

Abstract
Objective. To assess the perspectives of women with lupus nephritis on barriers to medication decision making.
Methods. We used the nominal group technique (NGT), a structured process to elicit ideas from participants, for a formative assessment. Eight NGT meetings were conducted in English and moderated by an expert NGT researcher at 2 medical centers. Participants responded to the question: “What sorts of things make it hard for people to decide to take the medicines that doctors prescribe for treating their lupus kidney disease?” Patients nominated, discussed, and prioritized barriers to decisional processes involving medications for treating lupus nephritis.
Results. Fifty-one women with lupus nephritis with a mean age of 40.6 ± 13.3 years and disease duration of 11.8 ± 8.3 years participated in 8 NGT meetings: 26 African Americans (4 panels), 13 Hispanics (2 panels), and 12 whites (2 panels). Of the participants, 36.5% had obtained at least a college degree and 55.8% needed some help in reading health materials. Of the 248 responses generated (range 19–37 responses/panel), 100 responses (40%) were perceived by patients as having relatively greater importance than other barriers in their own decision-making processes. The most salient perceived barriers, as indicated by percent-weighted votes assigned, were known/anticipated side effects (15.6%), medication expense/ability to afford medications (8.2%), and the fear that the medication could cause other diseases (7.8%).
Conclusion. Women with lupus nephritis identified specific barriers to decisions related to medications. Information relevant to known/anticipated medication side effects and medication cost will form the basis of a patient guide for women with systemic lupus erythematosus, currently under development.
Qualitative research in patients with system lupus erythematosus (SLE) has focused mainly on disease experience1,2,3,4,5,6 or medication adherence7,8,9. Challenges with medication taking, including low medication adherence, are common in patients with lupus nephritis10,11. One key understudied aspect of medication adherence in chronic diseases is the process of medication decision making by patients12,13. Often at the time of a new diagnosis, patients are provided with a lot of new information, including the task of medication decision making. Medication decision making can pose challenges for a significant proportion of patients14.
Limited data are available on medication decision making in patients with lupus nephritis. It is not known what challenges patients with SLE encounter in decisional processes involving medications for the treatment of SLE prescribed by their doctors. The dilemmas that patients face in the medication decision-making process can provide insight into how effective patient education materials can be developed. Although the healthcare reform requires more patient-centered approaches, data to understand patient perspectives are generally lacking for many chronic diseases. Our study aims to fill this gap for patients with SLE.
Unlike previous qualitative work in the area of medication adherence, we used the nominal group technique (NGT) as a more structured approach to elicit both qualitative (ideas) and quantitative (ranking) data from patients15. Our objective was to identify a comprehensive array of patient-reported barriers (issues) and the relative difficulty that presented for African American, Hispanic, and white patients in their medication decision-making process. We oversampled for minorities in our study because they have more severe SLE and worse SLE outcomes16,17. Our research was guided by a single question aimed at assessing the impediments to the decisional processes involving medications for treating SLE. The findings from this study will be used to develop a patient-centered decision guide that can be tailored to the specific issues that individual patients consider when making decisions regarding their prescribed SLE medications.
MATERIALS AND METHODS
Study cohort
Patients were recruited from the SLE clinics at the University of Alabama at Birmingham (UAB) and the University of California at San Francisco (UCSF). All patients met the American College of Rheumatology classification criteria (1997) for SLE18 and had a diagnosis of lupus nephritis based on renal biopsy or laboratory findings when biopsy was refused/not undertaken. Purposefully, we oversampled racial/ethnic minorities, and nominal groups were stratified by race/ethnicity; patients above and below the federal poverty line were recruited (familiesusa.org/product/federal-poverty-guidelines).
Eight NGT meetings were convened with participants who had received treatment for lupus nephritis at the UAB and UCSF clinics; no limit was placed on when therapy was received. NGT meetings were conducted in English and moderated by an expert NGT researcher (RS) at UAB and UCSF between February and April 2014. Institutional review boards at UAB and UCSF approved the study.
