

Abstract
Objective. Pulmonary infections (PI) are leading causes of death in patients with connective tissue diseases (CTD). The PREVENT study (Pulmonary infections in patients REceiving immunosuppressiVE treatmeNT for CTD) assessed risk of PI in patients with active CTD in the contemporary era of advanced immunosuppressive therapy.
Methods. In patients who started corticosteroids (n = 763), conventional immunosuppressants or biologics for active CTD were enrolled. Clinical and laboratory data, usage of drugs, and occurrence of PI were collected for 12 months. Baseline risk factors were investigated using Cox regression analysis. A nested case-control (NCC) study was performed with 1:2 matched case-control pairs to assess the risk for each drug category.
Results. During the observation period, 32 patients died (4.2%) and 66 patients were lost to followup (8.6%). Patients with PI (n = 61, 8%) had a significantly worse accumulated survival rate than patients without (p < 0.01). Cox hazard regression analysis using baseline data showed that these factors were significantly associated with PI: age ≥ 65 years (HR 3.87, 95% CI 2.22–6.74), ≥ 20 pack-years of smoking (2.63, 1.37–5.04), higher serum creatinine level (1.21, 1.05–1.41 per 1.0 mg/dl increase), and maximum prednisolone (PSL) dose during the first 2 weeks of treatment (2.81, 1.35–5.86 per 1.0 mg/kg/day increase). Logistic regression analysis by an NCC study revealed that maximum PSL dose within 14 days before PI (OR 4.82, 95% CI 1.36–17.01 per 1.0 mg/dl increase; 2.57, 1.28–5.16 if ≥ 0.5 mg/kg/day) was significantly associated with the events, while other immunosuppressants were not.
Conclusion. Physicians should be aware of the higher risks for corticosteroids of PI than other immunosuppressants and assess these risk factors before immunosuppressive treatment, to prevent PI.
Treatment of connective tissue diseases (CTD) has advanced with the introduction of molecular-targeted therapies, such as biologics and new classes of immunosuppressants1,2,3,4. Corticosteroids, still indispensable for the treatment of CTD, as well as most of the new treatments have the potential to increase susceptibility to infection, and risk of infection should be compared across these medications within a single cohort. Among all infections, pulmonary infections (PI) are the most common and one of the leading causes of death in patients with CTD5,6,7,8,9; therefore prevention of PI is crucial for physicians treating these diseases.
To our knowledge, no authors have previously assessed specific risk factors for PI in patients with CTD, except for some reports from the rheumatoid arthritis (RA) population10,11,12. Assessment of risks of infection in patients with CTD is quite complicated and difficult to study because of the relatively low prevalence of the diseases and changes in immunosuppressive treatments over time. Only a few studies conducted in a population of single CTD cohorts have tried to resolve this clinical question9,13,14,15. However, many of the previous studies were retrospective in nature and did not include an adequate number of patients or infectious events for multivariate analyses. Results from single CTD cohorts cannot be generalized or applied to patients who receive similar immunosuppressive treatment for different CTD. It is also important to enroll patients with active-phase CTD when the immunosuppressive treatment starts or intensifies, and when the patients will be expected to be at the highest risk of PI. To overcome these restrictions, we conducted a large-scale, multicenter, prospective observational study (Pulmonary infections in patients REceiving immunosuppressiVE treatmeNT for CTD; PREVENT) and recruited patients with a variety of active CTD to identify risk factors for PI common to these patients.
In our study, we investigated incidence and characteristics of PI and risk factors for these life-threatening complications in patients receiving immunosuppressive treatments for active CTD, to establish milestone evidence and to ensure the safety of patients with CTD.
