

Article Figures & Data
Figures
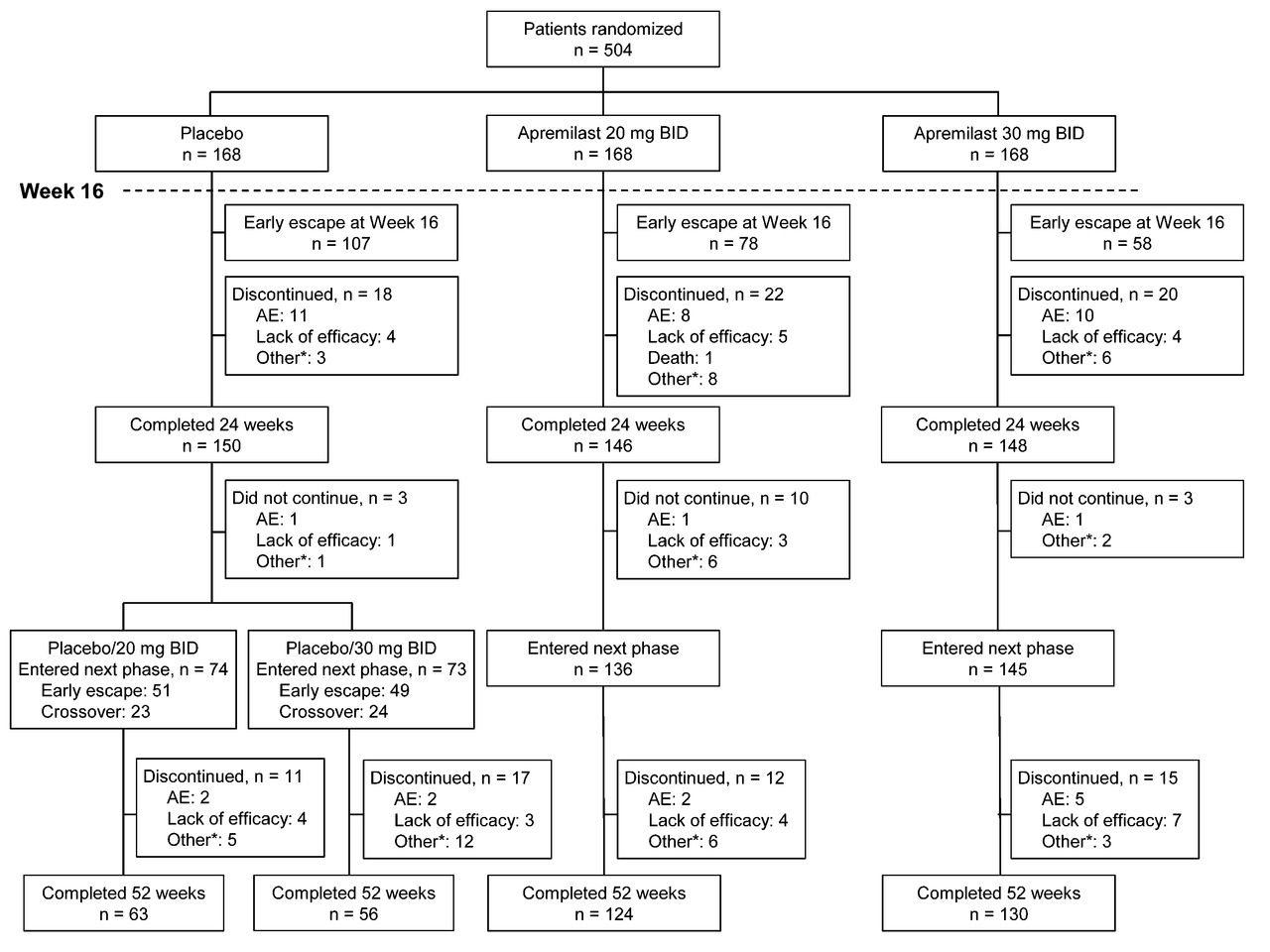
- Figure 1.
Patient disposition. * Includes withdrawal by patient, loss to followup, protocol violation, noncompliance, and other. Patients who discontinued apremilast were encouraged to complete scheduled study assessments. AE: adverse event.
- Figure 2.