NGT
The NGT meeting is a facilitated data collection activity that is structured to promote even and equal subject participation by minimizing the loss of information. There is evidence indicating that relative to interactive and less structured group data collection approaches, such as brainstorming and focus groups, the NGT when used correctly elicits a greater volume of novel and higher quality responses to a carefully articulated question19,20. Moreover, a potential source of investigator-induced interpretive bias resulting from transcribing and coding audio or video recordings is eliminated when using the NGT because verbatim responses are concisely documented on a flip chart as participants present them to the group.
We informed patients participating in each panel that the purpose of the meeting was to tap into their unique insights, knowledge, and lived experiences to identify different factors that increase the difficulty of their decision-making process involving prescribed medications. Following a brief explanation of the NGT process, patients were asked to work independently for about 5 min to develop their own lists of brief statements/phrases in response to the following question: “What sorts of things make it hard for people to decide to take the medicines that doctors prescribe for treating their lupus kidney disease?”
To help ensure that each panel generated a wide array of responses, patients were encouraged to think broadly about different types of challenges that affected (or could affect) their decisions involving prescribed medications. After about 5 min of independent work, they were asked to present their responses to the group. A “round-robin” nomination format was used to promote open disclosure, increase response volume, and to ensure all patients had an equal opportunity to present responses. This format involved having each participant, in turn, articulate a single response without providing any rationale, justification, or explanation for their response and without discussion or debate from other members in the panel. Each response was immediately recorded verbatim on a flip chart to help participants recollect previously nominated responses. This activity continued until no further responses could be generated. All responses were then discussed in a nonevaluative fashion to ensure that they were understood from a common perspective, and potentially to obtain additional insights15.
After this discussion, patients on each panel were asked to review the full list of responses generated during the meeting and then confidentially select 3 responses that reflected the most significant barriers in their own medication decision-making process. Patients recorded their selected responses on index cards and then ranked (prioritized) the significance of their selections from 1 to 3 by using weighted votes. The barrier that each patient perceived as most significant was assigned 3 votes by that patient, the second most significant by 2 votes, and the third most significant by 1 vote. The votes reflecting the individual rank orderings were collected and tabulated across patients in each group to determine the perceived relative importance of medication decision-making barriers and the level of agreement among patients about these perceptions.
To determine the relative importance of barriers for all patients, we first aggregated the responses that were generated by each of the 8 groups and combined responses that had the same or very similar wording. We then tabulated the number of patients from all groups that selected each response for ranking and calculated the sum of the weighted votes that it was assigned. A brief questionnaire was administered at the conclusion of each NGT meeting to obtain basic demographic data, education level, disease duration, and whether the patient needed assistance in reading materials. Data from this questionnaire were analyzed at the group level and not linked with individual responses generated during the NGT meetings.
RESULTS
Of the 55 patients who agreed to participate, 51 patients with lupus nephritis participated in 8 NGT meetings: 26 were African American (4 nominal groups), 13 were Hispanic (2 nominal groups), and 12 were white (2 nominal groups). Patients had a mean age of 40.6 years (SD 13.3), average disease duration was 11.8 years (SD 8.3), 36.5% had obtained at least a college degree, and 55.8% indicated a need for some help (from a family member, friend, and hospital or clinic staff) in reading health materials (Table 1).
Participant characteristics by NGT meeting panel (n = 52)*.
The 51 patients who participated in the 8 panels generated 248 perceived barriers (range 19–37 barriers per panel; Table 2). Of this total, 100 barriers (40%) were perceived by patients as reflecting relatively more important barriers in their own decision-making processes (i.e., were selected from each panel’s generated list of responses and then assigned weighted votes) than responses reflecting other barriers. Differences in the number of prioritized responses as a percentage of total generated responses were observed across the panels (range 32–54%). Relative to African American patients, white and Hispanic patients tended to endorse a smaller percentage of barriers as important (African American range 41–54%, white range 32–33%, Hispanic range 35–38%). Rescaled values expressing the level of agreement or consistency with which patients within panels independently agreed in their selections of the 3 most important decision barriers ranged from 40% for 1 patient panel (white Panel 1) to 67% for other patient panels (African American panels 3 and 4, and Hispanic Panel 1; Table 2).
