

Abstract
Objective. Recent advances in the management of patients with rheumatoid arthritis (RA) increased the rates of disease remission and patient life expectancy, while malignancy has become a more common cause of death. Here, we report the incidence of malignancy in a nationwide survey of Japanese patients with RA compared to the general population, focusing on the risk of lymphoma, which often arises in patients with RA.
Methods. Data on the occurrence of malignancy were collected from patients registered in a nationwide Japanese cohort database, the National Database of Rheumatic Diseases by iR-net in Japan, from 2003 to 2012. To adjust for different population composition and to compare the incidence of malignancy with the general population, standardized incidence rates (SIR) were calculated. To identify risk factors for lymphoma, individual patient data were obtained for multivariate analysis for the year before lymphoma diagnosis.
Results. In 10 years, the cohort composed of 66,953 patient-years yielded 559 malignancies, most frequently lung cancer, followed by gastric cancer, breast cancer, and lymphoma. The overall incidence of malignancies in patients with RA was slightly lower than in the general population (SIR 0.89, 95% CI 0.82–0.97). However, lymphoma risk was significantly higher (SIR 3.43, 95% CI 2.59–4.28), whereas risk of colon, rectal, or liver cancer was lower. Significant risk factors for lymphoma were the use of methotrexate or tacrolimus, and higher age.
Conclusion. Patients with RA had no higher overall incidence of malignancies, but lymphoma was significantly more frequent than in the general population.
Rheumatoid arthritis (RA) is a chronic systemic inflammatory disease associated with autoimmune disorders. It primarily affects joints. Improvements in the management of RA have increased the remission rate1 and life expectancy of patients with RA2; however, patients with RA die mainly of cardiovascular/cerebrovascular diseases, respiratory diseases, infections, or malignancies2,3,4. With regard to cause of death, the proportion of infections and respiratory disorders associated with RA has been decreasing while malignancies are increasing2. Although the recorded incidence of malignancies differs depending on regional or racial differences among the cohorts studied, an established characterization is the increased risk of lymphoma in patients with autoimmune rheumatic diseases, including RA5. Our present study investigated the incidence of malignancy in Japanese patients with RA, focusing on risk factors for the increased occurrence of lymphoma.
MATERIALS AND METHODS
Data on patients with RA were obtained from a nationwide Japanese multi-center cohort database, the National Database of Rheumatic Diseases by iR-net in Japan registry (NinJa), from 2002 to 2012. The NinJa registry is one of the largest registries in Japan, representing about 1% of the total number of Japanese patients with RA. In brief, patients who were seen at each participating hospital that belonged to the National Hospital Organization across Japan and fulfilled the standard diagnostic criteria for RA were registered by the physicians6,7. The data on all patients have been obtained every year by means of an open prospective cohort registry, which meant that not only fixed patients were continuously followed and registered, but the accumulation of patient data collected every year was analyzed1. About 81% of the registered patients have been followed continuously in the following year during the whole observation period. Information about the occurrence of malignancy was collected by the physician’s declaration by reference to medical records or medical referral letters. The study was reviewed and approved by the research ethics committees of the National Hospital Organization and each participating hospital.
To adjust for the differences in population composition and to compare the incidence of malignancy between patients with RA and the general population, standardized incidence rates (SIR) were calculated. The SIR was the ratio of the observed number of malignancies from the cohort and the expected number in the general age-matched and sex-matched Japanese population. Data on the incidence of malignancies in the general population were obtained from the Center for Cancer Control and Information Services, National Cancer Center, Japan8. Lymphoma, mainly Hodgkin’s and non-Hodgkin’s lymphoma, corresponds to C81–85 and C96 as coded in the International Statistical Classification of Diseases and Related Health Problems, 10th ed. The 95% CI of the SIR was calculated by referring to the observed number of malignancies as a Poisson variable and its related 95% interval obtained from statistical tables. Annual SIR and 95% CI of lymphoma and overall malignancies were calculated by reference to incidence in the general Japanese population in the same year (for SIR until 2008) or in 2008 (for SIR after 2008).
