

Abstract
Objective. To develop a plan for harmonizing outcomes for people undergoing total joint replacement (TJR), to achieve consensus regarding TJR outcome research.
Methods. The TJR working group met during the 2014 Outcome Measures in Rheumatology (OMERACT) 12 meeting in Budapest, Hungary. Multiple conference calls preceded the face-to-face meeting. Brief presentations were made during a 1.5-h meeting, which included an overview of published systematic reviews of TJR trials and the results of a recent systematic review of TJR clinical trial outcome domains and measures. This was followed by discussion of potential core set areas/domains for TJR clinical trials (as per OMERACT Filter 2.0) as well as the challenges associated with the measurement of these domains.
Results. Working group participants discussed which TJR clinical trial outcome domains/areas map to the inner versus outer core for core domain set. Several challenges were identified with TJR outcomes including how to best measure function after TJR, elucidating the source of the pre- and post-TJR joint pain being measured, joint-specific versus generic quality of life instruments and the importance of patient satisfaction and revision surgery as outcomes. A preliminary core domain set for TJR clinical trials was proposed and included pain, function, patient satisfaction, revision, adverse events, and death. This core domain set will be further vetted with a broader audience.
Conclusion. An international effort with active collaboration with the orthopedic community to standardize key outcome domains and measures is under way with the TJR working group. This effort will be further developed with new collaborations.
Endstage arthritis refractory to medical treatments is common, and this is typically caused by osteoarthritis (OA). At present, total joint replacement (TJR) is the most frequently performed surgical treatment for patients with endstage arthritis refractory to medical treatments, and the most commonly replaced joints are the knee and the hip. In 2010, 719,000 total knee replacements (TKR) and 332,000 total hip replacements (THR) were performed in the United States1,2, with an approximate cost of US$20 billion3.
The published literature suggests that the rate of TJR use is increasing worldwide4,5,6,7,8,9,10. The direct and indirect costs of treating endstage refractory arthritis are increasing as a result of the aging population, increasing prevalence of obesity, and limited alternative options. There is a growing need to better understand the overall benefits and risks of TJR, within the context of healthcare access and payer considerations, patient preferences and priorities, and clinician factors.
In the setting of endstage arthritis treated with interventions such as TJR, the range of relevant outcomes is diverse. Outcome may depend on the underlying arthritis type and its severity, coexistent medical comorbidity, and complications and adverse events that arise from the treatment. Longer-term outcomes are also related to patient expectation, satisfaction, and participation. For example, there is a wide variation in functional outcomes following TJR11. Although TJR is currently the most commonly used treatment for patients with endstage arthritis, other therapies, such as cartilage/stem cell transplant and other new surgical or medical therapies, may emerge as viable treatment options in the next decade.
It is increasingly recognized that having a core set of standardized outcome measures for TJR clinical trials is needed to interpret and compare findings from different studies. While short-term outcomes such as medical and surgical complications (e.g., myocardial infarction, pulmonary embolism, periprosthetic fracture, etc.), length of hospital stay, and 30- and 90-day readmission rates are defined by discrete events and are therefore easy to measure and report, other outcomes such as pain, function, and quality of life have been inconsistently measured and reported.
Because of these challenges, an Outcomes in Rheumatology (OMERACT) TJR working group was formed in 2008 for the harmonization of TJR clinical trial outcomes and was convened at OMERACT 9 in 2008 at Kananaskis, Alberta, Canada. The main discussion focused on the lack of consistency of TJR clinical trial outcomes12,13. Subsequently the working group again met at OMERACT 10 at Kota Kinabalu, Indonesia, and discussed findings from a large international study assessing whether pain and functional limitation were predictors of recommendation for TJR14. The TJR working group was further expanded in 2012, incorporating a broader membership including orthopedic surgeons and the leaders of arthroplasty registries, and met again at the OMERACT 12 meeting in Budapest, Hungary, in 2014.
A new development is the publication of the OMERACT Filter 2.0, based on the World Health Organization (WHO) International Classification of Functioning, Disability, and Health (ICF) model15. It is recommended as the framework for developing outcome core sets for any condition. Details of this filter are provided elsewhere15,16,17,18,19,20,21,22. It has 4 core areas to assess the influence of disease, namely death, life impact, resource use/economic impact, and pathophysiological manifestations15. Resource use is an optional core area and may be included on a condition-by-condition basis. Within each core area, there are multiple domains.
The objective of the 2014 OMERACT arthroplasty/joint replacement working group was to bring together clinical and methodological experts in epidemiology, psychometrics, orthopedics, and rheumatology with patient partners and others interested in harmonizing outcomes for people undergoing arthroplasty, to set the future agenda to achieve an international consensus-based core set of outcome domains and measures for use in TJR clinical trials. This article summarizes the work completed at this point toward achieving this aim, and our future plans. We summarize the results of previous systematic reviews and prospective studies performed by our group to identify gaps in outcome assessments in TJR clinical trials12,13,14,23,24,25,26, and a new systematic review of TJR clinical trials performed in preparation for the 2014 OMERACT meeting, currently under review elsewhere (Step 1) and the current and the future work in patient involvement and collaboration with surgeons (steps 2–3). Finally we outline future plans (steps 4–7) and highlight the main discussions and decisions from the working group meeting at OMERACT 2014.
