 MRI features: synovial hypertrophy, bone marrow changes suggestive of bone marrow edema, cartilage lesions, and bone erosions. The 3 latter features were adopted from the JAMRIS without any changes. Synovial hypertrophy was considered an inadequate term, because it is explanatory instead of descriptive. Therefore, the feature for inflammation of the synovium on MRI was split into 2 subitems: synovial thickening and synovial enhancement. It was agreed that measurement of synovial thickening was inaccurate because of lack of knowledge of synovial thickness in healthy controls and difficulties in standardizing this measurement. These findings led to a partial adoption of the recently innovated score for synovial abnormalities in the wrist, i.e., with a scale of 0–2 for synovial thickening (none-mild-moderate) and enhancement as scored based on comparison of signal intensity with the surrounding structures (i.e., muscle tissue and vessels)5.
Additional features were also discussed. Diffuse cartilage loss, tendinopathy, effusion, and Hoffa’s fat pad heterogeneity were considered of potential relevance for the scoring system for the knee. Future topics to be addressed for imaging of the knee in patients with JIA are the value of different MRI scoring systems for the knee, including those devised for other pediatric musculoskeletal disorders, and usefulness of higher field strength MRI10.
Small joints
The history of the development of an MRI scoring system for the arthritic wrist is shown in Figure 1. The group agreed on the need for reevaluation of the appearance of all anatomic structures at the wrist in healthy children to be able to discriminate normal variants from pathology and to look for specific locations for pathology versus normal findings.

Overview of previous studies on MRI scoring methods for the wrist with arthritis in both rheumatoid arthritis and juvenile idiopathic arthritis. MRI: magnetic resonance imaging; CMC: carpometacarpal joint; T2 fat-sat/STIR: fat-saturated/short-tau inversion recovery imaging; SI: signal intensity.
