

Abstract
Objective. To assess the effectiveness of total contact insoles (TCI) in patients with plantar fasciitis (PF).
Methods. A double-blind randomized controlled trial was carried out with intention-to-treat analysis. Seventy-four patients were randomly allocated to use a TCI made of ethylene vinyl acetate (study group, n = 37) or a flat insole (control group, n = 37). The following assessment tools were used: visual analog scale for pain while walking and at rest, Medical Outcomes Study Short Form-36 (SF-36) for quality of life, Foot Function Index and Foot Health Status Questionnaire for foot function, 6-min walk test (6MWT), and baropodometer FootWalk Pro for plantar pressure analysis. The groups were evaluated by a blinded assessor at baseline and after 45, 90, and 180 days.
Results. The groups were homogeneous for the majority of variables at baseline. The over-time comparisons show a statistical difference between the groups for pain while walking (p = 0.008) and the 6MWT (p = 0.010). Both groups showed significant improvements in pain at rest, foot function, and some quality of life variables (physical functioning, bodily pain, vitality, and social functioning), with no significant statistical differences between them. The baropodometer recorded no changes from the use of the insoles.
Conclusion. A TCI can be used to reduce pain while walking and to increase walking distance in individuals with PF.
Plantar fasciitis (PF) is an inflammation of the plantar fascia1. It is characterized by pain and stiffness in the heel and medial arch of the foot, and can affect daily activities2. The most common symptoms are pain and stiffness with an insidious onset, especially during the first steps when rising in the morning2. The symptoms vary in intensity and may improve after a few steps or within a few hours, but often increase as the day progresses2.
The diagnosis of PF is essentially clinical and based on a history of pain and pain upon palpation of the fascia2,3. Diagnostic imaging may be used to exclude other causes of pain: radiographic examinations may identify heel spurs (found in 27% of cases), and ultrasound examinations of symptomatic patients reveal thickened fascia and inflammation3.
PF is often self-limited. It responds well to conservative treatment and treatment results are favorable in most cases1. Conservative treatments are generally recommended before consideration is given to any invasive treatment1.
Insoles are commonly prescribed for the treatment of musculoskeletal disorders of the lower limbs. Studies addressing patient satisfaction with insoles have shown an improvement in symptoms4. However, only a few randomized controlled trials (RCT) have been performed to assess the clinical effectiveness of insole use for the treatment of PF5.
In a study assessing the use of insoles and taping to treat PF, the insole was more effective for pain relief than the viscoelastic heel cup or a combination of oral medication and anticorticosteroid injections6. However, the study was not blind and did not describe the type of insole used.
A metaanalysis of the effect of insoles on pain and foot function for patients with PF concluded that insoles led to improvements in pain and function in the short-, medium-, and long term7. However, both the insoles used and the control groups in the studies were heterogeneous. As a result, the author recommended better-designed future studies.
A total contact insole (TCI) is a custom-made foot device that redistributes a person’s weight uniformly across the entire sole of the foot. The design is unique to each individual and is based on a model of the patient’s foot. This type of insole is recommended for patients with PF, although there is no scientific evidence to support its use8.
An RCT comparing a TCI, a prefabricated insole, and a placebo insole in patients with PF concluded that the TCI and prefabricated insoles provided a small short-term benefit. There was no statistically significant difference among the insoles9. However, the study had methodological limitations: only the patients were blinded (allowing the possibility of investigator bias) and the TCI insole was rigid, which could have hampered comfort and impact absorption.
There is little scientific evidence for the benefits of a TCI for the treatment of PF. The studies all demonstrated flawed methodology, such as not describing how the insoles were made, not using a blinded assessor, inadequate randomization, comparisons of interventions with no scientific evidence, and not having a control group.
The aim of our present study was to assess the effectiveness of a TCI on pain, function, distribution of load in the plantar region, gait variables, quality of life, and satisfaction in patients with PF.
MATERIALS AND METHODS
Study design and patients
A double-blind RCT with a 6-month followup period was carried out. Seventy-four participants were selected from the outpatient clinic. The inclusion criteria were a clinical diagnosis of PF, foot pain ranging from 3 cm to 8 cm on a 0 cm to 10 cm numeric rating scale, age of 18 years or older, and an agreement to participate. The exclusion criteria were other symptomatic musculoskeletal conditions of the lower limbs, symptomatic disease of the central or peripheral nervous system, diabetes mellitus, rigid foot deformity, insole use in the previous 3 months, physical therapy in the previous 3 months, injection in the foot or ankle in the previous 3 months, history of lower limb surgery or lower limb surgery scheduled in the upcoming 12 months, allergy to the insole material, mental disability, and unavailability to attend the evaluation visits.
