

Abstract
Objective. To assess whether intraarticular corticosteroid injection (CSI) reduces inflammation of the temporomandibular joint (TMJ), prevents growth disturbances of the mandibular condyle, and restores normal growth of the mandibular ramus.
Methods. Retrospective longitudinal magnetic resonance imaging (MRI) evaluation of inflammatory activity, TMJ deformity, and mandibular ramus height in 33 children (23 girls, median age 5.2 yrs) over a median period of 5 years following repetitive CSI to the TMJ.
Results. Intraarticular location of CSI led to inflammatory grade improvement in 53% at first MRI followup compared to 20% with extraarticular location (p = 0.005), with more improvement of the mean inflammatory grade after intraarticular CSI (p = 0.001). Rate of osseous deformities of the TMJ deteriorated from 51% at study inclusion to 62% at end of observation period, with progression to severe condylar destruction in 26% of joints including 24% with development of intraarticular calcifications/ossifications. Mean short-term growth rates of the mandibular ramus were negative for intraarticular CSI while positive for extraarticular CSI (p = 0.036). Mean longterm mandibular ramus growth rate (0.7 ± 0.8 mm/yr) after CSI was significantly lower than reported normal mean age- and sex-matched growth rate (1.4 ± 0.1 mm/yr, p < 0.0001).
Conclusion. Despite improving the inflammatory activity as seen on MRI, repetitive CSI to the TMJ does not reach the treatment goals to prevent progressive osseous deformation and to normalize mandibular ramus growth in children with juvenile idiopathic arthritis.
- TEMPOROMANDIBULAR JOINT
- JUVENILE IDIOPATHIC ARTHRITIS
- STEROIDS
- INTRAARTICULAR INJECTIONS
- MAGNETIC RESONANCE IMAGING
Arthritic involvement of the temporomandibular joint (TMJ) has a high prevalence in children with juvenile idiopathic arthritis (JIA)1,2, which often results in joint damage and craniofacial growth disturbances3. The unique anatomy of the mandibular condyle, with bone formation taking place from secondary cartilage directly beneath a thin fibrocartilage layer, makes the growth susceptible to effects related to other biological processes such as inflammation. Early detection and treatment of TMJ arthritis is considered essential to maintain normal development of the mandibular condyle and growth of the mandibular ramus in children.
Local therapy with intraarticular corticosteroid injections (CSI) is effectively and safely used in peripheral joints and has also been introduced for TMJ arthritis4,5,6,7,8. Although there is evidence for clinical and radiological improvement of TMJ arthritis following CSI, there are no data, to our knowledge, showing improvement or normalization of mandibular growth9.
Because TMJ arthritis may frequently be asymptomatic and difficult to diagnose clinically10,11, contrast-enhanced magnetic resonance imaging (MRI) is considered the gold standard for detecting early inflammatory involvement of the TMJ12. In addition, MRI allows assessment of the level of inflammation, osseous deformity of the TMJ, and the height of the mandibular ramus13,14.
The aim of our study was to assess whether intraarticular CSI improves inflammation of the TMJ, prevents growth disturbances of the condyle, and restores normal growth of the mandibular ramus.
MATERIALS AND METHODS
Patients
For this retrospective study, we included 33 consecutive children seen at our tertiary pediatric university hospital between June 2006 and November 2008 with a diagnosis of JIA according to the International League of Associations for Rheumatology 2003 criteria15, MRI diagnosis of TMJ arthritis, and subsequent CSI during the same sedation. During this period, MRI of the TMJ was performed routinely at a timepoint when TMJ involvement had a potential implication for treatment16. CSI was performed irrespective of symptoms or clinical findings when MRI indicated any degree of active inflammation represented by increased contrast enhancement of the TMJ. The study population consisted of 23 girls and 10 boys, aged 2–9.7 years (5.3 ± 1.9 yrs) with oligoarticular (n = 12), extended oligoarticular (n = 11), polyarticular disease (n = 8), or psoriatic subtype (n = 2). All CSI and MRI of the TMJ until early 2014 were evaluated. Followup MRI was usually performed at about 2–4 months after the CSI and later at intervals around 6–12 months (Figure 1). When TMJ arthritis had not improved on followup MRI, CSI was repeated. The CSI was performed by a pediatric rheumatologist without image guidance, but the location of the injected fluid into or around the TMJ was immediately checked by MRI. During the study period, the injected dose of triamcinolone hexacetonide varied from 6 mg to 20 mg per joint.
