

Abstract
Objective. To determine the frequency of adverse events of diagnostic arthrocentesis in patients with possible gout.
Methods. Consecutive patients underwent arthrocentesis and were evaluated at 6 weeks to determine adverse events. The 95% CI were obtained by bootstrapping.
Results. Arthrocentesis was performed in 910 patients, and 887 (97.5%) were evaluated for adverse events. Any adverse event was observed in 12 participants (1.4%, 95% CI 0.6–2.1). There was 1 case (0.1%, 95% CI 0–0.34) of septic arthritis.
Conclusions. Diagnostic arthrocentesis is associated with a low frequency of adverse events. Septic arthritis rarely occurs.
Arthrocentesis is a common procedure in clinical practice, usually to obtain synovial fluid (SF) for diagnosing crystal arthritis or septic arthritis, or as a therapeutic procedure for glucocorticoid intraarticular injection. Hollander, et al introduced intraarticular glucocorticoid injections into rheumatology practice in the early 1950s and later reported on the results of a large number of therapeutic procedures1, showing a low rate of adverse events for intraarticular injections.
There is a generally held belief among rheumatologists that needle arthrocentesis is a safe and well-tolerated procedure. Needle arthrocentesis is a very useful, cost-effective, and usually straightforward skill that most nonspecialists can be trained to perform2,3. Although commonly not performed in primary care, it is a skill necessary to accurately and quickly diagnose gout. One possible concern with needle arthrocentesis in patients with inflamed joints may be a perception that needling through erythematous skin increases the risk of introducing bacteria into the joint, leading to septic arthritis. However, the safety of diagnostic arthrocentesis has not been previously studied systematically.
MATERIALS AND METHODS
The SUGAR project (Study for Updated Gout ClAssification CRiteria) was a multicenter study in which the gold standard for classification of gout was SF or tophus tissue polarizing microscopy. Every patient enrolled into the study routinely had either arthrocentesis to obtain SF or tophus tissue aspiration. The study protocol included systematic collection of data to determine the frequency of adverse events from diagnostic arthrocentesis.
This study was a cohort study with short-term followup of 6 weeks.
The SUGAR project has been previously described4. Briefly, consecutive patients with a recently swollen joint or subcutaneous nodule who were judged to possibly have gout by their treating rheumatologist were enrolled into a diagnostic study. Institutional review boards or ethics committees at each site approved the study protocol. All participants provided written informed consent.
All patients underwent arthrocentesis or nodule aspiration to provide fluid or tissue for polarizing microscopy. The technique of needle arthrocentesis was not standardized, but was performed by experienced rheumatologists according to local practice. In general, this consisted of anatomic localization of the puncture site, skin cleaning, and performing the puncture with a needle. Most investigators used chlorhexidine, povidone-iodine, 70% alcohol, or a combination to clean the skin. Nearly all investigators used a no-touch technique wearing nonsterile gloves. The needle size ranged from 20 g to 29 g for small joints and 18 g to 25 g for large joints. Local anesthesia was rarely used except for vapocoolant spray. Ultrasound was used by some investigators to localize needle placement.
This report includes all the study patients who underwent arthrocentesis. As part of the study protocol, patients were contacted by telephone or assessed at the clinic 6 weeks after the procedure and asked to report any adverse events. Serious adverse events were defined as life-threatening, leading to significant disability or permanent damage, resulting in a congenital anomaly, leading to hospitalization or death, or requiring medical intervention to prevent such outcomes. The clinical investigator, usually the treating rheumatologist, made a judgment rating on the likely causal relationship between the adverse event and the arthrocentesis (doubtful, possible, probable, very likely). A clinical grading of the severity of the adverse event (mild, moderate, or severe) was made by the clinical investigator, which aligned to the Common Terminology Criteria for Adverse Events severity grades of 1 (mild), 2 (moderate), and 3 to 5 (severe)5.
The number of events are presented with Poisson distribution 95% CI, calculated using exact limits from the chi-square distribution6. The 95% CI for the frequency of patients with adverse events who underwent arthrocentesis and who were evaluated at 6 weeks (denominator = 887) were obtained by bootstrapping. SPSS v22 (SPSS Inc.) was used for all analyses.