To identify risk factors for the development of lymphoma, each patient’s data in the year before the onset of lymphoma (2002–2011) were used for univariate and multivariate analysis with multiple logistic regression. The data of the patient-years after the onset of lymphoma were excluded in this analysis. To select significant variables for multivariate analysis, stepwise regression through backward elimination was applied to the following variables: age, sex, RA disease duration, Steinbrocker stage score, global functional status, Disease Activity Score in 28 joints (DAS28)-erythrocyte sedimentation rate (ESR) or –C-reacting protein (CRP), and use of nonsteroidal antiinflammatory drugs (NSAID), corticosteroids, methotrexate (MTX), tacrolimus, non-tacrolimus immunosuppressants (azathioprine, mizoribine, cyclophosphamide, and cyclosporine), anti-tumor necrosis factor (TNF) biologics (including infliximab, etanercept, adalimumab, and golimumab), and non-anti-TNF biologics (including tocilizumab and abatacept). In Japan, tacrolimus is the most common immunosuppressant in patients with RA and these biologics were all those that had been approved for RA by 2012. The stage of articular destruction was classified from radiographs of the hands based on the Steinbrocker classification (Steinbrocker stage)9. Global functional status was based on the classification by the American College of Rheumatology 1991 revised criteria10.
Between-group comparisons for univariate analysis were conducted using the Wilcoxon rank sum testing (with continuity correction) for numerical values or Fisher’s exact test for proportions. Significant p values were those lower than 0.05.
RESULTS
Table 1 shows baseline characteristics of the cohort based on patient-years. Over 10 years (2003–2012), the cohort accumulated 66,953 patient-years (81.6% female patient-yrs and 18.4% male) from 45 hospitals and yielded 559 malignancies. These were found in 370 women (67%) and 179 men (33%). Nine patients had multiple malignancies simultaneously. The incidence rate of malignancies of all types in the cohort was 820 per 100,000 person-years (0.8%). Mean age and DAS28-ESR of all patients were 62.7 years and 3.63, respectively.
Baseline characteristics of the entire cohort based on patient-years. Values are % unless otherwise specified.
Differences in characteristics of patients with or without malignancy are shown in Table 2, indicating that accumulated patient-years with the onset of malignancy were greater for men (33% with malignancy vs 18% without malignancy, p < 0.0001), older patients (mean age 68.1 vs 62.7 yrs, respectively, p < 0.0001), and patients with higher age at onset of RA (mean age 54.8 vs 49.7 yrs, respectively, p < 0.0001) relative to those without malignancy.
Characteristics of patients with or without malignancy based on patient-years.
The most frequent malignancy was lung cancer (n = 89, 16% of all malignancies), followed by gastric cancer (n = 78, 14%), breast cancer (n = 66, 12%), lymphoma (n = 63, 11%), and colon cancer (n = 47, 8%). Unlike the other malignancies, patients with lymphoma had onset of RA at a younger age (median 51.6 yrs with lymphoma vs 55.2 yrs with other malignancies, p = 0.0406) and had longer RA disease duration (median 12 yrs vs 10 yrs, respectively, p = 0.0140).
The total SIR of malignancies was 0.89 overall (95% CI 0.82–0.97), a significantly lower incidence than in the general population (Table 3). Thus, the SIR for gastric cancer in women (SIR 0.69, 95% CI 0.46–0.91), colon cancer in both sexes (SIR 0.71, 95% CI 0.51–0.91), pancreatic cancer in women (SIR 0.61, 95% CI 0.25–0.97), rectal cancer in both sexes (SIR 0.59, 95% CI 0.32–0.86), cancer of the kidney or urinary tract in men (SIR 0.35, 95% CI −0.13–0.82), liver cancer in both sexes (SIR 0.33, 95% CI 0.15–0.51), and leukemia in both sexes (SIR 0.37, 95% CI −0.05–0.79) were significantly lower than in the general population. However, in both sexes, the SIR of lymphoma (SIR 3.43, 95% CI 2.59–4.28) was significantly higher.
Types (ICD-10 codes), observed and expected numbers of malignancies, and their SIR with 95% CI. No information about the incidence of breast cancer in men was provided. The other 15 malignancies recorded in women and 3 in men, including duodenal cancer and tongue cancer, are not shown.
When looking at the transition from 2003 to 2012 (Figure 1), there were changes in treatment over the years, with the use of MTX increasing from about 36.6% of all registered patients in 2003 to 62.0% in 2012. Similarly, use of biologics increased from 0.5% to 22.9% and tacrolimus from very few to 9.7%. In contrast, the use of corticosteroids decreased from 62.5% to 45.3% of patients and NSAID from 73.3% to 45.5%. Concerning disease activity of RA, the percentage of patients with DAS28-ESR less than 3.2 (corresponding to low disease activity or remission) increased from 25% to 54%.