MATERIALS AND METHODS
Patients
Patients were eligible for enrollment in our study if they were admitted to participating hospitals for treatment of new-onset or relapsed CTD and if their attending physicians started 1 or a combination of the following 4 immunosuppressive treatments: (1) prednisolone (PSL) or other corticosteroids, (2) methylprednisolone (mPSL) pulse therapy, (3) conventional immunosuppressants, or (4) biologics. Patients who were receiving or had received immunosuppressive treatments were also eligible if they started any of the 4 treatments or increased the dose of corticosteroids or conventional immunosuppressants. Types of CTD and immunosuppressive treatments eligible for enrollment are summarized in Supplementary Table 1 (available online at jrheum.org). Ten university hospitals and 5 referring hospitals in Japan participated in our study and patients were enrolled from June 2008 to December 2010. This study was approved by the ethics committee of the Tokyo Medical and Dental University Hospital (TMDU) and those of the participating institutions. Written informed consent was obtained from each patient.
Data collection
We collected a predefined case report form at baseline, Month 6, and Month 12 after enrollment. We also collected demographic data and clinical data for CTD at baseline, data for candidate risk factors for PI at baseline and Month 6, and types and doses of administered medication and clinical course of CTD throughout the observation period. Candidate risk factors for PI were selected based on previous reports16,17,18,19,20,21,22 conducted in both general populations and patients with CTD10,11, and are summarized in Table 1. When patients developed PI, clinical, laboratory, and imaging data were collected to validate diagnoses of PI by the event-monitoring committee. All data were submitted by the site investigators to the PREVENT Data Center at the Department of Pharmacovigilance of TMDU. Two authors (HY and RS) visited 4 institutions for source data validation after all data were collected. These institutions contributed 55.5% of the total enrollment of our study. Minor errors were found in 2.0% of the data collected; all data were corrected before finalizing the database and performing analyses.
Baseline characteristics of patients from the PREVENT cohorta. Values are mean ± SD or % unless otherwise specified.
Definition of PI.
PI of interest were defined at the beginning of our study to include bacterial, atypical, Pneumocystis jirovecii, cytomegalovirus, and mycotic pneumonias; pulmonary tuberculosis (TB), pleuritis, lung abscess, and other clinically important PI reported by site investigators. The validity of the diagnosis for PI was assessed by the event-monitoring committee consisting of 2 rheumatologists (RK and MH), a pulmonologist (YM), and an infection specialist (RK). The event-monitoring committee scrutinized all data of PI cases reported, and patients were accepted as having PI only when the committee confirmed the diagnosis of site investigators. The diagnosis of PI was made by the presence of new infiltrates, consolidation, ground-glass opacity, or effusion seen using chest radiography or computed tomography, along with suggestive clinical features and laboratory findings. The results of bacterial cultures of blood or sputum were also used for the diagnosis of PI, if detected.
Statistical analysis
The primary objective of our study was to identify risk factors using multivariate analyses for the development of PI in patients with CTD given immunosuppressive treatment. We expected to identify 5 or 6 significant risk factors, requiring at least 50 cases with PI to perform multivariate analyses with appropriate statistical power. Based on our unpublished data, we assumed that 7% of the enrolled patients would develop PI and that 5% of the patients would be lost to followup by Month 12. The targeted number of patients enrolled was therefore set at 750.
The start of the observation period was the date when 1 of the 4 categories of immunosuppressive treatments began (Supplementary Table 1, available online at jrheum.org). Observation ended either 12 months later, or on the day a patient died or was lost to followup, whichever came first. We identified independent risk factors for the development of PI, first by comparing baseline characteristics of the patients with and without PI using univariate analyses. Second, we performed multivariate Cox regression analyses to identify risk factors among baseline data for the development of PI. Third, because drugs and doses of immunosuppressive treatments substantially changed over time, we then used a nested case-control (NCC) study to assess the risk of each category of medication for the development of PI more precisely.
The chi-square test for categorical variables and the Student t test or Mann-Whitney U test for continuous variables were used for comparisons between groups. Missing categorical variables constituted only 0.08% of all categorical variables. Missing continuous variable values, 1.4% of all continuous variables, were substituted with the mean value of the corresponding variables. Variables included in the Cox regression model were chosen based on the results of the age- and sex-adjusted HR and 95% CI of each variable for the development of PI. Collinearity and medical significance of the variables were also considered for selection.