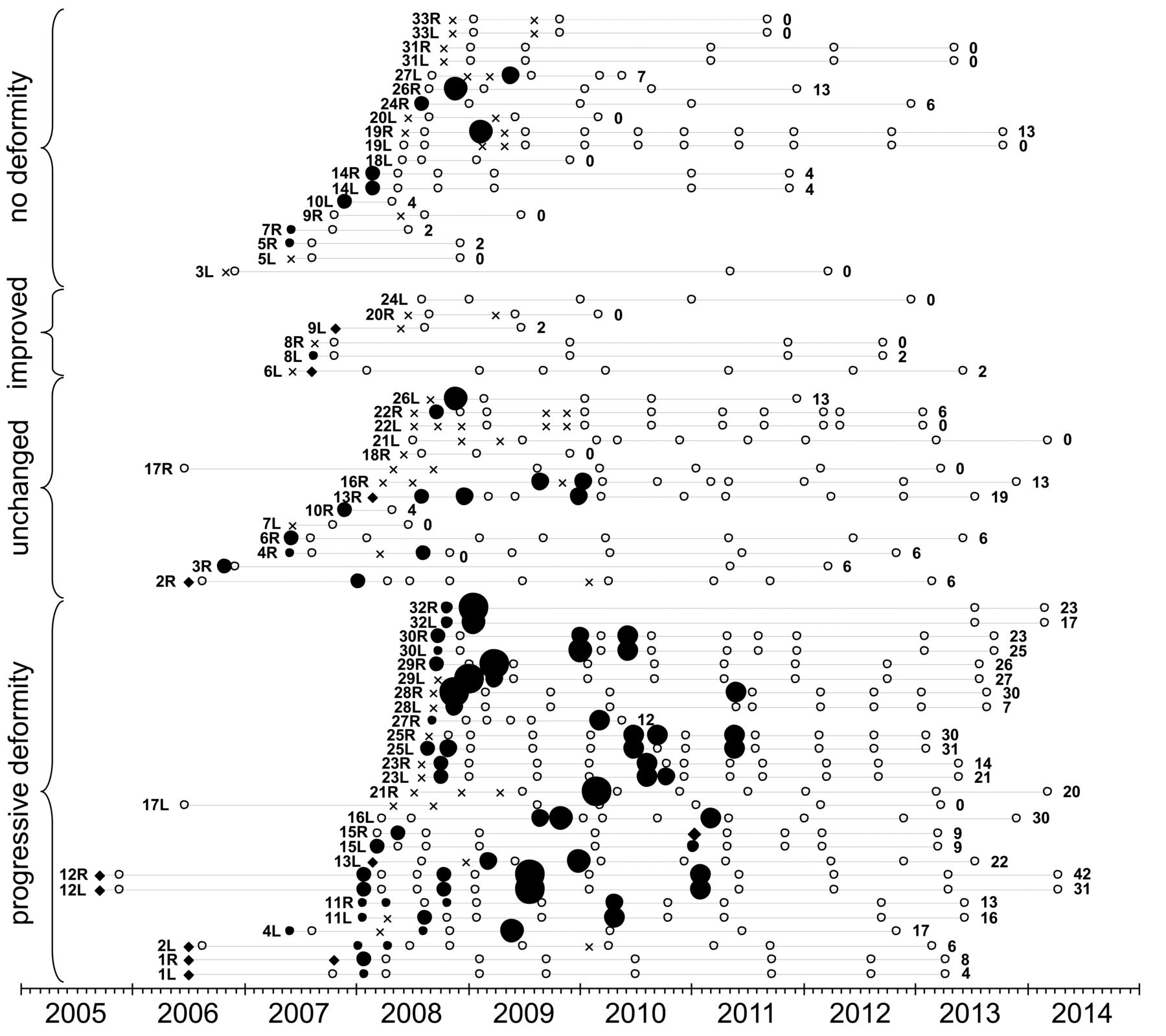
All magnetic resonance imaging (MRI) studies and corticosteroid injections (CSI) of each temporomandibular joint (TMJ) are plotted chronologically. The TMJ are grouped by the absence, improvement, stability, or progression of osseous deformities over the study period. Each TMJ is annotated by patient number and R for right or L for left joint. The cumulative dose index over the entire study period is given on the right side in mg. Empty circle (○): MRI study without CSI; filled circle (●): intraarticular CSI; multiplication sign (×) represents an extraarticular CSI; and rhombus (◆) represents a CSI without evaluation of the amount of intraarticular corticosteroid. Datapoint size represents the intraarticular corticosteroid dose index.