Our study received approval from the ethics committee of the Universidade Federal de Sao Paulo, Brazil, and all patients provided informed consent. A computer-generated randomization list with a 1:1 ratio created by a statistician not involved in the trial was used to allocate patients randomly to the study group (SG) or the control group (CG). Blinded randomization was performed using opaque-sealed envelopes, and an independent researcher not involved in the eligibility assessment, outcome assessment, or treatment kept the assignment scheme in a locked cupboard in a central location. The assignment scheme was revealed to the treating physiotherapist after the baseline evaluation. This trial is registered on ClinicalTrials.gov (NCT01549678) and this manuscript was prepared according to the Consolidated Standards of Reporting Trials (CONSORT) statement.
Intervention
An ethylene vinyl acetate (EVA; thickness 5 mm, hardness 35 ± 5 Shore-A, density 0.160 g/cm2) TCI was used. All patients were positioned in ventral decubitus with the knee and ankle at 90° of flexion (Figure 1A) to achieve the physiological plantar arch of the patient. A plaster mesh was placed on the plantar surface of the foot to produce a negative cast. Plaster was then placed on the negative cast to produce a positive cast from which the insole was custom-made with ethylene vinyl acetate (EVA; Figure 1B). The TCI for the CG were locked in a cupboard by the primary researcher.

A. Patients positioned in ventral decubitus with knee and ankle at 90° of flexion, and a plaster mesh placed on plantar surface, making the negative cast. B. Positive plaster cast with the EVA mold. C. Lower and upper views of the TCI. D. Placebo insole. EVA: ethylene vinyl acetate; TCI: total contact insole.
At baseline, the SG was given a TCI (Figure 1C) and the CG was given a flat insole (Figure 1D) for day-to-day use for 6 months. On the day the insole was given to the patient, the insoles were adapted to the participant’s footwear in both groups. All the participants were instructed to contact the primary researcher by phone if they experienced discomfort with the insole. The patients in the CG only received a TCI at the end of the study. All patients were instructed to use the insole for 1 h on the first day, and then 1 additional hour per day in the first week. After that the patients were to use the insole as much as they could and no other intervention was allowed during the research. For pain relief, both groups were instructed to take 50 mg diclofenac sodium at 8-h intervals, as needed, and to record the dose of the rescue drug they took.
Clinical evaluations
The patients were evaluated by a blinded assessor at baseline (T0), and after 45 (T45), 90 (T90), and 180 (T180) days of insole use. The following assessment tools were used:
-
The visual analog scale (VAS) for pain for the assessment of pain at rest and walking, ranging from 0 cm (no pain) to 10 cm (unbearable pain)10;
-
The 6-min walk test (6MWT) for the assessment of functional capacity. The subject walked at maximum speed for 6 min along a 22-m track, and the total distance was recorded11. Participants wore insoles throughout the test;
-
The Foot Function Index (FFI) is a questionnaire assessing the effect on foot disability, divided into 3 subscales: foot pain, difficulty, and functional limitation. The score was determined using a numeric rating scale ranging from 0 cm to 10 cm, with a higher score denoting a greater effect on foot disability12;
-
The Foot Health Status Questionnaire (FHSQ) is composed of 29 items divided into 3 subscales: foot health, general state of health, and general demographic data. The total score was calculated using dedicated software and ranged from 0 to 100, with a higher score denoting better health status13;
-
The Medical Outcomes Study Short Form-36 (SF-36) generic quality of life questionnaire is composed of 36 items divided into 8 subscales: physical functioning, role-physical, bodily pain, general health, vitality, social functioning, role-emotional, and mental health. The score ranged from 0 to 100, with a higher score denoting better quality of life14;
-
The Likert scale for the assessment of patient satisfaction with their insole. The options were the following: much worse, a little worse, unchanged, a little better, and much better;
-
The rescue drug chart: patients recorded their daily use of 50 mg diclofenac sodium in a chart;
-
The Dynamic Baropodometer FootWalk Pro (AM Cube) and its 2-m track with 4 pressure plates containing 16,384 sensors was used to evaluate static and dynamic foot pressure and stabilometric and gait variables. The participants were barefoot. To measure static foot pressure, patients were instructed to stand on 1 of the pressure plates with feet parallel and at hip width for 20 s. To measure dynamic foot pressure, patients walked from 1 end of the track to the other 6 times (12 m in total). To avoid the effects of acceleration and deceleration, marks were placed on the floor at 2 m in front of and 2 m behind the track, and the participant was instructed to begin and end each length between these marks.