Step 1. Systematic Reviews and Studies to Identify Gaps in Outcome Measurement in TJR Trials and Their Methodological Quality and Application of OMERACT Filter 2.0 to the Development of Outcomes
The systematic reviews summarized in the section below have identified the gaps in outcome measurement in TJR trials and were the reasons for forming this working group. The OMERACT filter provides a framework for deriving the TJR clinical trial core set measures.
Variation in outcome measures in TJR clinical trials
Riddle, et al conducted a systematic review of the use of outcome instruments used in knee and hip joint replacement clinical trials conducted between 2000 and 2007, using the WHO ICF conceptual model to categorize outcomes12. Among the 160 studies included for review, at least 20 different outcome measures were used in the hip trials, and at least 14 different measures were used in knee trials. The primary outcome was identified in only 24% of trials. There was an extensive variation across trials in the general construct being measured.
Role of pain and functional impairment in the decision to recommend TJR
Gossec, et al conducted a large international cross-sectional study of 1909 patients to define the pain and functional impairment cutpoints that correlate with the orthopedic surgeon’s decision to recommend TJR in patients with hip or knee osteoarthritis23. They were unable to determine the cutpoints for pain and function defining “requirement for TJR” because of considerable overlap of pain and functional disability between patients recommended and not recommended for TJR23.
Methodological quality of arthroplasty clinical trials
A systematic review of 196 arthroplasty clinical trials published in 2007 to 2008 found that the overall quality of arthroplasty trials was low and that the type of intervention, number of trial centers, and presence of funding were independently associated with overall trial quality24. In another analysis of these data, we found that larger sample size studies were associated with positive trial outcomes and that study sample size mediated the previously observed association of study quality with study outcome25.
Systematic reviews of hip and knee TJR epidemiology and outcomes
A systematic review of epidemiology of TKR and THR found that TJR rates were increasing over time and varied by key patient characteristics (age, race, socioeconomic status, country setting)10. In a systematic review of 30- and 90-day mortality rates in patients undergoing TKR or THR, we found that male sex and bilateral procedures were associated with higher 30-day mortality and with nonsignificant trend for higher 90-day mortality26.
We have recently completed a systematic review of TJR clinical trials that assessed to what extent the outcomes reported (1) met the truth, discrimination, and feasibility filter and (2) mapped the reported outcomes to OMERACT Filter 2.015. We noted that outcomes reported in TJR clinical trials mapped to only a few core areas of OMERACT Filter 2.0; notable gaps were reporting of core areas of death and resource use. Detailed findings of this systematic review to be published elsewhere, as recommended during group discussion at OMERACT 12 (manuscript under review), will lay the foundation for defining a final core domain set for TJR clinical trials.
The role of OMERACT Filter 2.0 framework in standardizing TJR outcomes
We will use the framework of OMERACT Filter 2.0 for developing TJR outcomes. For a condition to have a complete validated core outcome measurement set, at least 1 domain should be included from each of the 3 core areas (core domain set; with a consideration of whether resource use should be included as the fourth core domain) and at least 1 validated measure should be available (or developed) for each domain. To decide what to measure within the scope of a TJR clinical trial, a working group will first need to specify what should be included in a core domain set and core outcome measurement set.
There are several key issues related to the selection of core areas/outcome domains and measures in TJR clinical trials. What is the core set of domains for TJR that should be reported in every TJR clinical trial? Can we develop this core set with the input of many interested parties? Should the core area of resource utilization/economic impact be included? Can we identify valid measures of these core set domains and harmonize them? How can we reduce heterogeneity and promote a standard nomenclature, standard data collection, and use of validated measures in TJR research?
Our aim is to identify which measures should be used in TJR clinical trials through an established OMERACT-based method27. We have used the patient, intervention, comparator, and outcome (PICO) statement endorsed by the Cochrane Collaboration to help clearly define the type of trials for which we hope to harmonize outcome domains and measures28. The condition for which patients commonly undergo TJR is refractory arthritis pain, which is also required to be specified as the “condition/disease” for OMERACT Filter 2.0, so that a core domain set and measurement core set can be developed. Because TJR is the most commonly used option available to such patients and data are available, it will be our focus. The elements of PICO:
Patient (P). Patients with endstage osteoarthritis of knee or hip refractory to medical and other nonsurgical treatments, who are candidates for intervention/s such as elective TJR (and other interventions in the future) Intervention (I). Any intervention (total joint replacement is the most common intervention at present) Comparator (C). Any surgical or nonsurgical comparator Outcome (O). To be defined using the data, consensus process and the OMERACT filter
As an example, there are several potential core domains for TJR clinical trial outcomes that map to OMERACT Filter 2.0 and need further exploration with the involvement of patients, providers, and policy makers. Life impact domains such as patient perception of health, loss of ability to work, psychosocial effect, secondary effect on family and caregivers and utility, may be relevant and need further exploration. Strong and early involvement of patients, a key strength of the OMERACT process, can help us streamline which of these areas are critical for patients with endstage refractory arthritis undergoing TJR. Pathophysiological manifestations such as immediate postoperative complications and delayed implant related complications are important to define for TJR trials. Healthcare use is an important aspect, given the effect on healthcare costs and impressive improvement in quality of life demonstrating its value.