In the NCC study, we used a risk-set sampling design to select control patients. For each patient who developed PI (the case group), 2 age-matched (± 1 yr), sex-matched, and disease classification–matched patients who had not developed PI during the same length of observation periods were randomly selected as the control group. For this matching, CTD listed in Supplementary Table 1 (available online at jrheum.org) were classified into articular RA (i.e., RA treated for active arthritis with no active extraarticular involvement) or others (i.e., other CTD or RA treated for extraarticular involvement) because patients with articular RA used fewer corticosteroids and more biologics compared to others (mean ± SD PSL dose: 0.07 ± 0.08 vs 0.84 ± 0.31 mg/kg/day, use of biologics: 82.5% vs. 3.2%, observed during the first 14 days of immunosuppressive therapy). The observation period for the NCC study of a matched pair was defined using the length from the start of immunosuppressive treatment to onset of a PI. We assessed the risk of medications that were administered during the 14 days at the end of the observation period for the NCC study using univariate and multivariate logistic regression analyses. SPSS was used (version 18.0, SPSS Inc.). All p values were 2-tailed and p < 0.05 was considered statistically significant.
RESULTS
Patient disposition
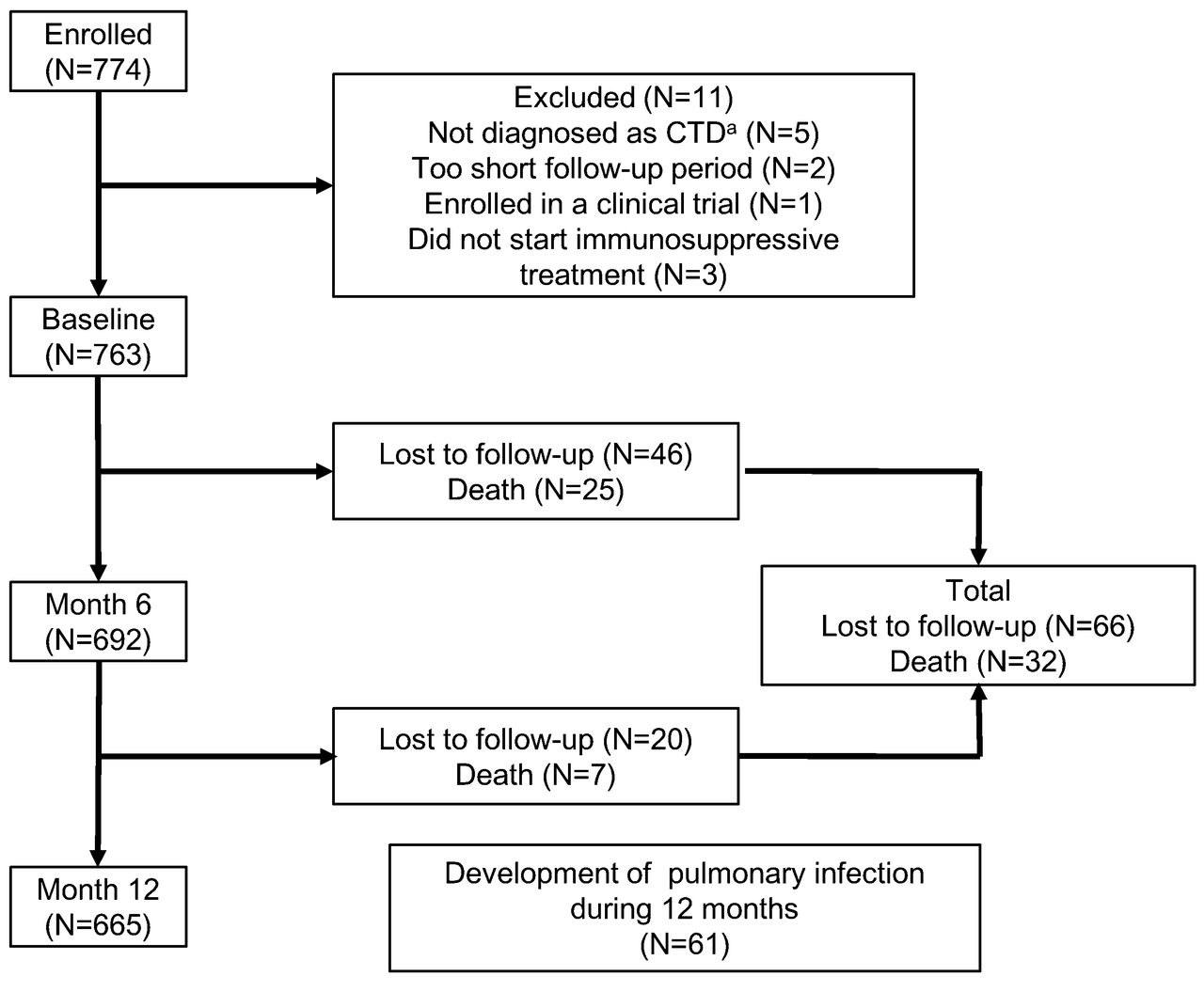
Among 774 enrolled patients, 11 were excluded and baseline data were acquired from 763 (Figure 1). Sixty-six patients were lost during the followup and 32 patients died by Month 12. The mean ± SD and median observation periods of all patients were 334 ± 86 and 365 days; for those lost to followup, 136 ± 105 and 124 days; and for those who died were 114 ± 87 and 97 days. PI were reported by site investigators in 81 patients. Among these, the event-monitoring committee confirmed 61 infections after thorough reviews of the data.

Patient disposition of the PREVENT cohort. Of the 774 patients who were registered in the PREVENT for CTD cohort, baseline data were acquired for 763 patients. Sixty-six patients were lost to followup and 32 patients died by Month 12; the remaining 665 patients completed 12 months of observation. Sixty-one patients developed pulmonary infection confirmed by the event-monitoring committee. aCTD denotes connective tissue disease. PREVENT: Pulmonary infections in patients REceiving immunosuppressiVE treatmeNT for CTD.