Statistical analysis
The sample size was calculated for repeated measures of ANOVA between 2 groups analyzed at 4 different times using the VAS for pain as the main variable. For the determination of the minimal effect of 2 cm, a 5% α error, 20% β error, and SD (σ) of 2 cm were established. The calculation determined a minimal sample size of 30 patients per group. Considering a possible loss of 20%, it was determined that each group would consist of 37 patients.
To study the homogeneity of the sample for the initial evaluation, the following tests were used: the chi-square test for categorical variables, Student t test for quantitative variables with normal distributions, and Mann-Whitney U test for quantitative variables without normal distributions. Repeated ANOVA measures with Bonferroni adjustment in the intragroup comparisons were used to assess differences in the outcomes between groups over time. An intention-to-treat analysis was performed — for patients who did not return for further evaluations, the last data collected were used in the subsequent evaluations. The SPSS 17 program (IBM SPSS) was used for the statistical analyses with the level of significance set to 5% (p < 0.05).
RESULTS
A total of 111 patients with PF were interviewed, 74 of which fulfilled the eligibility criteria and gave informed consent to participate. Patients were randomly allocated: 37 in the CG and 37 in the SG. Figure 2 shows the study flowchart. None of the patients discontinued treatment.

Flowchart. * Patients complete evaluations at T180. T0: baseline; T45: 45 days; T90: 90 days; T180: 180 days.
Table 1 shows the clinical and demographic characteristics of the study patients at baseline (T0). The groups were homogeneous for almost all of the variables; differences were observed in general health and vigor subscales of the FHSQ and in the subscale role-physical of the SF-36.
Baseline characteristics of the 2 intervention groups. Values are mean (SD) unless otherwise specified.
A statistically significant difference between the 2 groups (p = 0.008) was observed over time for pain while walking (Table 2) with a significantly greater improvement (p = 0.020) in the SG than CG at T180 (Figure 3A and 3B).
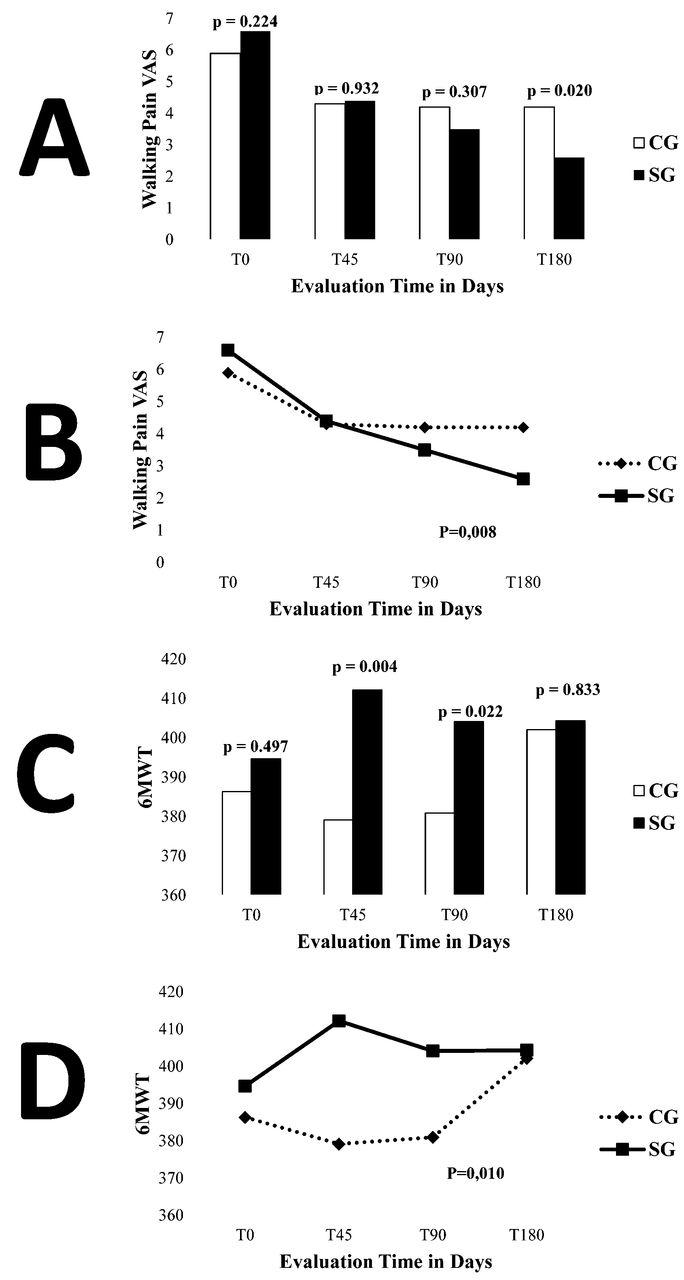
A. Comparison of groups over time for walking pain VAS. B. Comparison between groups over time for walking pain VAS. C. Comparison of groups over time for 6MWT. D. Comparison between groups over time for 6MWT. VAS: visual analog score; T0: baseline; T45: 45 days; T90: 90 days; T180: 180 days; CG: control group; SG: study group; 6MWT: 6-min walk test.
VAS at rest, walking VAS, 6MWT, FFI, FHSQ, and SF-36 measurements of the groups during 6 months. Values are mean (SD) unless otherwise specified.
Both groups showed improvement with no statistically significant difference between them for pain at rest, the foot pain, foot function, general foot health, general health, and physical activity subscales of the FHSQ; the FFI; and the physical functioning, role-physical, bodily pain, vitality, and social functioning subscales of the SF-36 (Table 2).