Summary statistics for NGT meetings (n = 51).
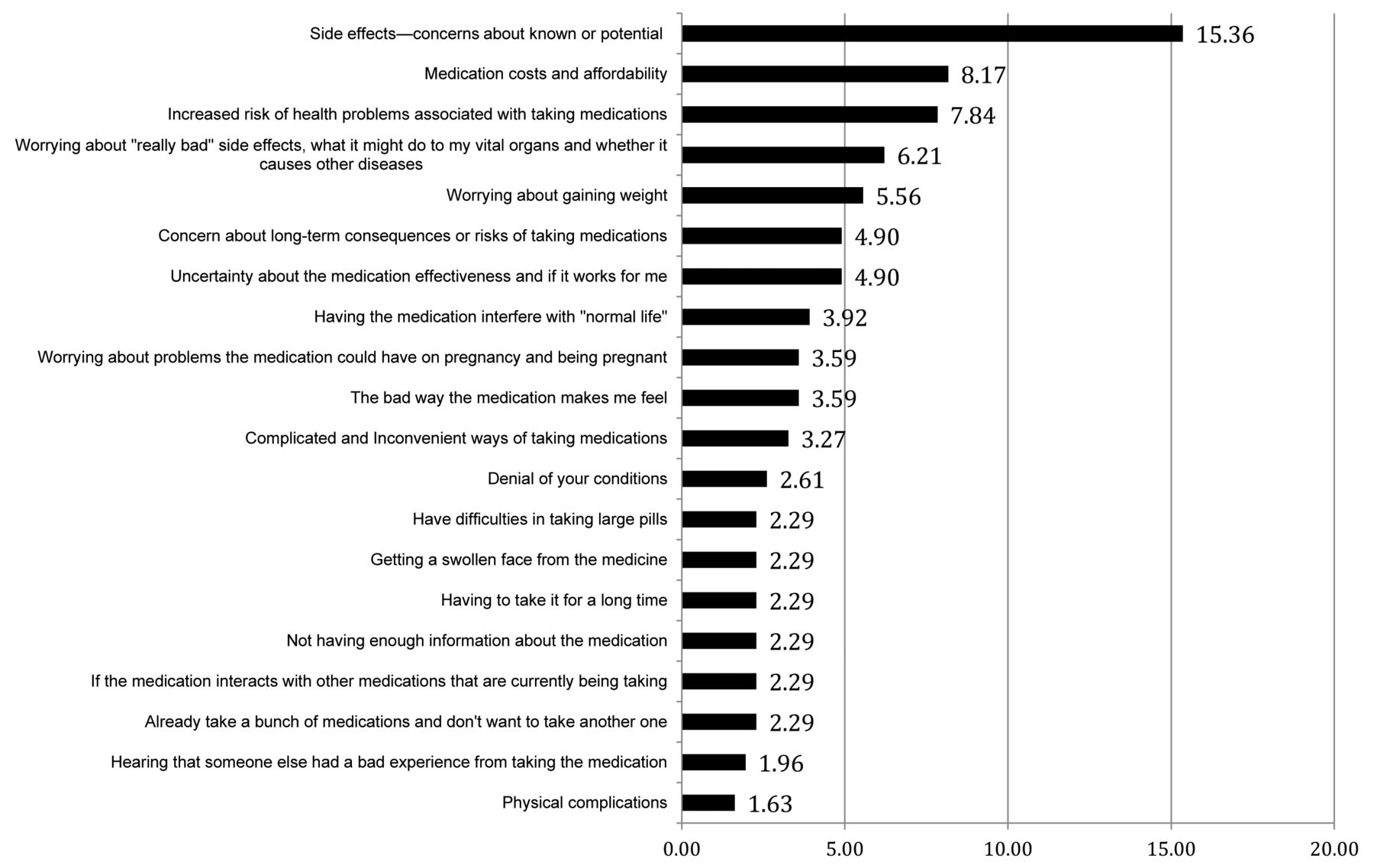
An aggregated response list, constructed by the investigators, based on combining the same or similarly worded responses from the 8 panels reflected 33 barriers that were endorsed as “important” by at least 1 patient nominal group panel (Table 3). Figure 1 shows the top 20 of these prioritized barriers across all nominal groups.