Baseline characteristics of the patients
Baseline characteristics of patients who developed PI (infection group, n = 61) and those who did not (noninfection group, n = 702) are summarized in Table 1. The infection group was older and had fewer women, higher rates of incident use of immunosuppressive treatment, more patients with ≥ 20 pack-years of smoking, more resolved serious infections within the 6 months prior to enrollment, and poorer Eastern Cooperative Oncology Group performance status (ECOG PS ≥ 3) than the noninfection group. Also observed in the infection group was higher prevalence of diabetes mellitus, previous pulmonary TB, interstitial pneumonia, and chronic obstructive pulmonary disease. Diagnoses of vasculitis and polymyositis/dermatomyositis were associated with the infection group. The infection group had higher mean serum creatinine and lower serum albumin levels, while other laboratory data did not differ significantly (Supplementary Table 2, available online at jrheum.org). The infection group was given a higher maximum PSL dose and used fewer conventional immunosuppressants during the first 14 days of their immunosuppressive treatment. The use of each conventional immunosuppressant and biologic during the first 14 days and for the whole observation period is shown in Supplementary Table 3 (available online at jrheum.org). P values were not corrected for multiple comparisons.
Development and prognosis of PI
Development of PI was more conspicuous within 3 months after the initiation of the immunosuppressive treatment. Thirty-three patients (54.1%) developed PI by Month 3 (Supplementary Figure 1, available online at jrheum.org). Percentages of each PI are summarized in Table 2. Twenty-five patients developed bacterial pneumonia and 20 developed P. jirovecii pneumonia (PCP), which accounted for 41.0% and 32.8% of total PI, respectively. Of the 20 patients who developed PCP, only 3 had prophylaxis for PCP with monthly aerosolized pentamidine. Opportunistic infections, including PCP, mycotic pneumonia, cytomegalovirus pneumonia, and pulmonary TB were reported in 34 of the 763 patients (4.5%). Three patients who developed pulmonary TB did not show evidence of previous pulmonary TB on chest radiographs at baseline and did not receive chemoprophylaxis, while 105 patients who received chemoprophylaxis did not develop pulmonary TB.