RESULTS
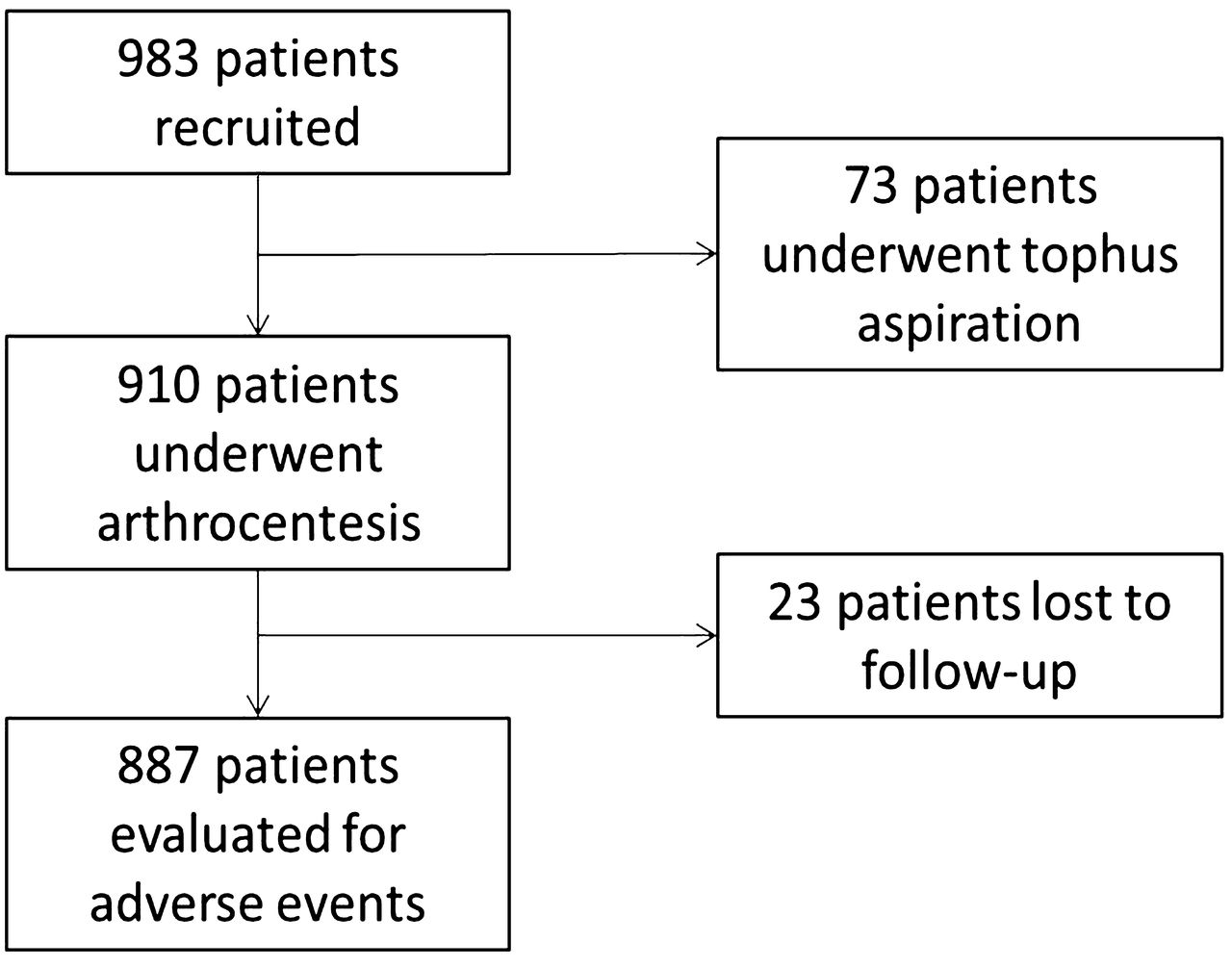
Twenty-five centers in 16 countries collected data from consecutively included 983 patients (509 gout cases, 474 non-gout cases), of whom 702 (71.4%) were men. Most patients underwent arthrocentesis (910, 92.7%); 73 patients underwent only suspected tophus aspiration and 21 patients underwent both arthrocentesis and suspected tophus aspiration (Figure 1). The most frequent sites for arthrocentesis were knee (58%), ankle (13%), and first metatarsophalangeal joint (13%). Adverse effects from nodule aspiration were not recorded.