Top 20 barriers to medication decision making identified by patients with systemic lupus erythematosus (SLE). The figure shows the aggregated top 20 barriers to medication decision making related to SLE medications. These first 20 barriers accounted for 87.25% of weighted votes of all 33 selected barriers.
Patient identified barriers involved in the medication decision-making process (n = 51).
The specific responses as articulated by patients from different panels are provided in Supplementary Figure 1–8 (available online at jrheum.org). To assess the relative importance of barriers across panels, we considered, for each response, the number of panels selecting it, the number of times it was selected as important by individual patients (i.e., number of votes), and the sum of weighted votes it received. One-third (n = 11) of the responses from this list were endorsed as important by at least half of the participating panels. In addition, 14 responses were endorsed by 2 or 3 panels, and only 8 responses were endorsed by a single panel.
The most important responses that were endorsed by 4 or more panels reflected issues concerning (1) known or anticipated side effects, (2) uncertainty/doubts about medication efficacy, (3) medication expense/ability to pay for medications, (4) weight gain worries, (5) fears about the medication causing organ damage, (6) the bad way the medications make patients feel, (7) complicated and inconvenient ways of taking the medications, (8) fear that the medication could cause other diseases, (9) having the medication interfere with normal everyday activities, (10) worries about how the medication could affect ability to get pregnant/child bearing, and (11) denial of the condition (existence and how serious it is). Because the 51 patients were each asked to select only 3 responses to indicate the barriers they perceived as most important in their own medication decision-making processes, there were 153 possible endorsements that could be made. Of this total, 96 endorsements of importance (63%) were assigned to these 11 responses. When 6 additional endorsements for a 12th response, concerns about the longterm consequences/risks of taking the medications, was added to this list, the percentage of available endorsements accounted for increases to about 77%. The set of 12 responses that patients endorsed most frequently also accounted for almost 70% of the 306 weighted votes that could be assigned to selected responses. The most salient perceived barriers, as indicated by percentage of weighted votes assigned, were known or anticipated side effects (15.6%), medication expense/ability to pay for them (8.2%), and the fear that the medication could cause other diseases (7.8%). Patient quotes corresponding to these concerns are shown in Supplementary Table 1 (available online at jrheum.org).
DISCUSSION
Medications used for the treatment of lupus nephritis can be lifesaving and preserve kidney function. Medication adherence is poor, yet detailed insight into patient perceptions of barriers to medication use is not available. In our study, we used a novel and rigorous method to elicit these perceptions directly from at-risk patients. We elicited patient perceptions of barriers to the SLE medication decision-making process and then prioritized these using a voting procedure during 8 NGT meetings of white, Hispanic, and African American patients with lupus nephritis. Because the structure of NGT promotes even rates of participation and equally weights the input from all participants, the anonymously ranked responses provide a valid reflection of the collective views held by group participants21. In the absence of formative research in this area of medication decision making, the goals of our study were to identify a comprehensive array of patient-reported barriers and the relative significance (influence) that these are perceived to have for patients in their decisions involving medications. This semiquantitative formative study enrolled patients from various races/ethnicities to allow generalizability, and purposefully oversampled for minority patients with lupus nephritis because research in that area is limited and they have worse SLE outcomes16,17. The identification of several medication decision-making difficulties in patients with lupus nephritis paves the way for the creation of a patient decision aid/guide to help patients make more informed decisions about lupus nephritis treatments. As in our study, the NGT can be used in formative research to obtain important insights in numerous contexts if a carefully articulated question based on a clear understanding of specified information needs can be addressed by a representative group of knowledgeable informants21,22,23,24,25.