Types of pulmonary infections (PI)*.
Vital prognosis
Thirty-two patients died during the observation period; the causes of their deaths are summarized in Table 3. Causes of death were confirmed using case report forms, additional information provided by site investigators, and discharge summaries. Among the 32 patients who died, 8 patients developed PI and 3 died of pneumonia. Among the remaining 5 other patients who developed PI, 4 patients died of exacerbation of interstitial pneumonia and 1 patient died of sepsis. All of these 5 patients died subsequently to PI during the same admission, except for 1 patient who died of exacerbation of interstitial pneumonia. In the noninfection group, 24 patients died. Exacerbation of interstitial pneumonia was the most frequently reported cause of death (n = 10) in the noninfection group. Age-adjusted and sex-adjusted HR of PI for death using Cox regression analysis was significantly elevated (HR 5.25, 95% CI 2.23–12.35).
Causes of death*.
Independent risk factors for PI
We constructed Cox regression models to identify risk factors for PI. We initially calculated the age-adjusted and sex-adjusted HR for each variable for the development of PI (Table 1). Lower ends of 95% CI of HR were higher than 1.0 for age ≥ 65 years, incident use of immunosuppressive therapy, ≥ 20 pack-years of smoking, ECOG PS ≥ 3, serum creatinine levels, maximum PSL dose, use of PSL > 0.5 mg/kg/day, and use of mPSL pulse therapy during the first 14 days of immunosuppressive treatment. We subsequently included these variables and sex in the final Cox regression model (Table 4). Age ≥ 65 years (HR 3.87, 95% CI 2.22–6.74), ≥ 20 pack-years of smoking (2.63, 1.37–5.04), serum creatinine (1.21, 1.05–1.41, per 1.0 mg/dl increase), and maximum PSL dose during the first 14 days of the immunosuppressive treatment (2.81, 1.35–5.86, per 1.0 mg/kg/day increase) were significantly associated with PI. Other statistical models that included use of conventional immunosuppressants and biologics during the first 14 days of immunosuppressive treatment or CTD diagnosis showed essentially the same results (data not shown).
Multivariate analysis of independent risk factors for pulmonary infections (PI) in the PREVENT cohorta.
NCC study to identify the risk of medication on the development of PI
Because 45.9% of the PI developed at or after Month 4 of the observation period (Supplementary Figure 1) and immunosuppressive treatments changed substantially during the observation period in each patient, prediction of PI using baseline medications may not be sufficient. To overcome this, we implemented an NCC study to cautiously and precisely evaluate the association of treatment with PI. Among 61 patients in the infection group, 1 patient failed to match with appropriate control patients. The remaining 60 patients (case group) were successfully matched with 120 patients from the noninfection group (control group). Baseline characteristics and diagnosis of CTD were not significantly different between the groups. We compared medications used during the 14 days at the end of the observation period for the NCC study of each matched pair and found that the maximum PSL dose of the case group was significantly higher than that of the control group (0.55 ± 0.30 vs 0.44 ± 0.28 mg/kg/day, p = 0.02), and the use of PSL > 0.5 mg/kg/day was more prevalent in the case group (53.3% vs 34.2%, p = 0.01; Supplementary Table 4, available online at jrheum.org). Multivariate logistic regression analysis revealed that both maximum PSL doses as a continuous variable (Model 1, OR 4.82, 95% CI 1.36–17.01, per 1.0 mg/kg/day increase) and a categorical variable (Model 2, 2.57, 1.28–5.16, ≥ 0.5 mg/kg/day) were significant risk factors for the development of PI (Table 5) after adjusting for the covariates of ≥ 20 pack-years of smoking, serum creatinine, and performance status ≥ 3. However, the use of mPSL pulse therapy, conventional immunosuppressants, and biologics was not significantly associated with PI.