For the scoring of inflamed synovium at the wrist, the 3-component-score of the Health-e-Child radiology group was considered suitable (Figure 1)5. The thickening of synovium as scored in the knee is not separately assessed (or measured) in the wrist, but covered by the subitem “overall grade of inflammation.”
Also for bone marrow changes suggestive of edema, we chose to use the existing score4, in which the volume of the bone with bone marrow changes suggestive of bone marrow edema is estimated based on scrolling through the slices. Following the principle “describe not explain,” osteitis enhancing on MRI after intravenous contrast is also scored as bone marrow change suggestive of edema.
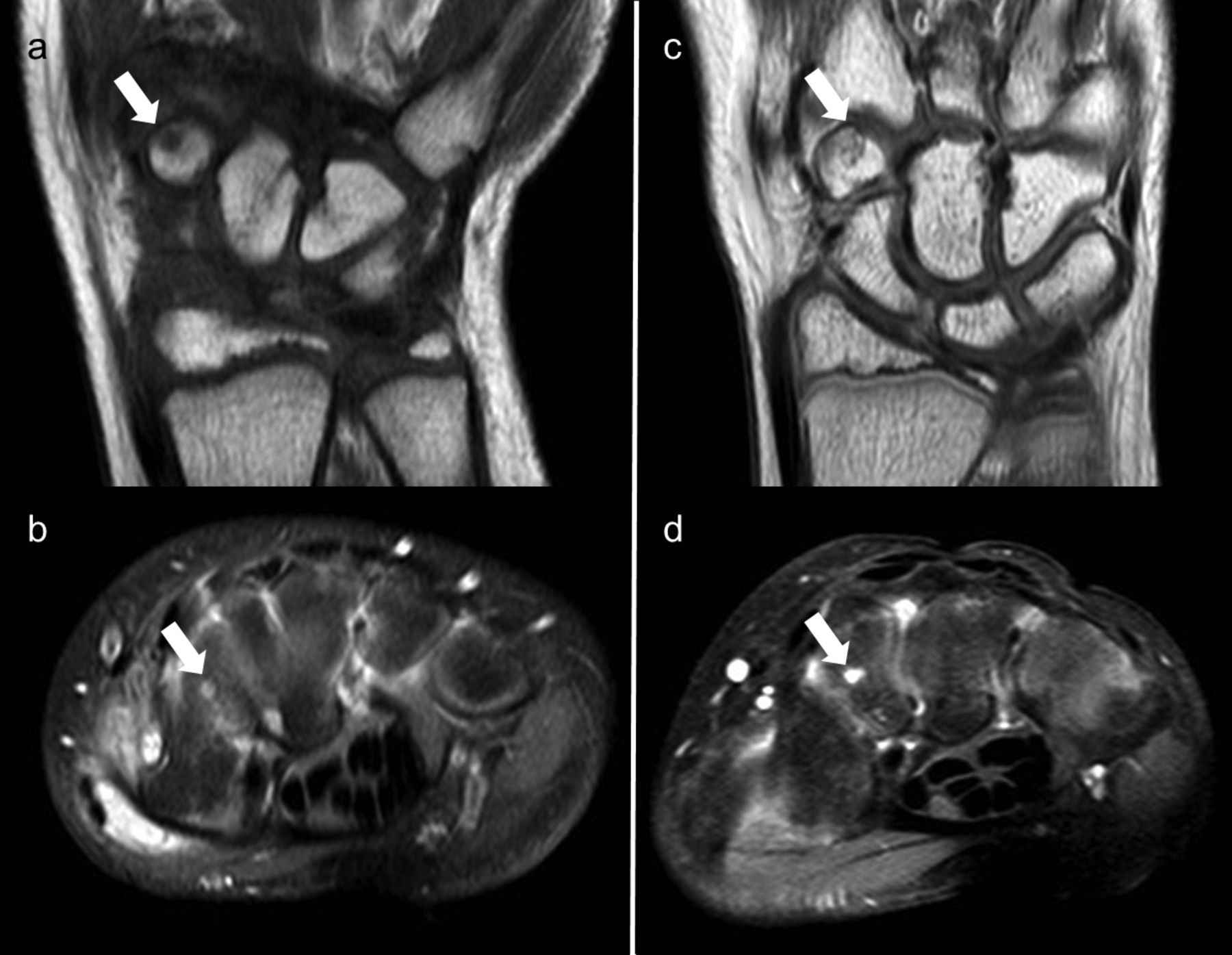
The most difficult feature of the MRI scoring system in the wrist is the distinction between normal bone depressions and bone erosions, as illustrated in Figures 2 and 3. In previous scoring systems, bony depressions were referred to as bone erosion11,12. However, the term “bone erosion” indicates that it is pathological, which is contradictory to the principle “describe not explain.” It was discussed whether the uncritical interpretation of bone erosions on MRI has misled us to reject the previous theory that, although they may appear, bone erosions are not the main feature of destructive change at the wrist, particularly in young children13,14. The definition of MRI damage developed for adult rheumatoid arthritis patients needs to be revised before it is applicable to pediatric patients. Additionally, the differences between the normal maturation process of the growing skeleton versus the pathological processes causing bone and cartilage destruction in patients with wrist inflammation need to be established. Therefore followup MRI examinations of both healthy children and patients with JIA should enable further understanding of the development of true erosions and hopefully enable us to differentiate between normal and pathological processes.
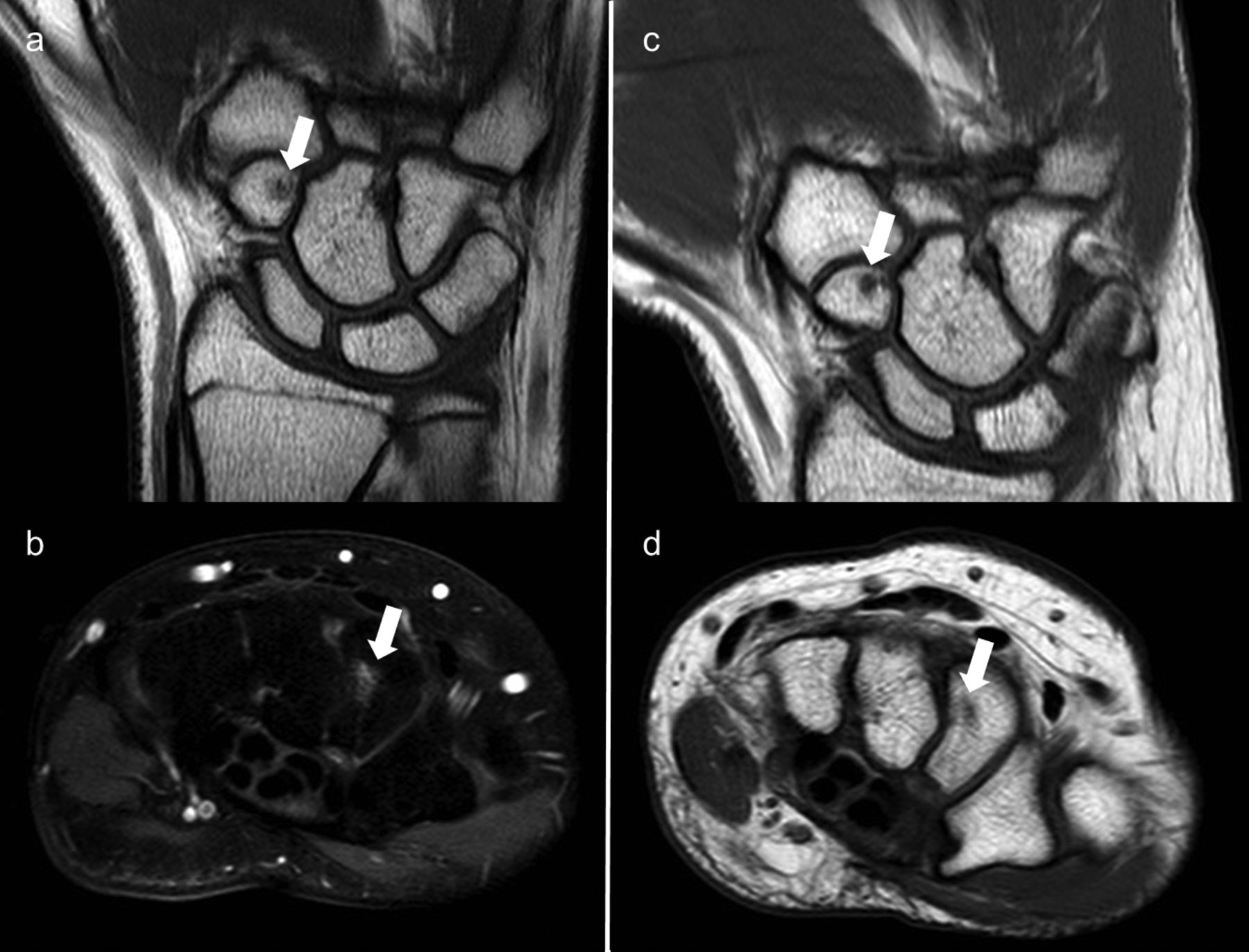