Responses to barriers to SLE medication adherence decision making appeared to fall into several key categories, including medication side effects, costs and affordability, negative effects on physical appearance, efficacy doubts, concerns about how the medications could affect health and risk for other diseases, medication interfering with normal life activities, conception and pregnancy issues, and complicated and inconvenient ways of taking medications.
Side effects were perceived by participants as a major impediment to decision making regarding SLE medications with 7 of 8 nominal groups identifying 2–4 responses related to side effects among the prioritized barriers. Such a frequent occurrence of responses related to side effects in nominal groups emphasizes the major role that side effects play in patients’ decision making regarding SLE medications. Side effect concerns predominantly included the worry about common side effects and longterm side effects, vital organ damage because of medication, the higher likelihood of getting sick while taking immunosuppressants, the effect on medical comorbidities, and the interaction with other medications. Patients’ actual experience with harmful side effects was only brought up in 1 nominal group. The most surprising aspect was that all other dimensions of side effects were discussed much more frequently than patient’s own experience of side effects and seemed to have a significant effect on medication decision making. This indicates that patient concern about medication side effects may be as or more important in medication decision making than experiencing side effects, and deserves key emphasis in patient-physician discussions prior to starting SLE medications.
Thus, while previous qualitative studies found that the fear of side effects was an important barrier7,8,9, our study is among the first to explore this important patient concern in detail and highlights its various dimensions that concern patients with lupus nephritis. These findings align with previous findings regarding patient preferences about SLE medication treatment, a related but somewhat different construct from the medication decision-making process that we examined. Medication efficacy and the risk for infection had the greatest effect on patient preference in a conjoint analysis of patients with SLE to evaluate patient treatment preferences26, and medication toxicity made patients favor azathioprine over cyclophosphamide when both drugs would confer an equal probability of renal survival27. Our detailed study provided us with an understanding of barriers to medication decision making and these findings will inform the design of a patient decision guide for the treatment for lupus nephritis.
An important contribution of our NGT study was the demonstration of other key barriers to medication decision making in patients with lupus nephritis. These included medication interfering with normal life activities, the interference of medication with pregnancy, and doubts about medication efficacy. Disruption to lifestyle and interference with daily activities because of lupus medication is a serious problem for a patient who is trying to incorporate a new habit of taking multiple daily medications for the first time in her/his life. A novel study finding was that the opinion of peers and the healthcare provider about how likely these medications could benefit or harm was very important to the patients. A practical implication of this finding is that healthcare providers and teams should use more efficient and effective ways to provide the information regarding these therapies to patients making decisions about medications and acknowledge the importance of peer opinion. Providing information and facilitating access to trustworthy resources, such as the Lupus Foundation of America and other SLE advocacy organizations, will help patients with SLE connect with well-informed peers and make informed medication decisions.
Patients commonly cited their fear that lupus nephritis medications might lead to other diseases. Corticosteroids can lead to several potential side effects with longterm use (i.e., osteoporosis, cataracts, etc.). Immunosuppressants are usually well tolerated and associated with some side effects, such as nausea, gastrointestinal upset, infections, etc. Significant benefits of renal function preservation and prevention of dialysis dependence (that may then lead to mortality benefit) and prevention of extrarenal flares make the risk-benefit ratio of immunosuppressants quite favorable in lupus nephritis. Thus, 1 key objective of our proposed lupus patient guide/decision aid is to provide a balanced view of risks and benefits of these treatments in lupus nephritis, so that patients can make informed decisions that align with their values and preferences and give them the most benefit.