Association between immunosuppressive medications and PI in the NCC studya.
DISCUSSION
To our knowledge, ours is the first large-scale, multicenter prospective cohort study that investigated PI in patients with CTD receiving immunosuppressive treatment. Here, we report incidence and types of PI, their implications for vital prognosis, and risk factors for developing PI among patients with CTD receiving immunosuppressive treatments.
The association of baseline characteristics with PI in patients with CTD described in our study is consistent with the results of previous studies conducted in general populations. Because immune function becomes impaired with aging, older age has been identified as a risk for serious infections16,17,18,19. Smoking is also a known risk factor for community-acquired pneumonia16,17,18,19,20. Reduced ciliary and respiratory epithelial functions, as well as defects in humoral and cellular immunity caused by smoking, have been suggested to explain the vulnerability of smokers for PI21,25,26. Renal impairment is associated with reduced function of both innate and adaptive immune systems27. James, et al22 reported an association of reduced glomerular filtration rates and increased risk of hospitalization and death from pneumonia, which is consistent with our results.
The most important information gained from our study is that the maximum dose of PSL clearly increased risk for PI, but the use of conventional immunosuppressants did not. We analyzed the risk of categories of medications for PI using 2 statistical methods, Cox regression analysis using baseline data in all patients and logistic regression analysis in the NCC study, and obtained the same results. For proper evaluation of the infection risk of each medication category, the NCC design appears to be more appropriate to our cohort because using the risk set sampling model enables direct comparison of medication use during the observation period between the 2 groups. The use of mPSL pulse therapy, conventional immunosuppressants, and biologics was not associated with an increased risk for PI; this contradicts the results from previous reports28,29,30,31. The use of conventional immunosuppressants has been assumed to increase the risk for infections in some studies32,33. However, there are no high-quality epidemiological data that reveal an increased risk of infection from conventional immunosuppressants in a population exposed to high doses of PSL. It is plausible that the risk of conventional immunosuppressants for PI was masked in our patient population because 65.5% of our patients received PSL ≥ 0.5 mg/kg/day at baseline and the maximum PSL dose had a high HR of 2.81. The negative result of the risk of biologics for PI may derive from treatment regimen characteristics of our cohort in which a low percentage of patients (17.7%) were exposed to biologics.
The occurrence of opportunistic infections was 4.5% in our cohort. As many as 20 patients (2.6%) developed PCP, the incidence of which in Japan has been shown to be significantly higher than in Western countries12,34,35,36. It has also been suggested that the prior experience of a hospital in treating patients with PCP is associated with a higher likelihood of diagnosis of PCP36. All participating hospitals in our cohort were referral centers with vast experience in diagnosing and treating PCP; this may be associated with the higher incidence rate of PCP in our study compared to previous reports. Although 489 patients (64.1%) received prophylaxis for PCP at some point from baseline to Month 6, none of the 20 patients at the time who developed PCP had received prophylaxis with trimethoprim-sulfamethoxazole, which is quite effective against PCP37,38. Three patients who received monthly administration of aerosolized pentamidine developed PCP, which suggested a limited prophylactic effect of the drug against PCP39,40. The unadjusted incidence rate of pulmonary TB in our cohort was 450/100,000 patient-year, which is apparently higher than that of the general Japanese population (14/100,000 patient-yr) in 2010. All 3 patients who developed pulmonary TB had not received prophylactic medication against TB. The high incidence of PCP and TB warns us to implement prophylaxis more stringently against these opportunistic infections.
