

Rheumatoid arthritis (RA) is a clinical diagnosis, as illustrated by the probabilistic approach adopted in the 2010 American College of Rheumatology/European League Against Rheumatism (ACR/EULAR) criteria for RA, where diagnosis/classification is based on accumulating a score ≥ 0.61,2. Although that level of probability can be reached using clinical criteria only, when those are insufficient, RA-associated autoantibodies become a determining factor. Proper interpretation of the serology data thus becomes imperative to prevent circular clinical reasoning.
The 2010 RA criteria introduced 2 new serology items. First, based on their apparent very high (> 95%) specificity and positive predictive value (PPV) in early and established RA cohorts3, anticitrullinated protein antibodies (“ACPA”) have been added to rheumatoid factor (RF). Second, based on their incremental association with severity and prognosis, antibody titers in both systems, whether absent, low, or high, have been given incremental weight in the scoring system. In the final revision of the ACR/EULAR RA criteria, a detail escaped the attention of the coauthors (including me)1,2. ACPA stands for “anticitrullinated protein antibodies.” Strictly speaking, the ACPA criteria were based exclusively on the anticyclic citrullinated peptide assay (anti-CCP) literature. Hence, the ACPA acronym in the criteria should refer to anticitrullinated peptide/protein antibodies2 depending on which one is used in a particular communication. It is important to emphasize this distinction because ACPA-peptide and ACPA-protein assays overlap, like birds of the same species that can have different colors, in terms of diagnostic, prognostic, and disease monitoring value4 (Figure 1).
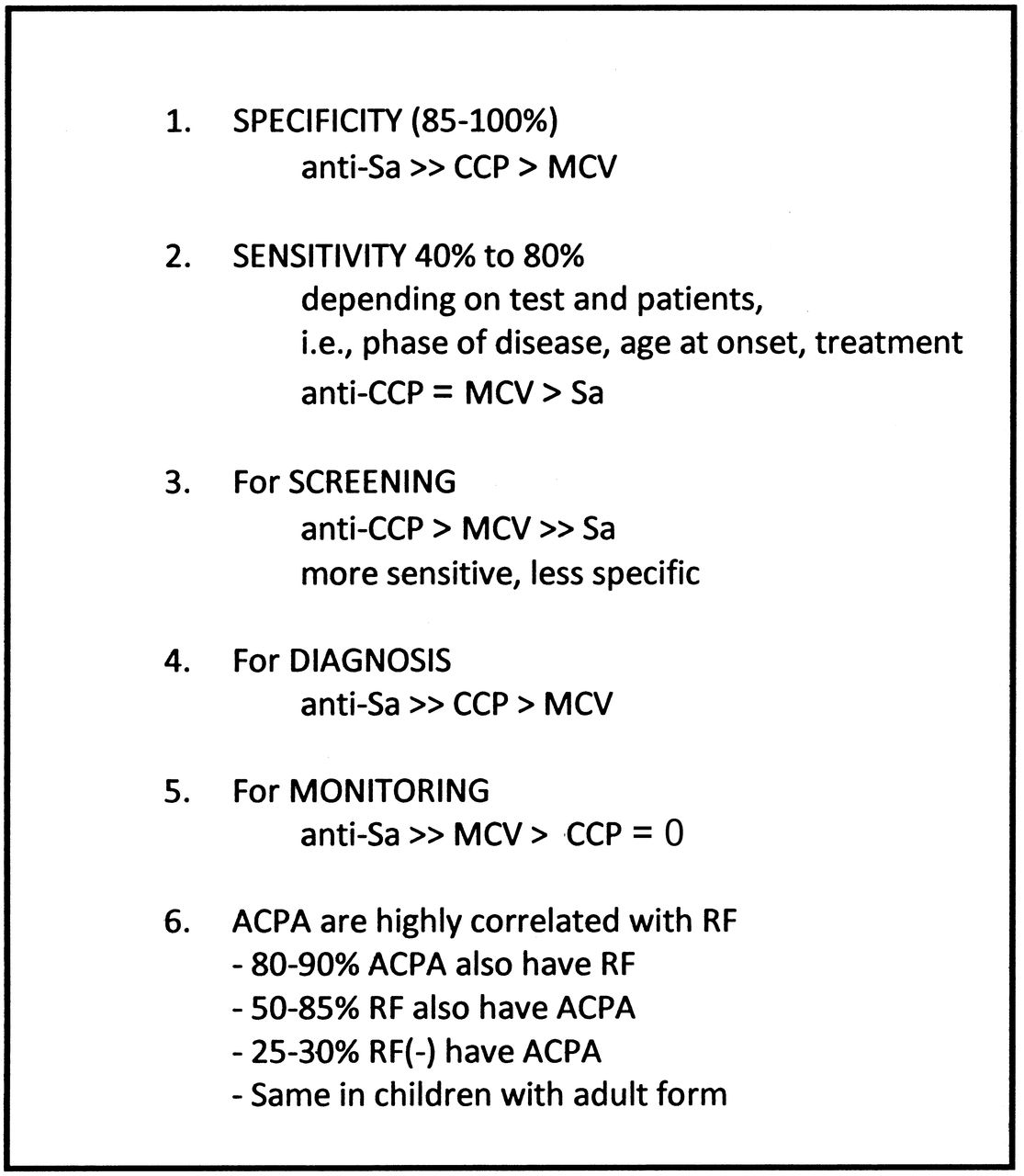
Clinical summary of ACPA literature in early and established rheumatoid arthritis. Anti-Sa ELISA (Euroimmun): anticitrullinated vimentin (target is an in vitro citrullinated native protein); anti-CCP ELISA (several companies): anticyclic citrullinated peptide (target is an in vitro synthetic peptide); anti-MCV ELISA (Orgentec): anti-mutated citrullinated vimentin (target is a multi-mutated recombinant vimentin molecule made in Escherichia coli and secondarily citrullinated in vitro). RF: rheumatoid factor.