All contrast-enhanced MRI were performed at 1.5 Tesla. The MRI protocol is given in Supplementary Table 1 (available online at jrheum.org).
All patients and/or their legal guardians gave informed consent for MRI and CSI, which had been clinically indicated by the responsible pediatric rheumatologist. Legal guardians signed a general waiver for analysis of patient data in the hospital chart. Retrospective analysis of patient data and imaging studies was approved by the institutional and cantonal research ethics boards.
Methods
Groups of TMJ with (1) successful intraarticular CSI, and (2) where intraarticular injection had failed, resulting in extraarticular placement of the corticosteroid (extraarticular CSI) were compared for the degree of bony deformation and level of inflammation, as assessed by MRI before and after CSI. Growth rates of the mandibular ramus were calculated from mandibular ramus height measurements and compared between TMJ with (1) intraarticular CSI, (2) extraarticular CSI, and (3) joints where initially no inflammation was detected and no CSI performed. Total cumulative intraarticular corticosteroid dose per joint was compared between groups of TMJ with different degrees of bony deformation and longterm growth rates. Longterm mandibular ramus growth rates of the TMJ studied were compared to age- and sex-matched normal growth rates from the literature, which were based on longitudinal cephalographic measurements between the constructed landmarks condylion and gonion in 102 children from 3 to 16 years of age17,18.
Statistics
Descriptive data are given as mean ± SD for normally distributed continuous variables and ordinal variables, or as median and interquartile range for continuous variables without normal distribution. Normal distribution of continuous data was checked with the Shapiro-Wilk test. For comparisons of joint characteristics before and after CSI, a paired sample t-test was used for continuous variables (ramus height, growth rate) and the Wilcoxon signed-rank test for ordinal variables (grade of inflammation). For comparisons between groups, an independent samples t-test was used for continuous variables or Mann-Whitney U test for ordinal variables. Frequency of JIA subtypes in extraarticular and intraarticular CSI were assessed with the chi-squared test. Inflammatory and deformity grades at the first CSI were correlated with the age, age at JIA onset, and time since JIA onset for each patient, using Spearman rank correlation. All analyses were conducted with MedCalc statistical software version 13.2.0 (MedCalc Software bvba), considering p < 0.05 statistically significant.
MRI evaluation
All MRI studies performed during the study period were reviewed by 2 pediatric radiologists (NL, CJK) for signs of TMJ inflammation in a consensus reading. Presence and degree of joint effusion, synovial thickening, and bone marrow edema were assessed on fat-saturated T2-weighted images. Presence and extension of joint enhancement was assessed on early contrast-enhanced images. Inflammatory activity of the TMJ was graded semiquantitatively on a 4-grade scale (grades 0–3; Table 1). Shape and integrity of the temporal bone (articular eminence and glenoid fossa) and mandibular condyle were assessed on the 3-D gradient echo images. Osseous deformity was also graded semiquantitatively on a 4-grade scale (Table 1). Intraarticular calcification/ossification were defined as corpuscular lesions with low signal intensity within the joint space. Mandibular ramus height was measured on minimum intensity projection images, on a line parallel to the posterior border of the ramus through the most cranial point of the condyle to the intersection with the inferior border of the ramus14.
MRI scoring system for inflammatory activity and osseous deformity of TMJ.