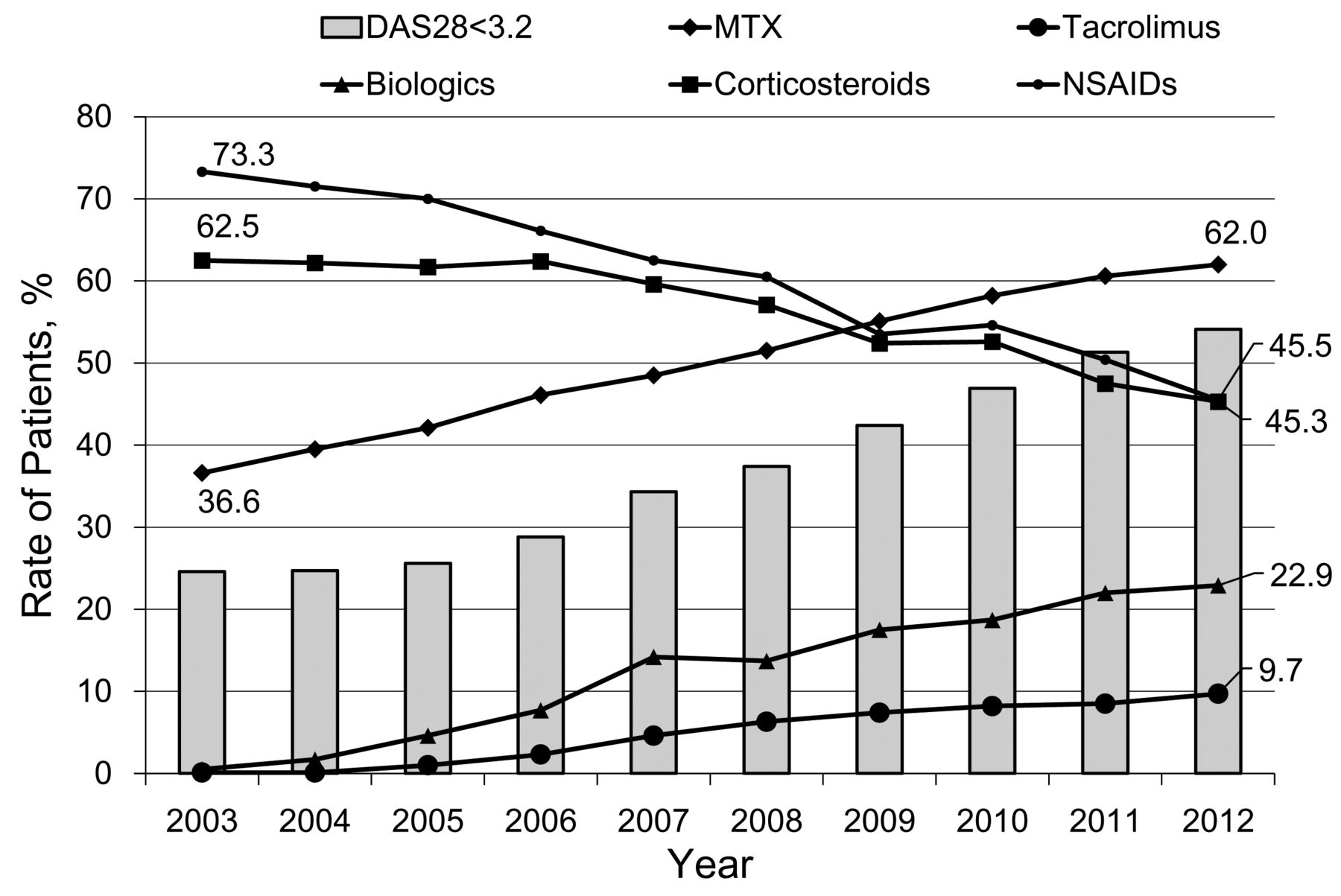
Changes in medication usage and patients with remission or low disease activity of RA. Each bar represents the annual rate of patients with disease activity score in DAS28-ESR lower than 3.2. The use rate of NSAID in 2012 was 45.5% and that of corticosteroids was 45.3%. RA: rheumatoid arthritis; DAS28: Disease Activity Score in 28 joints; ESR: erythrocyte sedimentation rate; NSAID: nonsteroidal antiinflammatory drugs; MTX: methotrexate.