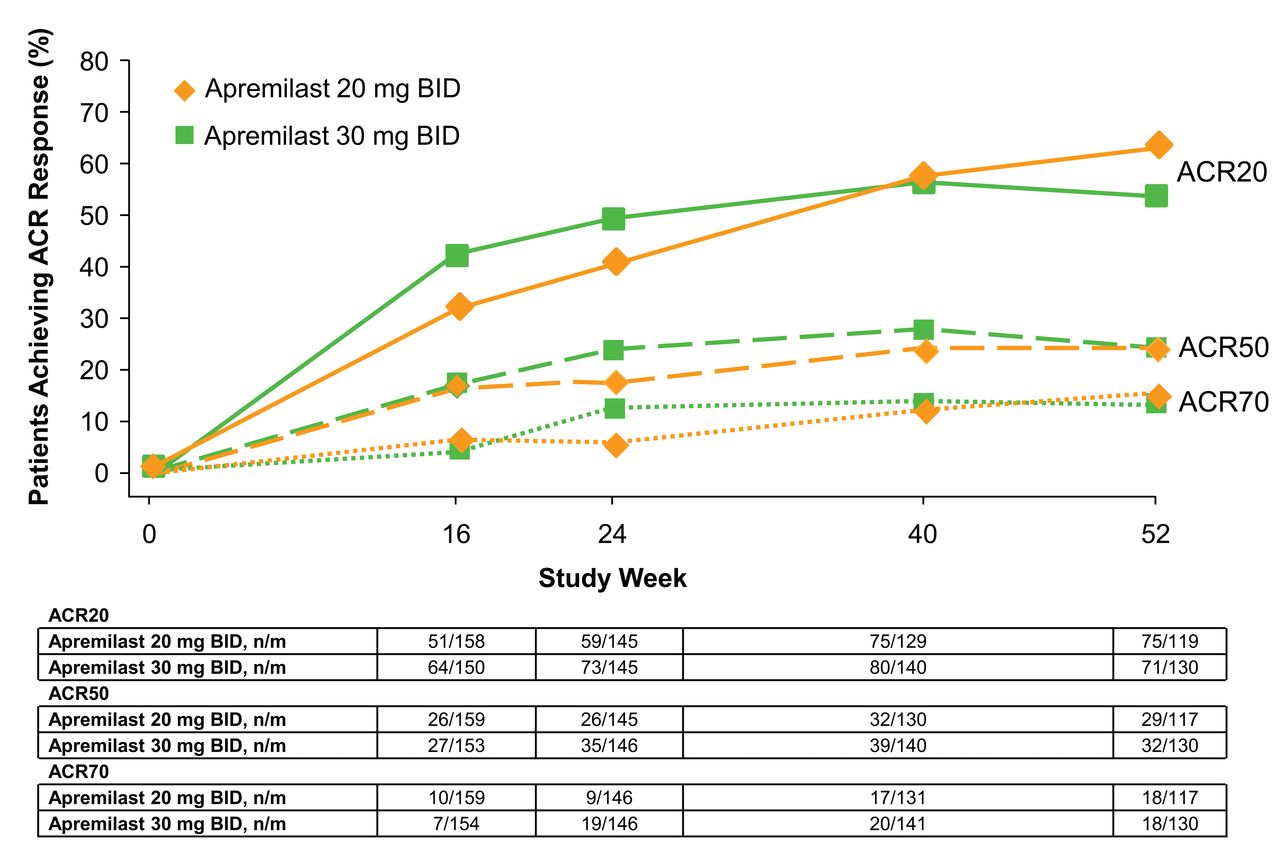
Proportion of patients achieving ACR20 response over 52 weeks. ACR20: American College of Rheumatology 20% improvement; n/m: number of responders/number of patients with sufficient data for evaluation.
- Figure 3.
Proportion of patients receiving apremilast from baseline who achieved ACR20/50/70 over 52 weeks. ACR20/50/70: American College of Rheumatology % of improvement; n/m: number of responders/number of patients with sufficient data for evaluation.
- Figure 4.