The CSI were classified as extraarticular or intraarticular based on the amount of fluid visible within the joint space: all injected fluid located periarticularly without any increase of intraarticular fluid for extraarticular CSI and visible increase of fluid within the joint space for intraarticular CSI. The amount of intraarticular corticosteroid was graded semiquantitatively on a 4-grade scale: grade 0, extraarticular injection (no fluid in joint space); grade 1, small intraarticular injection (little fluid in joint space); grade 2, moderate intraarticular injection (moderate amount of fluid in joint space); and grade 3, large intraarticular injection (large amount of fluid in joint space; Supplementary Figure 1, available online at jrheum.org). This 4-grade scale was used to calculate an intraarticular dose index based on the grade of visible fluid intraarticularly and injected corticosteroid dose (grade of visible intraarticular fluid multiplied by injected corticosteroid dose and divided by 3), which served as estimate of the amount of intraarticularly applied corticosteroid.
RESULTS
Corticosteroid injections
During the observation period, a total of 156 CSI were performed. Two of the 66 TMJ were never injected, 19 TMJ were injected once, and 45 were injected repeatedly (2.4 ± 1.4 CSI per joint, range 0–7 CSI). In 15 CSI, the location of the injected fluid was not checked with a control sequence and these CSI were excluded from the comparisons between intraarticular and extraarticular CSI, but for estimation of the dose index a small amount of intraarticular fluid (grade 1) was assumed. The injected fluid was located extraarticularly in 42% (59/141) of CSI in which a control sequence had been performed. An increase of the intraarticular fluid was seen in 58% (82/141) of CSI, with a small amount of fluid in 28, a moderate amount in 25, and a large amount in 29 cases. With the corticosteroid dose varying from 6–20 mg (11 ± 6 mg) triamcinolone hexa-cetonide per CSI, the resulting corticosteroid dose index ranged from 0 to 20 mg (4 ± 5 mg) per CSI. The total injected corticosteroid dose was 6–72 mg (26 ± 18 mg) per joint and the cumulative corticosteroid dose index ranged from 0 to 42 mg per joint (10 ± 11 mg). The rate of intraarticular CSI and corticosteroid dose index increased during the study period, from 52% and 2 ± 2 mg for the first 70 joint injections to 63% and 6 ± 6 mg for the later 71 joint injections (p < 0.0001).
The distribution of JIA subtypes between the joints with extraarticular and intraarticular CSI was not significantly different (p = 0.76). Also, the age at which a joint was injected, the age of JIA onset, the injected corticosteroid dose, the degree of osseous deformity, the level of inflammation before CSI, and the time interval since a previous CSI were not significantly different (Table 2). However, joints with intraarticular CSI had previously been injected more often, resulting in a higher cumulative intraarticular corticosteroid dose index (Table 2).
Characteristics, inflammatory grades, and growth following intraarticular and extraarticular corticosteroid injections. Data are mean ± SD unless otherwise indicated.
TMJ inflammation
The rate of edematous to fatty bone marrow conversion, decrease of the extension of joint enhancement, and resolution of synovial thickening following CSI (Figure 2) were more frequent with a higher intraarticular amount of the injected corticosteroid. At the first followup MRI performed at 2.5 months (2.3–3.2) after CSI, the inflammatory grade of the TMJ improved in 53% of the intraarticular injections, whereas with extraarticular injection improvement was seen in only 20% (Table 2). The mean grade of inflammation improved more for intraarticular CSI (from 1.56 to 0.95, p < 0.0001) than for extraarticular CSI (from 1.36 to 1.19, p = 0.04), while the initial degree of inflammation before CSI had not been significantly different between both groups (p = 0.09). The grade of inflammation before the first CSI showed no significant correlation with the patient’s age (rs = 0.078, p = 0.54) or age at JIA onset (rs = −0.120, p = 0.35), and only weak correlation with the time interval since JIA onset (rs = 0.244, p = 0.05).

Sagittal oblique magnetic resonance images before (a, b) and 3 months after intraarticular corticosteroid injection (c, d). Fat-saturated T2-weighted images (a, c) show resolution of bone marrow edema in condyle, small joint effusion, and synovial thickening. Contrast-enhanced fat-saturated T1-weighted images (b, d) show improvement of joint space enhancement.