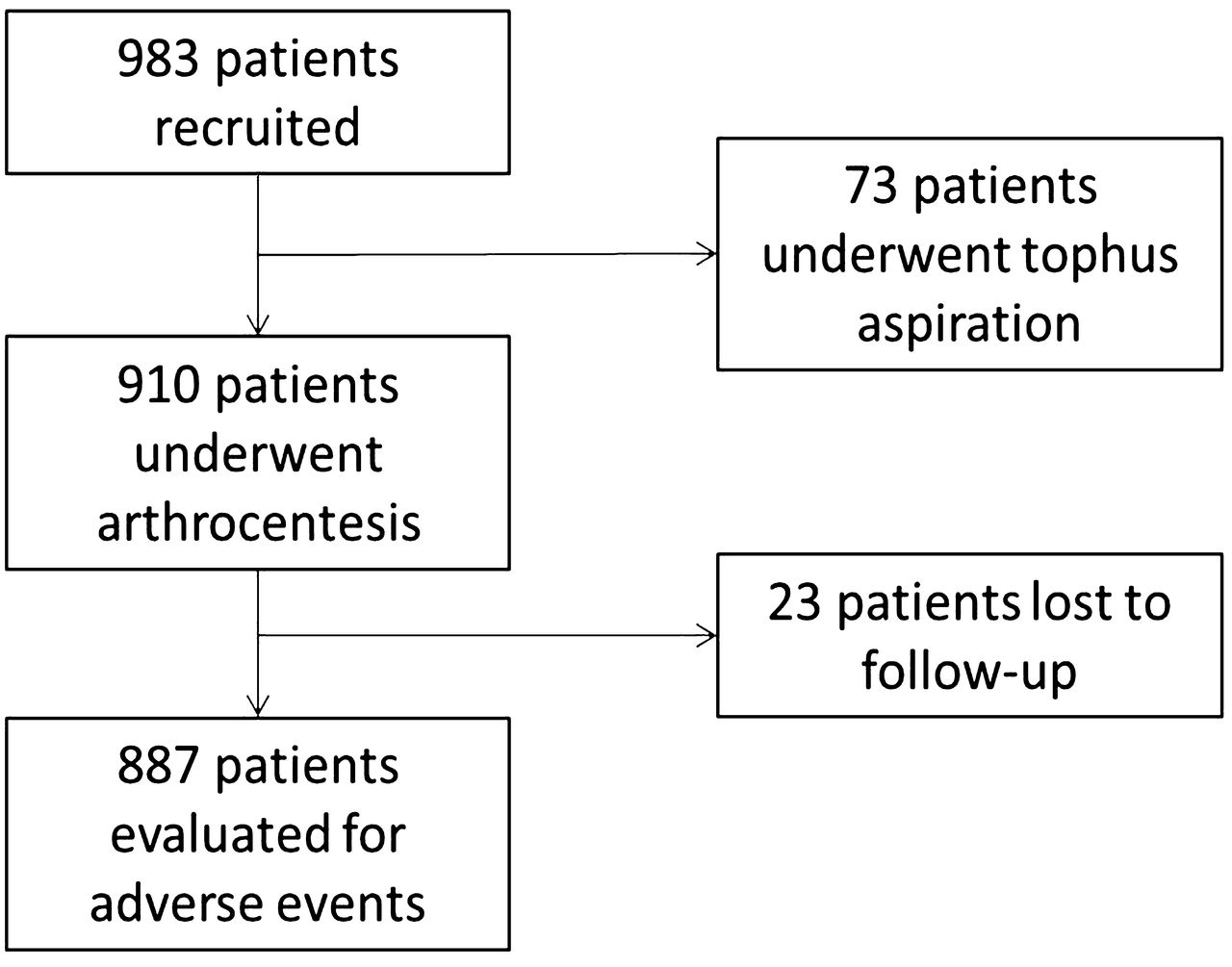
Flowchart showing patient recruitment and followup.
Of the 910 patients undergoing arthrocentesis, 23 patients (2.5%) were lost to followup despite at least 3 attempts to contact, resulting in 887 evaluable patients. There were 12 reported adverse events, of which 1 was a serious adverse event (Table 1). The most common adverse event was postprocedural pain, which occurred in 5 patients and which was nearly always rated as mild.
Adverse events following diagnostic arthrocentesis (n = 887 patients).
The 1 serious adverse event was a case of septic arthritis in a 24-year-old man with a 4-year history of joint symptoms and 10-day history of right knee pain and swelling, who underwent arthrocentesis of the right knee. SF fluid microscopy showed monosodium urate crystals and there was no growth on microbial culture. Eleven days after arthrocentesis, he presented with fever, right knee pain and swelling, and peripheral blood leukocytosis (17,800/ml). Repeated arthrocentesis showed monosodium urate crystals, but also cultured Staphylococcus aureus.
The patient was treated with intravenous cefalotin and made a full recovery. He was discharged from hospital after 16 days. Comorbidities included bipolar affective disorder and renal disease with moderate proteinuria (the cause of this was not known).
Overall, the occurrence of an adverse event was 13.5 per 1000 patient procedures (bootstrapped 95% CI 6–21) and serious adverse event was 1.1 per 1000 patient procedures (bootstrapped 95% CI 0–3.4).