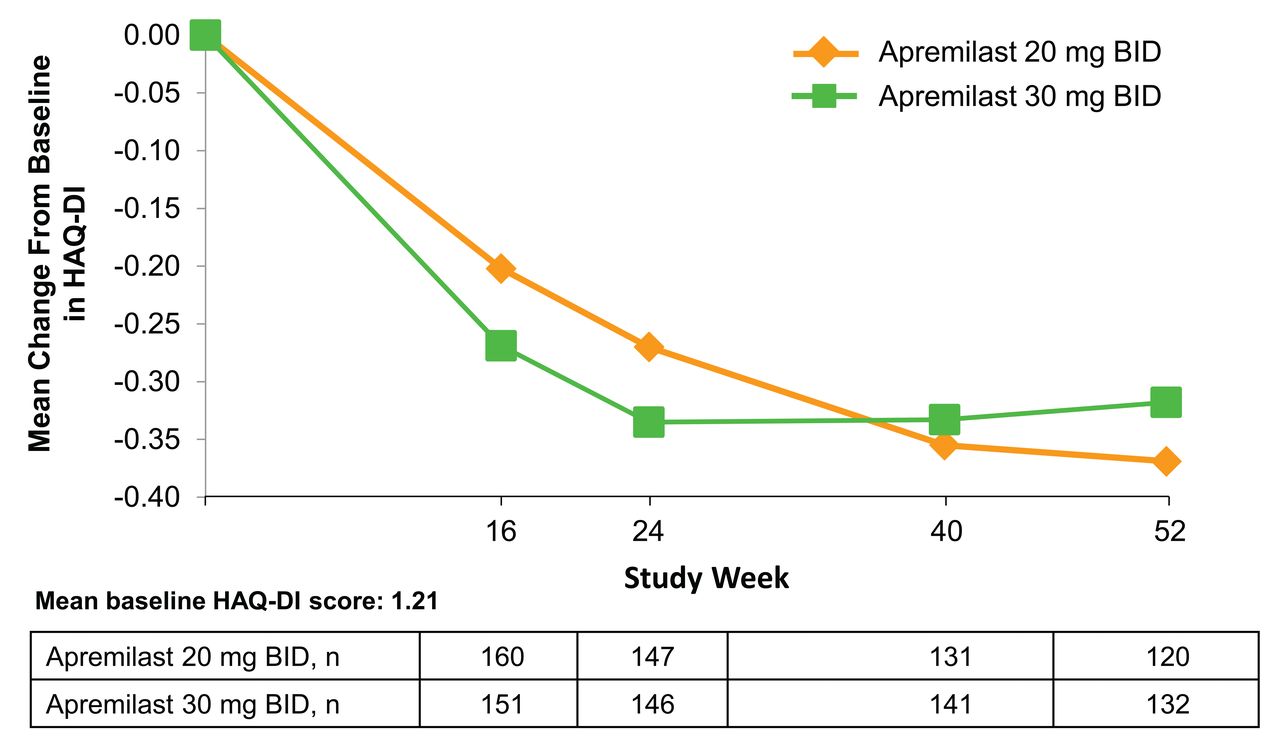
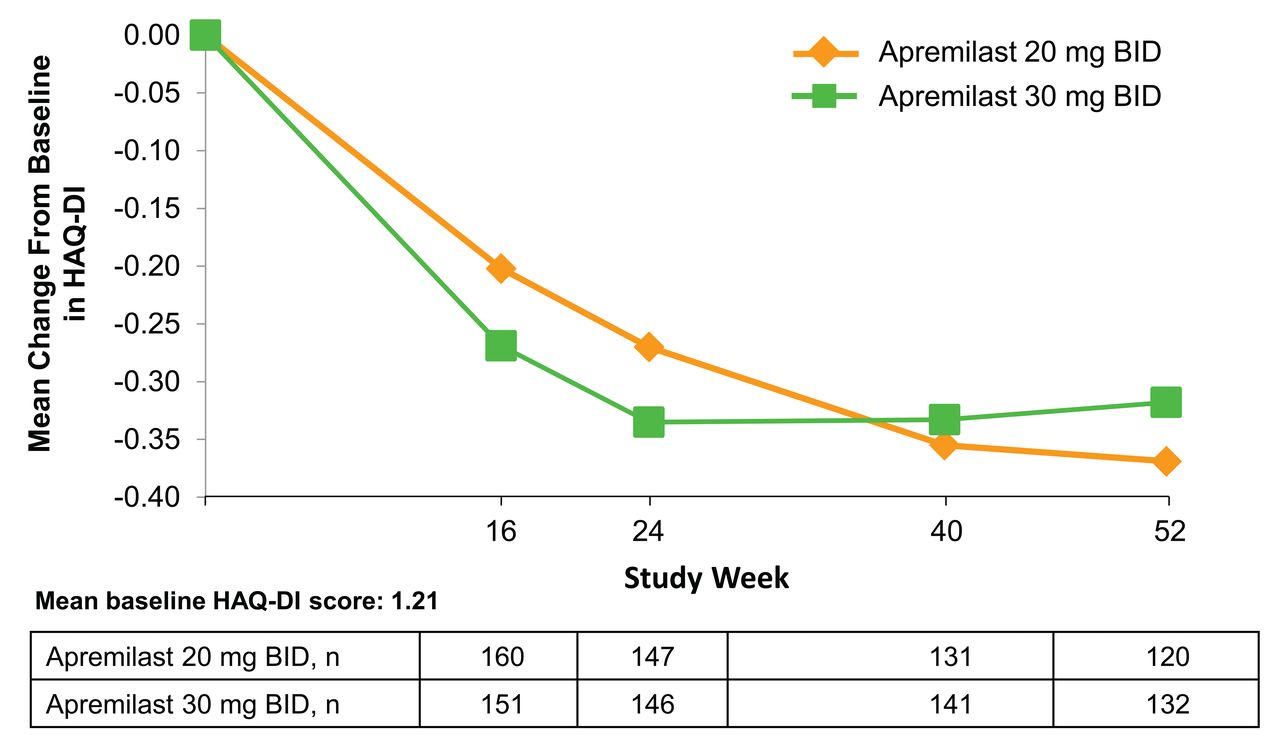
Mean change from baseline in HAQ-DI over 52 weeks in patients receiving apremilast from baseline. HAQ-DI: Health Assessment Questionnaire–Disability Index.



Tables
- Table 1.
Efficacy endpoints at Week 52*. The n reflects the no. patients who completed 52 weeks; actual no. patients available for each endpoint may vary. Values are n/m (%) or mean change (SD) unless otherwise specified.
Characteristics Placebo/Apremilast 20 mg BID, n = 63 Placebo/Apremilast 30 mg BID, n = 56 Apremilast 20 mg BID, n = 124 Apremilast 30 mg BID, n = 130 ACR20 34/64 (53.1) 30/60 (50.0) 75/119 (63.0) 71/130 (54.6) ACR50 16/63 (25.4) 17/61 (27.9) 29/117 (24.8) 32/130 (24.6) ACR70 3/62 (4.8) 9/61 (14.8) 18/117 (15.4) 18/130 (13.8) HAQ-DI, 0–3 −0.27 (0.56) −0.29 (0.59) −0.37 (0.48) −0.32 (0.55) SF-36v2 PF§ 4.5 (8.9) 4.6 (10.0) 7.0 (9.4) 5.7 (9.0) SF-36v2 PCS§ 4.6 (7.7) 5.6 (8.2) 7.8 (8.8) 6.5 (8.7) FACIT-Fatigue 4.3 (8.2) 4.2 (11.7) 4.3 (8.5) 3.7 (9.1) EULAR good/moderate response 53/64 (82.8) 42/60 (70.0) 90/120 (75.0) 96/129 (74.4) mPsARC response 45/61 (73.8) 42/59 (71.2) 93/120 (77.5) 95/129 (73.6) DAS28, CRP −1.5 (1.1) −1.2 (1.3) −1.4 (1.1) −1.3 (1.1) DAS28, CRP, < 2.6 17/65 (26.2) 11/60 (18.3) 39/120 (32.5) 30/129 (23.3) CDAI, 0–76 −15.0 (11.1) −14.0 (14.9) −15.4 (13.0) −14.5 (12.0) MASES, 0–13, median % change‡ −50.0 −40.0 −100.0 −66.7 Dactylitis count, 0–20, median % change‖ −100.0 −100.0 −100.0 −100.0 Swollen joint count, 0–76, median % change −81.0 −66.7 −78.8 −77.8 Tender joint count, 0–78, median % change −63.6 −56.1 −69.2 −62.5 CRP, normal range 0–0.5, mg/dl, median % change −30.4 −5.5 −8.2 −16.2 Patient global assessment, 0–100 VAS, median % change −38.5 −22.1 −36.8 −28.6 Physician global assessment, 0–100 VAS, median % change −70.9 −58.8 −66.7 −61.7 Patient assessment of pain, 0–100 VAS, median % change −33.6 −37.9 −35.6 −30.9 PASI-50¶ 11/25 (44.0) 11/27 (40.7) 28/53 (52.8) 41/68 (60.3) PASI-75¶ 4/25 (16.0) 6/27 (22.2) 13/53 (24.5) 25/68 (36.8) -
↵* Data as observed. Based on patients randomized to apremilast, placebo/apremilast 20 mg BID and placebo/apremilast 30 mg BID groups include patients who were randomized to placebo at baseline and re-randomized to apremilast 20 mg BID and apremilast 30 mg BID, respectively, at weeks 16 or 24; apremilast 20 mg BID and apremilast 30 mg BID groups include patients randomized to the respective regimen at baseline.