Osseous deformity
At the time of inclusion in the study, 49% of TMJ showed normal bony morphology, 36% had mild, and 15% moderate deformity of the temporal bone and mandibular condyle. The grade of osseous deformity showed no significant correlation with the patient’s age (rs = 0.194, p = 0.12), age at JIA onset (rs = −0.014, p = 0.91), and time interval since JIA onset (rs = 0.126, p = 0.32). At immediate followup MRI 2.5 months (2.3–3.2) after CSI, the grade of osseous deformity was unchanged in all cases. During the entire study period, 29% of TMJ retained normal osseous morphology, while the grade of osseous deformity improved in 9%, remained stable in 21%, and deteriorated in 41% of TMJ. The number of CSI and the mean cumulative corticosteroid dose index in the 27 TMJ with progressive deformation (3.2 ± 1.2 CSI, 19 ± 10 mg) was significantly higher than in the other TMJ (1.8 ± 1.2 CSI, 4 ± 5 mg, p < 0.0001). At the end of the observation period, 38% of TMJ showed normal osseous morphology, 18% had mild deformities, and 18% moderate ones. Twenty-six percent of TMJ had progressed to severe osseous deformity, including 24% (16/66) with destroyed condyles and 21% (14/66) with intraarticular calcifications/ossifications (Figure 3). The TMJ with destroyed condyles and ossifications had received a large amount of intraarticular corticosteroid with a high cumulative dose index (23 ± 9 mg), which was significantly higher than in the other TMJ (6 ± 7 mg, p < 0.0001).

Sagittal oblique magnetic resonance images of the right TMJ in a 9-year-old girl following 3 CSI with a cumulative dose index of 30 mg. T1-weighted gradient echo image (a) shows destroyed mandibular condyle with new bone formation (osteophytes) at the mandibular neck, the articular eminence, and within the pannus (ossifications). Fat-saturated T2-weighted image (b) shows small joint effusion. Contrast-enhanced fat-saturated T1-weighted image (c) shows mild inhomogeneous patchy enhancement of the pannus, which expands the joint space. TMJ: temporomandibular joint; CSI: corticosteroid injections.
When comparing TMJ with progressive deformation (n = 27) and TMJ without progressive deformation (n = 39), these variables were not significantly different: age of JIA onset [2.5 yrs (1.7–5.6) vs 3.4 yrs (1.3–5.7); p = 0.81], age at first CSI (5.1 ± 1.9 yrs vs 5.4 ± 1.9 yrs, p = 0.56), and interval from JIA onset to first CSI [0.5 yrs (0.3–2.4) vs 1.3 yrs (0.4–2.9), p = 0.75].
Mandibular ramus growth
At inclusion in the study, 7/66 TMJ in 7 patients had no inflammation and received no CSI. In these 7 cases, mean mandibular ramus height increased at next followup MRI 3.7 months (2.4–5) later with a normal median growth rate of 1.4 (0.4–2.5) mm/yr. Following all 156 CSI, median ramus height was unchanged after 2.5 months (2.3–3.2) for the whole group [before CSI, 42.0 mm (38.7–47.1), at followup 42.4 mm (38.4–47.2), p = 0.89]. In the subgroup with intraarticular CSI (n = 82), median ramus height decreased from 41.7 mm (38.4–45.8) to 41.5 mm (37.7–46.3) at first followup MRI (p = 0.08) with a negative mean growth rate of −1.0 mm/yr (−4.5–2.6), whereas with extraarticular CSI (n = 59) median ramus height increased from 43.3 mm (39.7–48.0) to 43.9 mm (39.8–47.7; p = 0.17) with a median growth rate of 0.8 mm/yr (−2.1–3.9). Up to the next followup MRI 9.6 months (8.3–12.5) after CSI, available in 91 cases without repeated CSI in the interim, the median growth rate of the mandibular ramus was still significantly different between intraarticular CSI (n = 59) and extraarticular CSI (n = 32; Table 2).