Regarding the walking distance (6MWT), Table 2 and Figure 3C demonstrate the statistically significant difference between groups over time (p = 0.010). Figure 3D shows that the SG had significantly better results compared to the CG at T45 (p = 0.004) and T90 (p = 0.022).
Table 3 shows the data of the plantar pressure analysis at baseline and the results of the ANOVA between the SG and CG over time. There were no differences between the 2 groups for almost all of the variables. A significant difference between the groups over time was found only in weight bearing in the right forefoot.
Static and dynamic baropodometry measurements of the 2 intervention groups during 6 months. Values are mean (SD) unless otherwise specified.
Regarding patient satisfaction with the Likert scale, no difference between groups was observed (p = 0.470 according to ANOVA). With the same statistical test in the intragroup analysis, both groups showed a significant difference in the Likert scale proportions over time (p = 0.046), whereas at T180, a larger proportion of patients chose “much better” and a small proportion of patients chose “much worse” compared to T45.
DISCUSSION
There is no consensus in the literature on the ideal type of insole for patients with PF; insoles made from a variety of materials and molding techniques have been reported15. However, there is consensus on the need for medial longitudinal arch support. A number of studies have assessed different types of insoles for the treatment of PF3,6,8,16,17,18,19,20,21,22. The TCI was chosen for the present study because we could reproduce the medial and anterior longitudinal arches of the patient’s foot without load, thereby maintaining the best physiological shape possible. We chose the ventral decubitus position to make negative casts despite it being widely debated because it creates custom-made insoles that reflect the physiological size of the arch without body load, thus giving the patient more comfortable support. The choice of EVA was based on clinical practice; this material is softer than the majority of insoles described in the literature and it has no adverse effects.
The intervention groups were homogeneous for the majority of variables at baseline, demonstrating the effectiveness of the randomization process. The mean age of about 50 years in the study population is similar to that reported in previous studies2,6,9. This age group corresponds to menopause in women that is frequently associated with weight gain, contributing to the appearance of PF23.
The mean body mass index (BMI) of the study population revealed that the patients were overweight, which is consistent with the findings of previous studies2,9. Indeed, being overweight or obese is a risk factor for PF24. A systematic review concluded that an increase in BMI was strongly associated with chronic pain in the plantar region and heel, as well as nonspecific foot pain25.