-
↵§ Increase indicates improvement.
-
↵‡ Examined among patients with enthesitis at baseline and having data at Week 52 (placebo/apremilast 20 mg BID: n = 36; placebo/apremilast 30 mg BID: n = 36; apremilast 20 mg BID: n = 69; apremilast 30 mg BID: n = 89).
-
↵‖ Examined among patients with dactylitis at baseline and having data at Week 52 (placebo/apremilast 20 mg BID: n = 23; placebo/apremilast 30 mg BID: n = 26; apremilast 20 mg BID: n = 48; apremilast 30 mg BID: n = 49).
-
↵¶ Examined among patients with psoriasis involving body surface area ≥ 3% at baseline. n/m: number of responders/number of patients with sufficient data for evaluation. ACR20/50/70: 20%/50%/70% improvement in modified American College of Rheumatology response criteria; HAQ-DI: Health Assessment Questionnaire–Disability Index; SF-36v2 PF: Medical Outcomes Study Short Form-36 health survey version 2 Physical Functioning domain; PCS: physical component summary score; FACIT-Fatigue: Functional Assessment of Chronic Illness Therapy-Fatigue; EULAR: European League Against Rheumatism; mPsARC: modified psoriatic arthritis response criteria; DAS28: 28-joint Disease Activity Score (using CRP as acute-phase reactant); CRP: C-reactive protein; CDAI: Clinical Disease Activity Index; MASES: Maastricht Ankylosing Spondylitis Enthesitis Score; VAS: visual analog scale; PASI-50/75: 50%/75% reduction from baseline Psoriasis Area and Severity Index score.
-
- Table 2.
AE during the 24-week placebo-controlled and 52-week apremilast-exposure periods. Placebo-controlled period includes data through Week 16 for patients initially receiving placebo who escaped, and data through Week 24 for all other patients. Apremilast-exposure period includes all apremilast-exposure data, regardless of when the apremilast exposure started (weeks 0, 16, or 24).
Characteristics Weeks 0 to 24 Weeks 0 to 52 Apremilast Apremilast Placebo, n =168 20 mg BID, n = 168 30 mg BID, n = 168 20 mg BID, n = 245 30 mg BID, n = 245 Patients, n (%) ≥ 1 AE 81 (48.2) 101 (60.1) 103 (61.3) 164 (66.9) 174 (71.0) Any serious AE 7 (4.2) 8 (4.8) 9 (5.4) 14 (5.7) 19 (7.8) Any severe AE 6 (3.6) 8 (4.8) 11 (6.5) 15 (6.1) 15 (6.1) AE leading to drug withdrawal 8 (4.8) 10 (6.0) 12 (7.1) 16 (6.5) 23 (9.4) Death 0 (0.0) 1 (0.6)* 0 (0.0) 1 (0.4) 0 (0.0) Frequent AE, ≥ 5% in any treatment group, n (%) Diarrhea 4 (2.4) 19 (11.3) 32 (19.0) 27 (11.0) 47 (19.2) Nausea 11 (6.5) 16 (9.5) 31 (18.5) 24 (9.8) 35 (14.3) Headache 8 (4.8) 17 (10.1) 18 (10.7) 22 (9.0) 24 (9.8) URTI 6 (3.6) 10 (6.0) 7 (4.2) 19 (7.8) 14 (5.7) Nasopharyngitis 5 (3.0) 