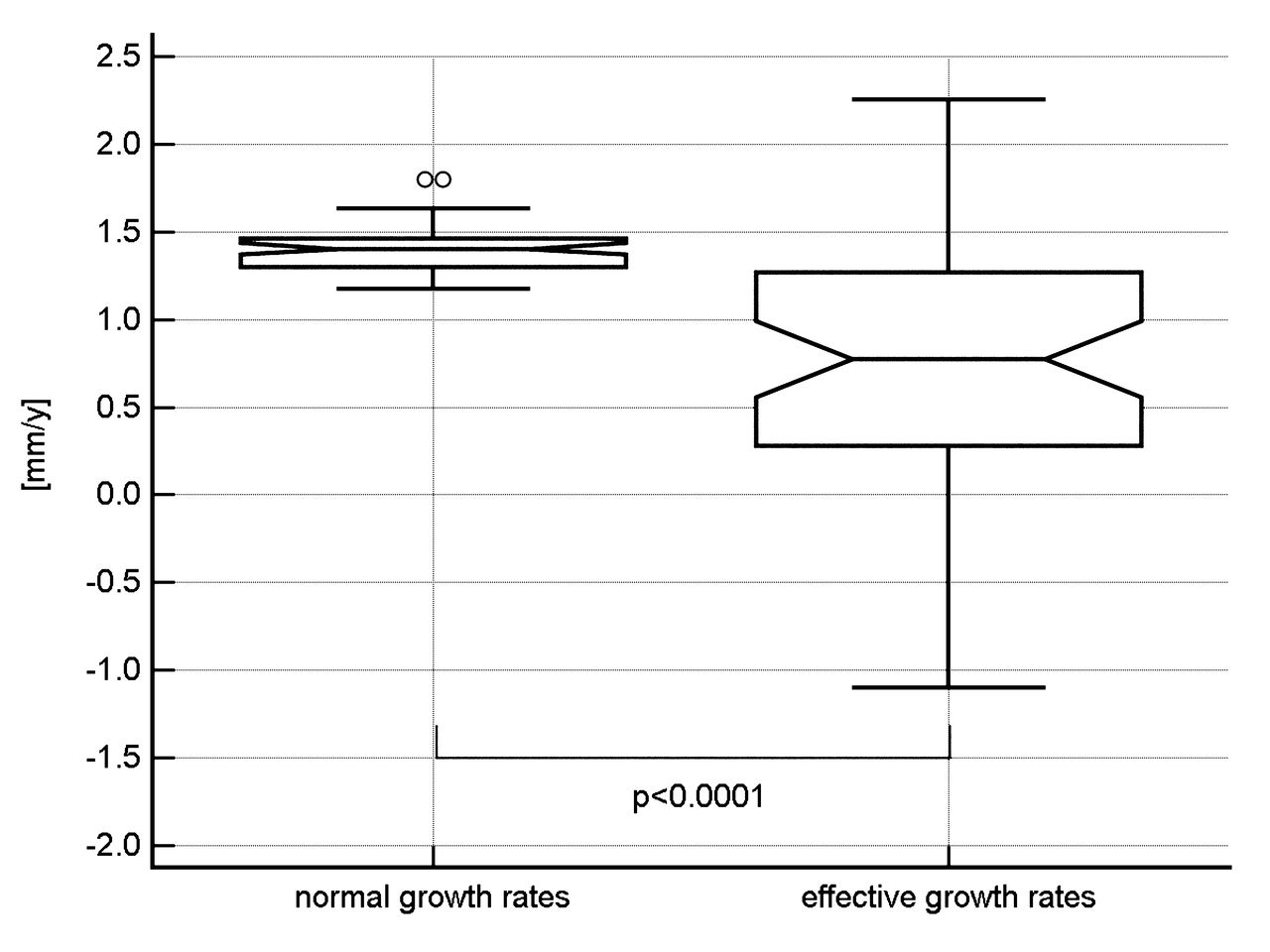
In 26 patients with MRI followup longer than 2 years, the mean longterm growth rate of the mandibular ramus was 0.7 ± 0.8 mm/y in the 5 ± 0.9-year interval since the beginning of the study, which was significantly lower than the expected sex- and age-matched normal mean growth rate of 1.4 ± 0.1 mm/yr (p < 0.0001; Figure 4). The TMJ with progressive osseous deformation (n = 26) had a lower mean longterm growth rate of 0.5 ± 0.9 mm/yr, while TMJ without deformation (n = 11) showed a higher longterm growth rate of 1.3 ± 0.6 mm/yr (p = 0.01). When comparing TMJ with low growth rate [0.3 (−0.3–0.53) mm/yr, n = 26] to TMJ with high growth rate [1.3 (1.0–1.7) mm/yr, n = 26], the TMJ with low growth rate had a significantly higher mean cumulative corticosteroid dose index (17 ± 11 mg) than those with a high growth rate (7 ± 8 mg, p = 0.0008). The mean patient age at first CSI was not significantly different for TMJ with low growth rates (5.5 ± 1.7/yr) than for TMJ with high growth rates (4.9 ± 2.1/yr, p = 0.23).