In the current issue of The Journal5, Martin, et al share their experience as they reassess the premises of the ACR/EULAR ACPA-peptide criteria in a unique “real-world” situation. They look at patients referred to a central triage facility over 3 years (total referrals: 20,389). They identified in that database those referred specifically for a positive ACPA-peptide test (total 568 patients) and described the clinical correlations in those who were subsequently seen by a rheumatologist to clarify their diagnosis (total 314 patients). The data from their Table 1 will have to be reconciled with our current interpretation of the ACPA-peptide (anti-CCP) literature.
The first observation is that a small majority of 66.6% of those ACPA-positive patients had, as expected, RA, early RA, or possible RA, giving a PPV of 74.3%. That number was computed from people with moderate to high titers. It is much lower than the > 95% PPV found in European RA cohorts using ACPA-peptide assays or in an RA cohort from Central Canada using an ACPA-protein assay based on anti-Sa/anticitrullinated vimentin (anti-Sa/cit-vimentin) to confirm the ACPA peptide4,6.
The second observation is that 33.6% of ACPA peptide–positive patients do not have RA. They have either another rheumatic disease or no autoimmune-inflammatory disease at all. In a prospectively studied cohort of Native North Americans from the Canadian Western provinces, ACPA-peptide positivity was present in 80% of patients with RA, was frequently found in up to 20% of healthy first-degree relatives, and in up to 10% of a healthy unrelated control general population7. The average titers are slightly higher in RA but with extensive overlap between the 3 groups. In the same study, ACPA-protein testing using anti-Sa/cit-vimentin is positive in only 50% of patients with RA, and never in relatives or healthy people. Looking at the anti-CCP immunoglobulin isotype usage in each group, those without anti-Sa are all comparable. The anti-Sa positive RA subgroup is twice as active immunologically and more severe clinically even if they have the same mean anti-CCP titers. In fact, the anti-Sa negative RA patients have anti-CCP immune features resembling those of the healthy relatives and unrelated controls with anti-CCP7. The presence of positive ACPA-peptide and ACPA-mutated cit-vimentin (MCV; which behave like multiple artificial peptides stuck on a vimentin backbone) has been confirmed around the world in 10–15% first-degree relatives of RA patients in Europe (Sweden) and Asia (Korea) and in 5–7% of their general population. An ACPA real-protein test has yet to be performed in those countries and has been shown to be negative.
ACPA-peptide is mostly useful as a screening test. Like antinuclear antibodies in systemic lupus erythematosus, ACPA-peptide is more sensitive but not as specific as we were led to believe. In fact, the bottom line seems to be that ACPA-peptide testing is most useful for its negative predictive value. If negative, it is very unlikely to be RA. If positive, one would be well advised to continue relying on RF, and where possible, request an ACPA-protein test such as the anti-Sa/cit-vimentin ELISA to first confirm the diagnosis (PPV of 99% under all circumstances) and to separate out, on an individual basis, from patients with high titer ACPA-peptide, those with really bad RA prognosis8.
The third observation is that patients without RA represent 22.1% of the moderate-titer to high-titer ACPA-peptide patients. Those titers should predict soon-to-appear RA (in pre-RA) and more severe disease (in established RA), i.e., bad functional and structural prognosis. Whether those people will ever develop RA remains to be seen: that is the followup task that awaits our Calgary colleagues. As it stands, patients with high ACPA-peptide titer form a heterogeneous group, and if a high titer status is more likely to confirm diagnosis of RA, it is very risky to take population-based data interpretation at face value, as is currently done, to perform severity stratification in drug trials. Similarly, good medicine requires the appropriate use of the best tests available to establish diagnosis, inform on prognosis, and perform immune monitoring. RA being polygenic and multifactorial, the emerging biomarkers (whether genetic, serological, biochemical, clinical, or radiological) are all linked, exerting confounding influences on outcomes. The ACPA contribution to the road map toward personalized medicine in RA is to use ACPA-peptide (anti-CCP, anti-MCV, or other peptide-based assays) for first-line screening, and if positive, use ACPA-protein (anti-Sa/cit-vimentin) as second line, to either confirm diagnosis or properly establish prognosis. Positive anti-Sa means more extensive anti-CCP Ig isotype usage7, is essentially made of IgG as is an antigen-driven response6, and features extensive epitope spreading. Anti-Sa target a locally produced antigen6 and act systemically in RA vasculitis9. They have been shown to be closely associated with the worse clinical scenario4,8. Further, as pathogenic antibodies should, they vary with disease activity and can be made to disappear with treatment8,9.








{kind=link}