In the recommendations on the management of medium- to high-dose glucocorticoid therapy in CTD by the European League Against Rheumatism41, evidence about risk management of infection was limited to those obtained from RA cohorts42,43,44,45, which suggests the lack of high-quality evidence in patient populations of other CTD. Previous studies assessing risk factors for infections in patients with CTD have deficiencies in design and methods13,14,15. For proper identification of risk factors for PI common to patients with various CTD receiving immunosuppressive treatment, an ideal study design should meet the conditions of large sample sizes, prospective study design, and appropriate observation period to include the active phase of CTD when immunosuppressive treatment starts or intensifies. Our study is the first to satisfy these methodological conditions.
Our study has several limitations. First, the different approval status of medications from Western countries should be considered when generalizing. Because of the lack of approval by the Japanese regulatory agency, few patients used mycophenolate mofetil and rituximab in our cohort. Second, we enrolled patients with “articular RA” who used less PSL and more biologics. As a sensitivity analysis, we conducted an additional multivariate analysis excluding patients with articular RA and found essentially the same risk factors (Supplementary Table 5, available online at jrheum.org).
We have shown the prevalence and types of PI during immunosuppressive treatment among patients with CTD. Significant risk factors age ≥ 65 years, ≥ 20 pack-years of smoking, and elevated serum creatinine at baseline and maximum PSL doses, both at baseline and when PI developed. To reduce the risk of PI in patients with these irreversible risk factors, investigations for novel treatment strategies with lower doses of corticosteroid are warranted. The results of our study mean that all physicians should take appropriate measures to prevent PI.
ONLINE SUPPLEMENT
Supplementary data for this article are available online at jrheum.org.
Acknowledgment
We sincerely thank all the physicians and others caring for the patients enrolled in the PREVENT study.
Appendix
List of study collaborators. Investigators of the Pulmonary infections in patients REceiving immunosuppressiVE treatmeNT for connective tissue disease (PREVENT) study group, and their affiliations: Hiromi Hagiwara, Yuichiro Fujieda (Hokkaido University); Tsutomu Takeuchi, Michito Hirakata (Keio University); Shintaro Hirata, Kazuyoshi Saito (University of Occupational and Environmental Health); Jun Kishi, Yuko Toyoda (Tokushima University); Hirofumi Amano, Naoto Tamura (Juntendo University); Kenchi Takenaka (Ome Municipal General Hospital); Koichi Amano (Saitama Medical Center); Futoshi Hagiwara (Sagamihara National Hospital); Tadashi Hosoya (Tokyo Metropolitan Geriatric Hospital); Yasuhiro Katsumata (Tokyo Women’s Medical University).
Footnotes
-
Supported by a grant-in-aid from the Ministry of Health, Labor and Welfare, Japan (H23-meneki-sitei-016 and H19-meneki-ippan-009 to N. Miyasaka), and by grants-in-aid for scientific research from the Japan Society for the Promotion of Science (#24890057 to R. Sakai, #19590530 to R. Koike, #26590171 to M. Tanaka, and #20390158 to M. Harigai).
Also supported by grants for pharmacovigilance research on biologics from Abbvie G.K., Astellas Co. Ltd., Bristol-Myers Squibb Japan, Chugai Pharmaceutical Co. Ltd., Eisai Co. Ltd., Mitsubishi Tanabe Pharma Corp., and Takeda Pharmaceutical Co. Ltd. (to M. Harigai), and by a grant from the Japanese Ministry of Education, Global Center of Excellence Program, International Research Center for Molecular Science in Tooth and Bone Diseases. TMDU received unrestricted research grants from Abbvie G.K., Astellas Co. Ltd., Bristol-Myers Squibb Japan, Chugai Pharmaceutical Co. Ltd., Eisai Co. Ltd., Mitsubishi Tanabe Pharma Corp., and Takeda Pharmaceutical Co. for the Department of Pharmacovigilance, with which TMDU paid salaries for H. Yamazaki, R. Sakai, R. Koike, M. Tanaka, T. Nanki, K. Watanabe, and M. Harigai.
- Accepted for publication December 5, 2014.








{kind=link}