Notched box and whisker plot showing significantly decreased longterm growth rates (effective growth rates) compared to their age- and sex-matched normal growth rates in 26 patients (52 TMJ) with a mean followup of 5 ± 0.9 years. TMJ: temporomandibular joint.
DISCUSSION
With this longitudinal study of 33 children with JIA and TMJ arthritis, we demonstrate immediate and longterm effects of local corticosteroid therapy by MRI over a median followup period of 5 years. To our knowledge, this is the first attempt to assess outcome of CSI to TMJ by measuring mandibular ramus growth with MRI.
Articular CSI have been reported to improve the uncommon symptoms and clinical findings (e.g., pain and maximal mouth opening) of TMJ arthritis4,5,6,7,8. Early reports have shown resolution of joint effusion following CSI by MRI4,5, while a report also mentions resolution of contrast enhancement7. Our results confirm that CSI can decrease inflammatory activity in arthritic TMJ shown as reduction in the degree and extension of bone marrow edema, synovial hyperplasia, and contrast enhancement on MRI. In addition, we demonstrate that injection of the corticosteroid into the joint space has a stronger effect than injection into the periarticular soft tissues. Following intraarticular CSI, the grade of inflammatory activity improved significantly more often than following extraarticular CSI (53% in intraarticular CSI compared to 20% in extraarticular CSI).
In our patients, repetitive CSI could not improve the degree of osseous deformity of the TMJ. On the contrary, we observed progressive deformity of the mandibular condyle and temporal bone in 41% of the investigated TMJ. Similar worsening osseous changes have also been noted by Ringold, et al in 10 out of 15 children imaged with computed tomography following intraarticular CSI6.
Arvidsson, et al have observed comparable progression of osseous deformities in 60 children (mean age at baseline 8.6 ± 2.9 yrs) with JIA who had not been treated with repetitive CSI, showing radiographic condylar and temporal bone abnormalities in 42% of patients (about 34% of TMJ) at baseline and in 65% of patients (about 60% of TMJ) at a 4-year followup examination19. Compared to this older cohort (on average 3 yrs), the grades of osseous deformity in our patients tended to be lower at baseline but higher after a mean followup of 5 years. While this might be due to more severe inflammation in our selected patient group, it might also indicate that repetitive CSI accelerates the progression of osseous deformities of the TMJ. Although in our study TMJ with progressive deformities and the 26% of TMJ with complete destruction of the mandibular condyle had received significantly higher intraarticular amounts of corticosteroid than the others, we cannot be sure whether progression of osseous deformity was due to CSI or inflammation, because these TMJ also had more inflammatory activity leading to repetition of the CSI. However, the high rate (21%) of intraarticular calcifications and heterotopic ossifications observed in our patients may be related to the high intraarticular corticosteroid doses applied. Similar severe condylar destruction with intraarticular ossifications of TMJ have been described following high-dose CSI in adults without arthritis20 and in a series of 12 children with JIA21, but not in cross-sectional or longterm radiographic studies of TMJ in children with JIA not treated with repetitive CSI13,19,22,23,24.