Nevertheless, as shown in Figure 2, annual SIR of lymphoma and overall malignancies remained steady at about 4 and 1, respectively. There was no tendency for the annual SIR of other malignancies, such as lung, gastric, breast, colon, and rectal cancer, to either increase or decrease (data not shown).

Annual SIR and 95% CI of lymphoma (broken line) and overall malignancies (solid line). The SIR of lymphoma are stable at about 4 and those of overall malignancies at 1. SIR: standardized incidence rate.
To identify risk factors associated with the increased frequencies of lymphomas, data from individual patients in the year before lymphoma onset (2002–2011) were analyzed. First, we examined correlations between the onset of lymphoma and DAS28-ESR or -CRP at a single measurement in the preceding year, which were not significant (p = 0.8811 for DAS28-ESR or p = 0.6444 for DAS28-CRP). Second, stepwise regression was used to screen variables. In variables including background characteristics or medications, only the following variables were selected as significant for multivariate analysis: age, use of MTX, and use of tacrolimus. Third, when performing multivariable analysis, we added the following variables for clinical concern: sex and use of NSAID, corticosteroids, non-tacrolimus immunosuppressants, and any biologics (anti-TNF and non-anti-TNF). As shown in Table 4, higher age (OR 1.04 per an additional yr of age), use of MTX (OR 3.5, 95% CI 2.0–6.3), and use of tacrolimus (OR 3.9, 95% CI 1.9–7.4) were significantly associated with the onset of lymphoma in the next year. Tacrolimus was often used for patients with RA in Japan, while the other immunosuppressants were not (Table 1). Non-tacrolimus immunosuppressants (azathioprine, mizoribine, cyclophosphamide, or cyclosporine) also had high OR (6.8) but showed no statistical significance, probably because of the paucity of patients receiving them (0.5% of total patient-yrs in this analysis). Concurrent use of MTX and tacrolimus presented no additive effect for developing lymphoma (data not shown).
Risk factors for lymphoma by multivariable analysis.
We observed that 46 (73%) and 10 (16%) of 63 patients who developed lymphoma had received MTX or tacrolimus in the preceding year, respectively, while MTX or tacrolimus was used in 50% and 5% of all patient-years, respectively (p = 0.0003 for MTX and p = 0.0010 for tacrolimus). No significant correlation was found between the onset of lymphoma and the dose of MTX in the preceding year (data not shown).
DISCUSSION
Advances in the treatment and management of patients with RA have contributed not only to the reduction of their symptoms and the improvement of function and quality of life, but also to increased life expectancy. However, malignancy is emerging as one of the least tractable, unexpected, life-threatening complications during the course of RA. It is not clear whether the overall incidence of malignancies in patients with RA is higher11,12,13, lower14,15, or the same as in the general population16,17. Because the incidence of each type of malignancy differs according to regional or racial features, the overall incidence of malignancies differs from study to study. With respect to the contemporary general Japanese population, breast cancer is the most frequent malignancy in women, followed by colon, gastric, and lung cancer. In men, gastric cancer is the most common cancer, followed by lung or colon cancer8. Our 10 years’ observation of Japanese patients with RA revealed a slightly but significantly reduced overall incidence of malignancies of any type (SIR 0.89), but excess lymphoma compared with the age-matched and sex-matched Japanese population. Fewer malignancies overall resulted from reduced frequencies of several types, including colorectal and liver cancer. These results almost agree with the latest research from East Asia (Taiwan)15. Although the sample size of our cohort was not small, annual fluctuations of the numbers of different malignancies did occur. However, these had little influence on the SIR over the entire observation period. Thus, a conservative interpretation of the annual SIR for malignancies overall (Figure 2) is that their incidence in patients with RA is similar to that in the general population.