Our findings of barriers to patient medication decision making (important before starting medications) have some overlap with findings from studies of medication adherence (important after starting medications), such as the belief that continuous longterm medications were not needed and the fear of the medication side effects7; perceived lack of efficacy, financial burden, health system access, and language barriers8; concerns regarding their necessity, side effects, or perceived lack of their efficacy9; medication cost and forgetfulness8,28; concerns about medication use29; lower education level, lower socioeconomic status, being single, and low health literacy8,30,31; and depression, medication concerns, physical symptoms, and short-term memory problems28. Similar findings were reported in a systematic review of nonadherence to SLE medications32. Effective communication by clinicians promoted a sense of trust and respect among patients with SLE32, indicating its importance in modifying medication adherence.
So what is the optimal way to develop a patient decision guide? Patients listed the desire for SLE education, need for assistance navigating the healthcare system, isolation at the time of diagnosis, and the emotional and physical barriers to care as the top targets for intervention; most (69%) favored a peer-support intervention1. Patients identified a lack of understanding of their disease and their needs by healthcare providers or people close to them as important barriers2. These and our findings suggest that an effective patient decision aid/guide to improve medication decision making in SLE would have to be multifaceted. It should target several important barriers, incorporate peer experience, and present patient-relevant discussions of benefits and harms to enhance communication.
These study findings must be interpreted while considering study limitations. It is possible that patients from other geographical areas, culture, or minority groups (e.g., Asians, etc.) may have different barriers to SLE medication decision making and our findings may not apply to those groups; we recruited patients across the spectrum of socioeconomic status and race/ethnicity from 2 centers to improve the generalizability of our findings. We did not appreciate any obvious differences in medication decision making by race/ethnicity; therefore, it is possible that our findings may be generalizable to a wider SLE population. We are not able to differentiate which of these barriers are related to the use of corticosteroids versus immunosuppressants. However, this was intentional and was based on an extensive discussion by the research team that weighed the pros/cons of assessing barriers to specific medications versus lupus nephritis medications as a group, and decided to explore barriers to lupus nephritis medications as a group.
Hispanic group participants were fluent in English and provided data during the nominal groups conducted in English (were bilingual). We considered conducting groups in men with SLE and in Spanish in Hispanics. Limited by resources and time, we could not conduct those nominal groups. It is possible that findings might differ by sex or language. In particular, concerns regarding pregnancy and breastfeeding are sex-specific, and it is possible that men might prioritize these concerns differently. Detailed information regarding adherence to each SLE medication was not collected; however, we attempted to choose a representative sample of patients from our SLE clinic and it is quite likely that patients with a wide range of medication adherence participated in our nominal groups.
We found that African American, Hispanic, and white women with lupus nephritis identified several barriers to decision making regarding SLE treatments. The nominal group approach allowed semiquantitative formative evaluation of these barriers. These findings will inform the development of a patient guide for patients with lupus nephritis that will then be tested in a randomized study.
ONLINE SUPPLEMENT
Supplementary data for this article are available online at jrheum.org.
Footnotes
This material is the result of work supported by the research contract CE-1304-6631 from the Patient-Centered Outcomes Research Institute. J.A. Singh is also supported by the resources and the use of facilities at the VA Medical Center at Birmingham, Alabama, USA, and research grants from these US agencies: Agency for Health Quality and Research Center for Education and Research on Therapeutics U19 HS021110, National Institute of Arthritis and Musculoskeletal and Skin Diseases P50 AR060772 and U34 AR062891, National Institute on Aging U01 AG018947, and the National Cancer Institute U10 CA149950. J. Yazdany is also supported by the US National Institutes of Health K23 AR060259 and the Rosalind Russell Medical Research Center for Arthritis.
- Accepted for publication April 30, 2015.








{kind=link}