In our patient cohort, repetitive CSI was not able to restore normal growth of the mandibular ramus in the vast majority of inflamed TMJ, with the mean longterm growth rate over 5 years being significantly lower than normal (Figure 4). Normal short-term growth rates were observed initially in 7 TMJ without inflammation or CSI and in inflamed TMJ with extraarticular CSI, but not after intraarticular CSI. Following intraarticular application of the corticosteroids, mandibular ramus height even decreased and on average did not reach the initial height after a mean followup of 1 year. This supports the concern that intraarticular CSI may result in even more pronounced mandibular growth reduction than that caused by arthritis alone, which has been raised previously by Stoustrup, et al based on data from their experimental rabbit studies25,26. Systemic or intraarticular corticosteroid application has a direct adverse effect on bone cells and mineralization, which can result in osteonecrosis27. Decline in bone strength and collapse of the condyle could explain the mandibular ramus height reduction observed in our patients following the intraarticular CSI. Endochondral growth may also be impaired by prolonged, direct negative effects of repeated CSI on chondrocyte proliferation, collagen matrix synthesis, and mineralization28.
The main limitations of our study are its retrospective nature, which did not allow us to control for the injected corticosteroid dose, and the lack of a control group of patients not treated with CSI. However, comparison of TMJ with intraarticular and extraarticular location of the injected corticosteroid did allow demonstrating the effect of intraarticular corticosteroid on inflammatory activity and short-term growth. Further prospective studies comparing intraarticular injections with different doses of corticosteroids and placebo would be needed for better discriminating the effects of arthritis itself and corticosteroid on growth impairment of the mandibular ramus.
Comparing different events of CSI to the same TMJ and studying both TMJ of a patient pose a potential bias to our results on improvement of inflammatory activity and short-term growth following extra- and intraarticular CSI. Although inflammatory activity and growth of the TMJ may be influenced by the disease status of the contralateral TMJ, we consider the effects of the intraarticularly applied corticosteroid to outweigh those related to the contralateral joint.
Even though we did not find any significant differences in patient age between extraarticular and intraarticular CSI, between grades of inflammation and deformity at the first CSI, between TMJ with progression of deformities and without, or between TMJ with low and high growth rates, we cannot be sure whether our relatively young cohort was more susceptible to effects of inflammation and corticosteroids than an older group would be. Further studies are required to answer this question and to investigate whether a single CSI combined with systemic medication can prevent progressive deformation of the TMJ and normalize growth of the mandibular ramus.
Another limitation is the measurement error of the mandibular ramus height, which does not allow measuring short-term growth accurately in a single patient. According to Markic, et al14, MRI measurements of the mandibular ramus height can be performed with a mean difference of 0.2 mm (95% limits of agreement −2.4–2.9 mm). With a mean normal growth rate of 1.6 mm/yr (range 0.7–2.6 mm/yr)17,18, short-term growth rates over 3 months may show a mean measurement error of up to ± 50%, whereas for longterm growth rates over 5 years the mean measurement error is estimated at ± 5%. This error may be substantially higher for measuring the growth rate of a single joint, but should be canceled out when comparing the mean growth rates of groups of joints, as done in the current work.
The comparison of growth rates obtained from MRI measurements with normal growth rates from radiographic data may be a limitation to our study, but we do not expect the growth rates assessed by MRI to be significantly different from growth rates obtained by radiography. Even though mandibular ramus height measurements on lateral cephalograms show a mean difference of −2.5 mm compared to MRI measurements14, this 6% error (2.5 mm/40 mm ramus height) would result in an error of only −0.01 mm/yr for a mean growth rate of 1.6 mm/yr. This is corroborated by the fact that the short-term growth rates of the few initially untreated TMJ were not significantly different from the radiographic normal data.
In children with JIA, repetitive CSI to inflamed TMJ does not prevent progressive osseous deformity of the mandibular condyle and cannot restore normal growth of the mandibular ramus. Repetitive intraarticular application of corticosteroid may result in even more pronounced destruction and growth reduction of the mandibular condyle than that caused by arthritis alone. Because the goal of treatment was not reached in our patients, we have now discontinued the use of CSI on the TMJ treated at our institution.
ONLINE SUPPLEMENT
Supplementary data for this article are available online at jrheum.org.
- Accepted for publication March 24, 2015.








{kind=link}
{kind=link}
{kind=link}
{kind=link}