6 (3.6) 8 (4.8) 17 (6.9) 16 (6.5) Select laboratory assessments Marked abnormalities, n/m (%)§ ALT > 150 U/l 0/167 (0.0) 0/166 (0.0) 2/168 (1.2) 0/243 (0.0) 2/245 (0.8) Creatinine, male > 156, female > 126 μmol/l 0/167 (0.0) 1/166 (0.6) 0/168 (0.0) 1/243 (0.4) 0/245 (0.0) Hemoglobin, male: decrease > 2.0 and value < 10.5 g/dl; female: decrease > 2.0 and value < 10.0 g/dl 0/167 (0.0) 0/166 (0.0) 1/168 (0.6) 0/243 (0.0) 2/245 (0.8) Leukocytes < 2.0, 109/l 0/167 (0.0) 0/166 (0.0) 0/168 (0.0) 0/243 (0.0) 0/245 (0.0) Neutrophils < 0.75, 109/l 0/167 (0.0) 0/166 (0.0) 0/168 (0.0) 0/243 (0.0) 0/245 (0.0) Platelets < 75, 109/l 0/166 (0.0) 0/166 (0.0) 0/168 (0.0) 0/243 (0.0) 0/245 (0.0) Select laboratory shifts from normal to > upper limit of normal, n/m (%)§ ALT, U/l 20/150 (13.3) 12/146 (8.2) 12/155 (7.7) 29/215 (13.5) 28/222 (12.6) Creatinine, μmol/l 3/159 (1.9) 7/151 (4.6) 10/158 (6.3) 14/222 (6.3) 16/228 (7.0) Select laboratory shifts from normal to < lower limit of normal, n/m (%)§ Leukocytes, 109/l 1/155 (0.6) 4/155 (2.6) 2/159 (1.3) 5/227 (2.2) 6/232 (2.6) Neutrophils, 109/l 2/146 (1.4) 2/145 (1.4) 5/151 (3.3) 3/213 (1.4) 8/221 (3.6) Platelets, 109/l 0/146 (0.0) 0/142 (0.0) 1/151 (0.7) 1/208 (0.5) 1/221 (0.5) Hemoglobin, g/dl 8/148 (5.4) 7/149 (4.7) 14/153 (9.2) 22/220 (10.0) 26/224 (11.6) -
↵* Multiorgan failure considered by investigator to be unrelated to study medication.
-
↵§ Represents patients with ≥ 1 occurrence of the abnormality (n)/patients with a baseline value of normal and ≥ 1 post-baseline value for criteria requiring baseline or with ≥ 1 post-baseline value for criteria requiring baseline (m). AE: adverse event; URTI: upper respiratory tract infection; ALT: alanine transaminase.
-
- APPENDIX 1.
Baseline demographics and clinical characteristics in PALACE 1: intent-to-treat population (n = 504*). Values are mean (SD) or n (%).
Characteristics Placebo, n = 168 Apremilast 20 mg BID, n = 168 30 mg BID, n = 168 Age, yrs 51.1 (12.1) 48.7 (11.0) 51.4 (11.7) Age ≥ 65 yrs 19 (11.3) 11 (6.5) 22 (13.1) Female 80 (47.6) 83 (49.4) 92 (54.8) Race White 153 (91.1) 150 (89.3) 152 (90.5) Asian 8 (4.8) 8 (4.8) 8 (4.8) Black 0 (0.0) 2 (1.2) 0 (0.0) Other 7 (4.2) 8 (4.8) 8 (4.8) Region North America 81 (48.2) 73 (43.5) 69 (41.1) Europe 39 (23.2) 41 (24.4) 42 (25.0) Rest of world 48 (28.6) 54 (32.1) 57 (33.9) Weight, kg 89.8 (22.4) 88.8 (21.1) 87.1 (19.6) Body mass index, kg/m2 31.1 (6.6) 30.9 (7.3) 30.6 (5.9) Duration of PsA, yrs 7.3 (7.1) 7.2 (6.8) 8.1 (8.1) Swollen joint count, 0–76 12.8 (8.8) 12.5 (9.5) 12.8 (7.8) Tender joint count, 0–78 