DISCUSSION
Our study confirms the generally held belief that needle arthrocentesis is a safe and well-tolerated procedure. The very low rate of serious adverse events makes it difficult to estimate the frequency accurately. We observed a single case of septic arthritis following the joint puncture among 887 patients, which gives a bootstrapped 95% CI of between 0 and 3.4 per 1000 patients.
It has been previously reported that joint infection following intrasynovial glucocorticoid injection is very rare, occurring with a frequency (bootstrapped 95% CI) of 14 (7–22)1, 2 (0–5)7, and 7 (4–11)8, per 100,000 injections. It should be stressed that in these older studies, followup of patients was not clearly described and the denominator of the number of injections tended to be a simple estimate over a prolonged period of time. Also, 2 of these publications were from the same cohort. A study in patients with rheumatoid arthritis with a more complete description of the study population found 6 cases of septic arthritis following 10,000 joint injections, representing 60 (20–110) per 100,000 injections9. In addition, the CI in these studies were biased by an undetermined cluster effect because multiple injections were administered to the same patient.
The occurrence of joint infection in our present study was too infrequent to be able to determine whether the incidence is any different from what has been previously observed in intrasynovial glucocorticoid injections. Even though this was a reasonably large prospective study, it was still too small to provide multiple occurrences of very rare events, and this is the main limitation of the analysis.
Some other limitations include the expertise of the investigators performing arthrocentesis; less experienced operators may find a different rate of adverse events. Also, we did not record whether the needle passed through erythematous skin, which may conceivably influence the likelihood of bacterial contamination. Although patients taking anticoagulants were not excluded from our study, the decision to enroll such patients was at the clinical investigators’ discretion and it was not recorded whether the patient was taking anticoagulants at the time of arthrocentesis. It is possible that such patients experienced a higher rate of adverse events from arthrocentesis, but that possibility cannot be addressed from these data. It is also possible that the 6-week delay in assessing potential adverse events may have led to recall bias, especially by missing minor short-lived adverse events that might have been elicited within a few days of the procedure. Finally, attribution of causality was based solely on the opinion of the clinical investigator and may have been subject to bias.
Nonetheless, the strength of our current study is that unselected patients undergoing arthrocentesis were systematically and prospectively followed within a standardized protocol to determine short-term adverse events. This helps to minimize selection bias (choosing only patients with low risk of adverse events) and ascertainment bias (only identifying adverse events because they led to clinical presentations for care), both of which may occur in previously reported retrospective studies. Also, because these patients almost always underwent only a single arthrocentesis, the cluster effect was negligible.
The frequency of minor adverse events following arthrocentesis has not been previously reported because the focus of most prior reports has been adverse events from glucocorticoid injection (systemic effects, skin atrophy or depigmentation, tendon damage, postinjection flare). We observed a low frequency of pain, bruising, or joint swelling following arthrocentesis, which confirms that it is a safe and well-tolerated procedure. These data can be used to encourage clinicians to more often perform joint aspiration in the diagnostic investigations of patients who might have a crystal arthritis.
Acknowledgment
We gratefully acknowledge the help of the following with data collection, crystal examination, or patient referral: Joung-Liang Lan, Chien-Chung Huang, Po-Hao Huang, Hui-Ju Lin, and Su-Ting Chang (China Medical University Hospital, Taiwan); Anne Madigan (Dublin, Ireland); Yi-hsing Chen (Taichung, Taiwan); Alain Sanchez-Rodríguez and Eduardo Aranda-Arreola (Mexico City, Mexico); Viktoria Fana (Copenhagen, Denmark); Panomkorn Lhakum and Kanon Jatuworapruk (Chiang Mai, Thailand); Dianne Berendsen and Femke Lamers-Karnebeek (Nijmegen, the Netherlands); Olivier Peyr (Paris, France); Ana Beatriz Vargas dos Santos (Rio de Janeiro, Brazil); Fatima Kudaeva (Moscow, Russia); Angelo Gaffo (Birmingham, Alabama, USA); Douglas White (Hamilton, New Zealand); Giovanni Cagnotto (Pavia, Italy); Heidi Lunøe (Oslo, Norway); and Juris Lazovskis (Sydney, Nova Scotia, Canada).
Footnotes
Supported by the American College of Rheumatology, European League against Rheumatism, Arthritis New Zealand, Association Rhumatisme et Travail, and Asociación de Reumatólogos del Hospital de Cruces.
- Accepted for publication September 17, 2015.








{kind=link}