Area of bone depression (arrows) is visualized at baseline (a,b) and at followup (c,d) MRI scans of the wrist in a girl with JIA. At baseline both coronal T1-weighted (a) and axial T1-weighted fat-saturated MR images show an irregularity that would be scored as a bone erosion following the adult definitions. However, the followup MR images (c,d) fail to show any pathologic deterioration of the depression (i.e., synovial enhancement, enlargement of the lesion). MRI: magnetic resonance imaging; JIA: juvenile idiopathic arthritis.

MRI of the wrist of a girl with JIA shows an area of bone depression in the trapezium (arrows) similar to that of the patient in Figure 2 at baseline (a,b). But at followup, both the coronal T1-weighted (c) and axial T1-weighted fat-saturated images depict obvious synovial enhancement in the lesion, which is suggestive of a pathologic “bone erosion.” MRI: magnetic resonance imaging; JIA: juvenile idiopathic arthritis.
The evaluation of tenosynovitis and cartilage lesions in the wrist was outside the scope of the discussions of this meeting and should be reconsidered in the near future.
The research focus of the combined efforts of the OMERACT MRI in JIA working group and the Health-e-Child radiology group included the assessment of currently available material in the literature, and determination of the basis from where to start the development of MRI scoring systems for both the knee and wrist. Those steps combined with a future research agenda are summarized in Figure 4.

A schematic diagram representing the Amsterdam November Meeting in terms of conceptions beforehand, encountered problems, and current status.
Future goals of this ongoing research collaboration primarily include the consensus on an MRI scoring system for both the knee and the wrist. Further, an MRI atlas of the healthy knee and wrist will be developed. Additionally, requisites for an MR imaging protocol for both the knee and wrist of patients with JIA should be further established.








{kind=link}
{kind=link}
{kind=link}
{kind=link}