Pain while walking is the most disabling symptom for patients with PF and was therefore selected as the primary outcome in our present study7. The level of pain at baseline was similar to that reported in previous studies using a numeric rating scale2,6,16. The use of the TCI led to a statistically and clinically significant improvement of 4 points on the VAS for pain while walking. This result differs from that of previous studies comparing insole use with a placebo insole that showed no improvements in pain9,16. The lack of improvement in pain in these studies could be because of the type of insole used or methodological limitations.
The SG walked a greater distance in the 6MWT compared with baseline after 45 days, whereas the CG only walked a greater distance versus baseline after 180 days. To our knowledge, no studies in the literature have used the 6MWT or any other type of functional test to assess patients using insoles. Therefore, it is not possible to compare our results with those of other studies. The present findings suggest that the type of insole evaluated in our study improves gait performance in the initial months of use; this improvement can be considered a substantial short-term functional benefit.
The lack of improvement in pain at rest was expected because insoles only have a biomechanical effect when the individual is standing or walking. Moreover, PF has only a minor effect on function because patients are able to maintain functionality despite the pain. It is possible that the generic SF-36 questionnaire is not sensitive enough to detect the effect of PF because it is not a disabling condition in the general population.
No statistically significant differences were found between the intervention groups or between the timepoints for the majority of variables in the plantar pressure analysis. Greater static weight bearing in the right forefoot was found in the CG compared with the SG after 45 days, but the groups had similar values in the subsequent evaluations. Most studies that have performed plantar pressure analysis in patients with PF do not perform a static analysis and it is difficult to explain this result in the CG because the placebo insole does not provide any biomechanical support that would require a period of adjustment.
The plantar pressure analysis system used in our study allows for the collection of data that cannot be analyzed using a system based on sensors arranged in an insole pattern. It also allows the analysis of gait variables, such as step time, stride time, cadence, and mean velocity. Another advantage of this system is that no equipment is attached to the body, allowing for a more natural gait. While platform baropodometry is widely used in clinics, to our knowledge no studies have performed this type of plantar pressure analysis in patients with PF. However, a limitation of this type of analysis is not being able to analyze patients during insole use because they must perform the test barefoot.
The mean daily duration of insole use of 6 h is similar to that described in previous studies4,9. For this variable, no inter- or intragroup differences were found. It is likely that the patients did not use the insoles for longer periods during the day because of the tropical heat in Sao Paulo; the prolonged use of shoes may cause discomfort. No reduction in the duration of insole use was found between evaluations, which suggests that the insole material had no adverse effects. Moreover, no patients reported an increase in pain, changes in sensitivity, or skin reactions, suggesting that the insoles constitute safe treatment for patients with PF.
No differences in rescue drug intake were found in the intra- or intergroup analyses. This finding is likely because the use of medication in this population was generally low (less than half a pill per day). Moreover, no differences were found in the intra- or intergroup analyses regarding patient satisfaction with the insoles. The majority of participants reported improvements after using the insoles; this may explain why none dropped out of the study.
The purpose of our study was to compare a TCI with use of no other type of intervention. We therefore chose to use a flat insole as a sham. However, the control group showed positive results, which can be explained through the work of McCormick, et al that compared baropodometer results using only a shoe with 4 types of sham insoles, showing that the sham EVA insole had some biomechanical effect on the foot. We cannot state that the insole used in our study had the same effect as was observed in the work of McCormick, et al because they used a three-quarter insole with 3 mm of EVA while we used a full insole with 5 mm of EVA26.
The results of our study should be interpreted in light of 2 limitations. First, most patients had chronic symptoms that had persisted for an average of 1 year — the effects of the insoles may be different for patients with shorter symptom duration. Second, we did not test the bias of blinding.
Redmond, et al showed that casted and not casted insoles have similar clinical properties27. Redmond, et al provided for the first time evidence that there may be an added clinical benefit of casted TCI; however, a direct comparison between different types of devices would have been beneficial in plantar fasciitis.
Based on the present findings, a TCI can be used to diminish pain while walking and achieve a greater walking distance in patients with PF.
Footnotes
-
Supported by the Fundacao de Amparo a Pesquisa do Estado de Sao Paulo (grant #2009/54307-4) and CNPq.
- Accepted for publication January 16, 2015.








{kind=link}
{kind=link}
{kind=link}