Less colorectal cancer in patients with RA has previously been reported in epidemiological studies11,13,14,15,16,18. This might be the result of using NSAID, the inhibitory effect of which on colorectal cancer was confirmed by experimental animal studies19 and metaanalysis of clinical research20. Additionally, as in a study in Taiwan (SIR 0.87, 95% CI 0.75–1.00)15, we found decreased liver cancer. The rarity of these cancers can be explained by the finding that NSAID, which were used in about 60% of all patient-years, induced apoptosis of such cancer cells by means of cyclooxygenase 2 suppression21,22. If this is so, the recent decreased use of NSAID in patients with RA could lead to increased colorectal cancer in the future; however, such a tendency is not detectable to date (data not shown).
Several reports have noted excess lung cancer in patients with RA, although not as frequently as lymphoma11,12,13,23. We also saw a tendency for increased lung cancer, but this was not statistically significant. The reasons for the difference between our results and the earlier reports cannot be determined because of the lack of information in our study about risk factors, such as smoking history and the presence of interstitial lung disease (ILD), which would be associated with the development of lung cancer.
Lymphoma, particularly non-Hodgkin’s lymphoma, is well known to develop in patients with RA. The SIR of 3.43 for lymphoma in our cohort is consistent with results of earlier studies that reported a SIR of lymphoma ranging from about 2 to 611,12,13,15,16,18. Moreover, currently, most patients with RA are treated with MTX, biologics, or disease-modifying antirheumatic drugs, all of which might contribute to the development of lymphoma. The association between RA per se and lymphoma was established by the finding that lymphoma incidence was increased in patients with RA even before MTX was approved by the US Food and Drug Administration in 198824,25,26,27. Further, a case-control study with quantitative analysis of cumulative disease activity of RA by Baecklund, et al revealed an association between disease activity and the development of lymphoma28. That analysis was critical because longterm disease activity of RA was taken into account and channeling bias was excluded. Thus, the tendency for physicians to administer potent antirheumatic drugs such as MTX and biologics to patients with severe RA who may then be at a higher risk of developing lymphoma was excluded. In our study, we found that patients who developed lymphoma had had a significantly longer RA disease duration (Table 2), supporting the existence of a relationship between RA cumulative disease activity and the development of lymphoma. On the other hand, the results of Baecklund, et al yielded no statistically significant associations between the development of lymphoma and the use of antirheumatic drugs, including MTX28. However, that could have been because of the small number of patients who received MTX (5%) in their study.
Subsequent RA case series have documented spontaneous remission of lymphoma after withdrawal of MTX, implying an association between MTX and lymphoma29. Many such cases are diffuse large B cell lymphomas positive for Epstein-Barr virus (EBV)30,31,32,33,34. Possible mechanisms for the development of EBV-related lymphoma in addition to some property of RA per se34,35 are, therefore, the reduction of the ability to prevent EBV infection by MTX36,37. In agreement with a prospective cohort study38, we showed in the present epidemiological study that MTX use was a risk factor for the development of lymphoma even after adjustment for several variables, including age, sex, and use of other antirheumatic drugs. Meanwhile, we were unable to demonstrate an association between lymphoma and RA disease activity in our study. Although DAS28 assessed at a single measurement in the year before the onset of lymphoma was taken as a measure of disease activity, this might not represent longterm disease activity as in the study of Baecklund, et al28. Given that not only MTX, but also RA disease activity alone, is associated with the development of lymphoma, the efficacy of MTX in also preventing lymphoma by reducing disease activity should be evaluated.
We did not find any significant correlations between the development of lymphoma and the use of biologics, which is consistent with previous metaanalyses39,40. No other antirheumatic drugs have been suggested to induce malignancy except for immunosuppressants, such as azathioprine23,28,41, for which the risk is difficult to ascertain because so few patients with RA are treated with them. In addition to MTX, the use of tacrolimus was significantly associated with the development of lymphoma in our multivariate analysis. Azathioprine was assumed to be a candidate lymphoma-inducer in patients with inflammatory bowel disease42 through its effects on mutation and DNA repair43. However, the risk of lymphoma development associated with oral tacrolimus in patients with autoimmune diseases has not been evaluated because this drug is approved for RA in only a few countries worldwide and insufficient data exist. Tacrolimus, a calcineurin inhibitor, is primarily used in patients with organ transplants, in whom an increased risk of lymphoma has been noted44. Our results are supported by a report of a small number of Japanese patients with autoimmune diseases who were thought to have developed tacrolimus-induced lymphoma45. It can be hypothesized that oral tacrolimus is associated with the development of lymphoma through systemic immune suppression in patients with RA for the same reason as in patients with transplants, despite the low initial dose of the drug.