23.3 (15.2) 22.2 (15.9) 23.1 (14.5) HAQ-DI, 0–3 1.2 (0.6) 1.2 (0.6) 1.2 (0.6) Patient’s global assessment, 0–100 mm VAS 58.8 (22.3) 55.3 (23.7) 55.9 (21.5) Physician’s global assessment, 0–100 mm VAS 55.2 (20.3) 54.1 (21.8) 55.7 (19.2) CRP, mg/dl, normal range < 0.5 1.1 (1.436) 0.90 (1.409) 0.84 (1.024) Patient assessment of pain, 0–100 mm VAS 61.2 (20.2) 54.9 (22.9) 57.9 (20.2) SF-36v2 PF score 33.8 (10.6) 35.1 (10.7) 33.0 (10.2) DAS28, CRP 4.9 (1.0) 4.8 (1.1) 4.9 (1.0) CDAI, 0–76 29.7 (12.0) 28.4 (13.1) 29.4 (11.5) Duration of psoriasis, yrs 15.7 (13.0) 15.5 (11.9) 16.5 (12.3) PASI score, 0–72† 9.1 (9.5) 7.4 (8.7) 9.2 (9.7) Presence of enthesitis 98 (58.3) 103 (61.3) 114 (67.9) MASES, 0–13‡ 5.4 (3.5) 5.0 (3.3) 4.4 (3.1) Presence of dactylitis 68 (40.5) 59 (35.1) 68 (40.5) Dactylitis severity score, 0–20§ 3.3 (3.3) 4.1 (4.2) 2.9 (2.4) Prior use of DMARD, biologic-naive 120 (71.4) 129 (76.8) 124 (73.8) Prior use of biologics 41 (24.4) 37 (22.0) 41 (24.4) Prior biologic failures 19 (11.3) 14 (8.3) 14 (8.3) Baseline DMARD use 110 (65.5) 111 (66.1) 106 (63.1) Methotrexate, mean dose 16.6 mg/week 90 (53.6) 95 (56.5) 88 (52.4) Leflunomide, mean dose, 17.2 mg/day 11 (6.5) 10 (6.0) 9 (5.4) Sulfasalazine, mean dose, 2.3 g/day 18 (10.7) 16 (9.5) 20 (11.9) Baseline corticosteroids¶, mean dose, 6.1 mg/day 12 (7.1) 25 (14.9) 16 (9.5) Baseline use of NSAID 118 (70.2) 123 (73.2) 120 (71.4) -
From Kavanaugh A, et al. Ann Rheum Dis 2014;73:1020–6, with permission.
-
↵* The n reflects the no. randomized patients; actual no. patients available for each endpoint may vary.
-
↵† Examined among patients who had body surface area ≥ 3% affected at baseline.
-
↵‡ Examined among patients who had enthesitis at baseline.
-
↵§ Examined among patients who had dactylitis at baseline.
-
↵¶ Prednisone ≤ 10 mg/day (or equivalent). PsA: psoriatic arthritis; HAQ-DI: Health Assessment Questionnaire-Disability Index; VAS: visual analog scale; CRP: C-reactive protein; SF-36v2 PF: Medical Outcomes Study Short Form-36 health survey version 2 Physical Functioning domain; DAS28: 28-joint Disease Activity Score; CDAI: Clinical Disease Activity Index; PASI: Psoriasis Area and Severity Index; MASES: Maastricht Ankylosing Spondylitis Enthesitis Score; DMARD: disease-modifying antirheumatic drugs; NSAID: nonsteroidal anti-inflammatory drugs.
-
- APPENDIX 2.
Efficacy endpoints at Week 52 in PALACE 1 (value at timepoint, data as observed*). The n reflects the no. patients who completed 52 weeks; actual no. patients available for each endpoint may vary. Values are n/m (%) or mean (SD).
