

Systemic lupus erythematosus (SLE) and its treatment have been associated with progressive multifocal leukoencephalopathy (PML)1. We report a case of PML in a 58-year-old woman with SLE treated with belimumab, a biological therapy approved in 2011 for refractory SLE2. To the best of our knowledge, to date, 1 other such case has been described in the literature3. There was no case of PML described in the trials for this drug4.
The patient, diagnosed with SLE in 1978 and stable under hydroxychloroquine, presented in October 2012 with arthritis, rash, thrombopenia, and anemia. Mycophenolate mofetil (MMF) 1500 mg bid and prednisone 10 mg were introduced. In January 2013, her SLE was still active. Belimumab was started with a good clinical response. In July 2013, she presented with a 3-week history of fatigue, apathy, and aphasia. Biological investigations were normal. Brain magnetic resonance imaging (MRI) showed large confluent white matter hyperintensities (Figure 1). A positive PCR of John Cunningham virus in the patient’s cerebrospinal fluid confirmed the diagnosis of PML. After interruption of all immunosuppressive medication, we observed an initial neurological deterioration, probably explained by the immunological reconstitution phenomena. A second MRI showed increased diffuse white matter edema (Figure 2). During the third week, the patient progressively got better. One year later, a moderate aphasia and executive function deficits still persist, rendering her unable to lead an independent life.

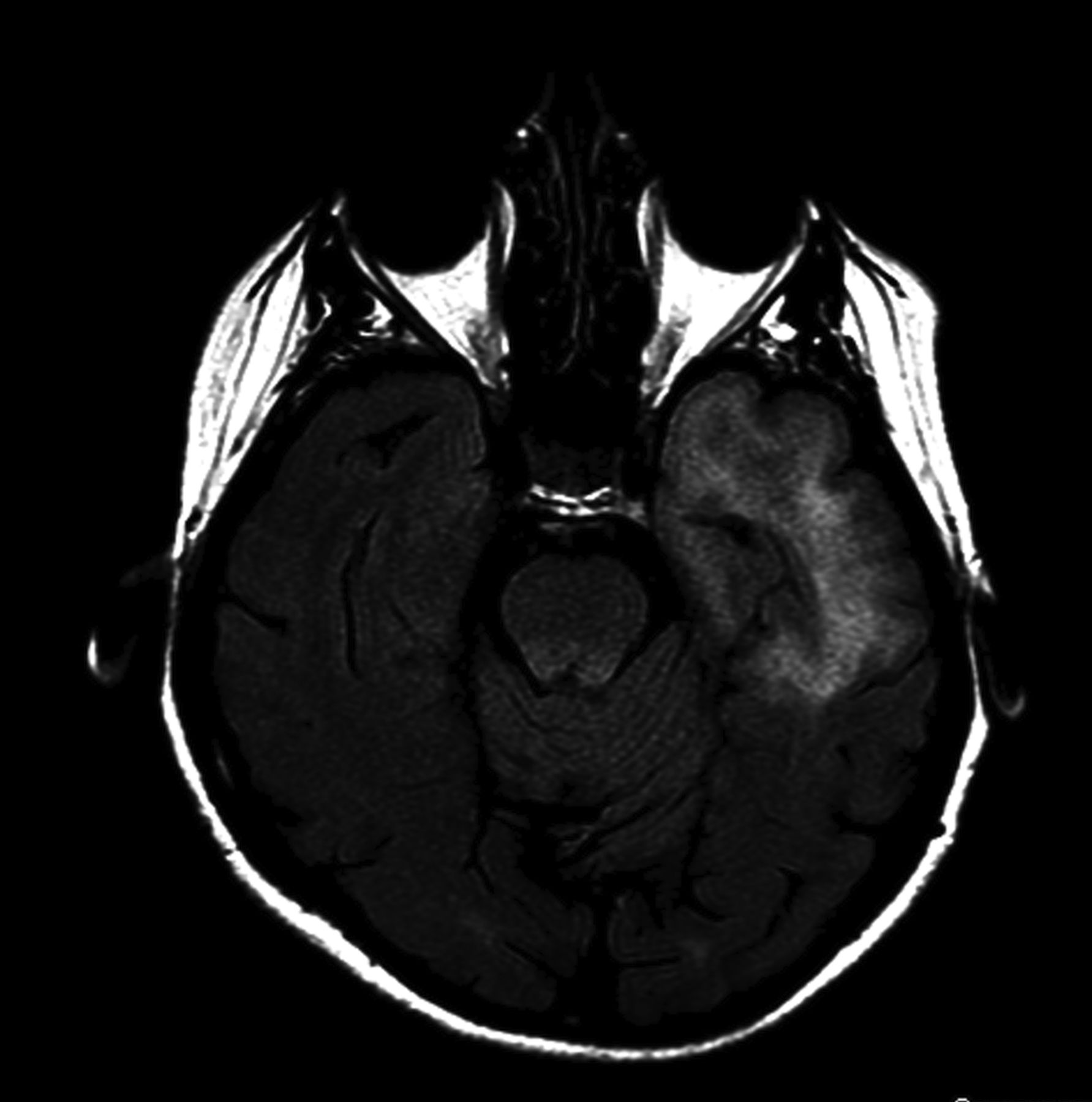
Brain MRI showing extensive and confluent white matter hyperintensities on FLAIR in the left temporal and frontal lobes, and amygdalohippocampic and insular regions. MRI: magnetic resonance imaging; FLAIR: fluid attenuated inversion recovery.

MRI done a week later showed increased white matter hyperintensities on FLAIR. MRI: magnetic resonance imaging; FLAIR: fluid attenuated inversion recovery.
SLE itself and immunosuppressive agents5, including MMF, could have predisposed this patient to PML, but because of the temporal evolution, we believe that belimumab was the principal contributor. Clinicians should be aware of the risk of PML in patients using belimumab.








{kind=link}
{kind=link}