Although our study demonstrated that the use of MTX or tacrolimus means a significant risk for developing lymphoma in patients with RA, the risk could be reduced by some confounding factors such as reduced RA disease activity. A characteristic of our database, NinJa, is to provide an overview as well as annual changes of all patients’ profiles, which can present data for an interpretation of the relationship. Of note, the following 3 trends were observed. First, annual SIR of lymphoma have not changed over the survey period (Figure 2). Second, the proportion of patients receiving MTX or tacrolimus has been increasing in those 10 years. Third, the number of patients with remission or low disease activity has been increasing over the years1 (Figure 1). The stable annual SIR of lymphoma might possibly result from a balance between increased lymphoma caused by elevated use of MTX or tacrolimus, but decreased incidence from reduced RA disease activity. Otherwise, assuming that there is a time lag between the administration of those drugs and lymphoma development, the SIR of lymphoma would increase further in future. While the use of MTX or tacrolimus may carry a certain risk for lymphoma development, it should be emphasized that they are now essential for RA disease control.
The limitations of our present study are related to its open prospective cohort registry nature and the smaller proportion of followed-up patients relative to single-center cohorts. That is, only malignancies that the patients developed while attending the hospitals participating in the NinJa registry were recorded. In contrast to single institutional cohorts, which have low dropout rates with close followup of patients, our nationwide multiinstitutional cohort represents an overview of all Japanese patients with RA and has the advantage of excluding biases, such as center effect, ethnicity, and socioeconomic status. Because a single institute specializing in rheumatology tends to accumulate referral patients with poorly controlled RA and to transfer those who do not require active treatment to regional hospitals or family doctors, such single-center studies may focus on unrepresentative, relatively young patients with active and severe RA. Indeed, patients in a large Japanese single institutional cohort were younger and had more active RA than those in our cohort13.
Other limitations of our study lie in the time between the onset of lymphoma and the administration period of a drug. We sought correlations between the onset of lymphoma and medication in the preceding year, on which the significance of the risk for lymphoma was based. The duration of the treatment or whether lymphoma developed during or after the drug administration period was not taken into account. In addition, evaluating the risk of malignancies, including lymphoma, in patients with RA would require the prospective study to include detailed information for variables such as accumulated disease activity, comorbidity, and history of cancer, medication, and smoking. For instance, Sjögren syndrome vastly augments the risk for lymphoma5, just as ILD does for lung cancer. Smoking has been established as contributing to various malignancies, except for several cancers such as breast and prostate cancer, in the general population46. Some studies noted an increased risk for smoking-related cancers in patients with RA47 because smoking is a risk factor for RA per se48, but other studies, including ours, have not. It is not well known whether smoking contributes to the development of such malignancies in patients with RA as in the general population.
Our present study demonstrated that patients with RA have no higher overall incidence of malignancies than the general population, but should be closely monitored for lymphoma development, which is more frequent. Older age, use of MTX, and use of tacrolimus in the preceding year were identified as risk factors for lymphoma development. In studying the risk for malignancy in patients with RA, it is important to discriminate between characteristics of RA (particularly longterm disease activity) and the influence of therapeutic or environmental factors and comorbidities. These influences still need to be investigated. Further work is required to elucidate the mechanisms responsible for increased lymphoma but decreased occurrence of several other malignancies in patients with RA.
Acknowledgment
We thank Mayumi Yokoyama (Sagamihara National Hospital) for secretarial assistance. We also thank Dr. Satoshi Kashiwagi (Amagasaki Medical Coop Hospital), Dr. Masao Katayama (Nagoya Medical Center, National Hospital Organization), Dr. Ryutaro Matsumura (Chiba East National Hospital, National Hospital Organization), Dr. Akira Okamoto (Himeji Medical Center, National Hospital Organization), Dr. Kota Shimada (Tokyo Metropolitan Tama Medical Center), and Dr. Yoshiki Shiohira (Tomishiro Chuo Hospital) for their support in data collection.
Footnotes
-
Supported in part by Grants-in-Aid for Scientific Research from the Ministry of Health, Labor and Welfare of Japan.
- Accepted for publication December 2, 2014.








{kind=link}
{kind=link}