Characteristics Placebo/Apremilast 20 mg BID, n = 63 Placebo/Apremilast 30 mg BID, n = 56 Apremilast 20 mg BID, n = 124 Apremilast 30 mg BID, n = 130 ACR20 34/64 (53.1) 30/60 (50.0) 75/119 (63.0) 71/130 (54.6) ACR50 16/63 (25.4) 17/61 (27.9) 29/117 (24.8) 32/130 (24.6) ACR70 3/62 (4.8) 9/61 (14.8) 18/117 (15.4) 18/130 (13.8) HAQ-DI, 0–3 0.88 (0.64) 0.93 (0.67) 0.74 (0.65) 0.95 (0.66) SF-36v2 PF§ 38.3 (11.1) 39.4 (10.8) 42.5 (10.6) 38.7 (11.1) SF-36v2 PCS§ 38.9 (9.5) 40.4 (9.4) 43.0 (9.9) 40.1 (9.6) FACIT-Fatigue 35.1 (10.3) 32.5 (11.9) 37.2 (10.6) 33.3 (11.2) EULAR good/moderate response 53/64 (82.8) 42/60 (70.0) 90/120 (75.0) 96/129 (74.4) mPsARC response 45/61 (73.8) 42/59 (71.2) 93/120 (77.5) 95/129 (73.6) DAS28, CRP 3.4 (1.2) 3.9 (1.3) 3.3 (1.2) 3.6 (1.3) DAS28, CRP, < 2.6 17/65 (26.2) 11/60 (18.3) 39/120 (32.5) 30/129 (23.3) CDAI, 0–76 14.0 (11.1) 16.9 (12.1) 13.2 (10.9) 15.4 (11.9) MASES, 0–13‡ 3.5 (3.7) 3.9 (3.9) 1.9 (3.1) 2.4 (3.2) Dactylitis count, 0–20‖ 1.8 (3.2) 1.5 (2.8) 0.9 (2.4) 1.2 (2.0) Swollen joint count, 0–76 4.5 (5.9) 6.9 (8.7) 4.4 (7.1) 5.0 (7.3) Tender joint count, 0–78 10.5 (13.8) 12.8 (13.4) 8.5 (11.1) 12.1 (13.8) CRP, mg/dl, normal range 0–0.5 0.69 (0.66) 1.24 (2.76) 0.68 (0.88) 0.79 (1.15) Patient global assessment, 0–100 VAS 41.4 (24.9) 46.7 (27.3) 37.6 (24.5) 40.6 (23.7) Physician global assessment, 0–100 VAS 25.0 (22.1) 28.9 (24.4) 22.5 (21.2) 27.2 (23.3) Patient assessment of pain, 0–100 VAS 40.1 (24.4) 43.6 (25.4) 35.6 (23.2) 39.1 (23.0) PASI-50¶ 11/25 (44.0) 11/27 (40.7) 28/53 (52.8) 41/68 (60.3) PASI-75¶ 4/25 (16.0) 6/27 (22.2) 13/53 (24.5) 25/68 (36.8) -
↵* Data as observed. Based on patients randomized to apremilast: placebo/apremilast 20 mg BID and placebo/apremilast 30 mg BID groups include patients who were randomized to placebo at baseline and re-randomized to apremilast 20 mg BID and apremilast 30 mg BID, respectively, at Weeks 16 or 24; apremilast 20 mg BID and apremilast 30 mg BID groups include patients randomized to the respective regimen at baseline.
-
↵§ Increase indicates improvement.
-
↵‡ Examined among patients with enthesitis at baseline and having data at Week 52 (placebo/apremilast 20 mg BID: n = 36; placebo/apremilast 30 mg BID: n = 36; apremilast 20 mg BID: n = 69; apremilast 30 mg BID: n = 89).
-
↵‖ Examined among patients with dactylitis at baseline and having data at Week 52 (placebo/apremilast 20 mg BID: n = 23; placebo/apremilast 30 mg BID: n = 26; apremilast 20 mg BID: n = 48; apremilast 30 mg BID: n = 49).
-
↵¶ Examined among patients with psoriasis involving body surface area ≥ 3% at baseline. n/m: number of responders/number of patients with sufficient data for evaluation; ACR20/50/70: 20%/50%/70% improvement in modified American College of Rheumatology response criteria; HAQ-DI: Health Assessment Questionnaire-Disability Index; SF-36v2 PF: Medical Outcomes Study Short Form-36 health survey version 2 Physical Functioning domain; PCS: physical component summary score; FACIT-Fatigue: Functional Assessment of Chronic Illness Therapy-Fatigue; EULAR: European League Against Rheumatism; mPsARC: modified psoriatic arthritis response criteria; DAS28: 28-joint Disease Activity Score (using CRP as acute-phase reactant); CRP: C-reactive protein; CDAI: Clinical Disease Activity Index; MASES: Maastricht Ankylosing Spondylitis Enthesitis Score; VAS: visual analog scale; PASI-50/75: 50%/75% reduction from baseline Psoriasis Area and Severity Index score.
-








{kind=link}
{kind=link}
{kind=link}
{kind=link}