Step 2. Active Patient Engagement in the Validation Process
Central to the OMERACT process is the recognition that patient engagement in the process of outcome measure selection and validation across different settings and populations is paramount. We have included 2 patient partners on our team, who have been integral to the discussions to define core domains for TJR clinical trials. Both patients have actively participated in premeeting conference calls and the face-to-face working group discussion. We plan to identify more patient partners/patient groups in our research. Patient partners will participate in Web surveys and Delphi exercises to identify and achieve consensus on a final list of TJR outcome domain core set and measures and will be at the table for these key decisions.
Step 3. Involve Multistakeholder International Collaborators Interested in TJR Outcome
We have engaged several key organizations who are working group members, including the International Society of Arthroplasty Registries (ISAR; Goran Garellick and Steve Graves); Function and Outcomes Research for Comparative Effectiveness in TJR registry (FORCE-TJR; Patricia Franklin, working group member)29; American Association of Hip and Knee Surgeons (AAHKS), and American Joint Replacement Registry30 (AJRR; Michael Dohm, co-chair; and David Lewallen, working group member); the Orthopaedic Research Society, the Orthopaedic Evidence and Outcome Education Organization Research Interest Group (Michael Dohm, co-chair); the International Consortium of Orthopaedic Registries (ICOR; Art Sedrakyan, working group member)31; and the American Physical Therapy Association (Daniel Riddle, coauthor). Active participation by several of these leaders, most of whom are orthopedic surgeons, is a clear endorsement that TJR clinical trial outcome harmonization is an area of interest for orthopedic surgeons. For the first time in the history of OMERACT, several orthopedic surgeons attended the working group meeting. Our plan is to foster these collaborations and relationships to achieve common goals.
We will liaise with multiple groups actively working in the area of TJR care to evaluate the current status of outcomes, so that we can work in collaboration, rather than in competition. We believe OMERACT would provide a unique forum for discussion and consensus. There are active efforts under way, but few starting with patient input and Delphi panels and using an established framework. As a starting point, we will establish links to several organizations we have identified so far. With discussions under way, we will collaborate with organizations such as ISAR, and the International Consortium for Health Outcomes Measurement will provide a forum to identify the most meaningful outcome measures and to harmonize the measures being used to assess TJR outcomes. The ISAR has a wide membership from several arthroplasty registers in Sweden32, Norway33, Finland34, the United Kingdom35,36, New Zealand37, Australia38, and Canada39, to name a few. Several of these groups, such as AAHKS, AJRR, ICOR, and FORCE-TJR, are currently collaborating with ISAR and with each other to follow standardized reporting of implant-related outcomes as well as patient-reported outcomes.
Step 4. Make a Working Group of TJR Trialists, Registry Leaders, Patients, and Methodologists
We plan to form a core group of 6 to 12 key TJR trialists and registry leaders, patients, and methodologists. We will then agree on an agenda for this effort that is harmonized with other international TJR outcome initiatives and the proposed timeline, as well as clear understanding of partner organizations, their role/s, and the rules of engagement.
Step 5. Conduct Delphi and Consensus Meetings Online and In-person to Develop Data-driven Consensus for Core Domains for Patients with Endstage Refractory Arthritis Seeking TJR
We will discuss the potential core domains, and in a consensus-based method using Delphi and/or nominal group approach, agree on TJR core domains. With active discussion and voting on the core domains, we will generate a proposed core domain set. This will be discussed further in the next round of Delphi or face-to-face consensus meeting. A consensus will be achieved.
Step 6. Develop a Core Domain Set for Endorsement by the Larger Community of Stakeholders
Once the core domain set is constructed by the working group, with the help of the working group international experts (also leaders in the field of orthopedic trials/outcomes), we will identify the groups and e-mail listings to obtain buy-in and feedback from a larger orthopedic community regarding the relevance and acceptability of the core domain set.
Step 7. Do TJR Outcome Measures Meet Truth, Discrimination, and Feasibility?
Once the core set domains have been defined, we will evaluate the literature to identify the most common measures used in determining TJR outcome in TJR clinical trials, which builds on our previous work that described the heterogeneity of outcome measures13. We will include discussion from representative individuals from many different countries and societies to reach consensus about what measures should be used to obtain the highest level of evidence. This will lead to the development of TJR core measurement set that meets the truth, discrimination, and feasibility filter.
Highlights of the discussion at the TJR working group meeting at OMERACT 12
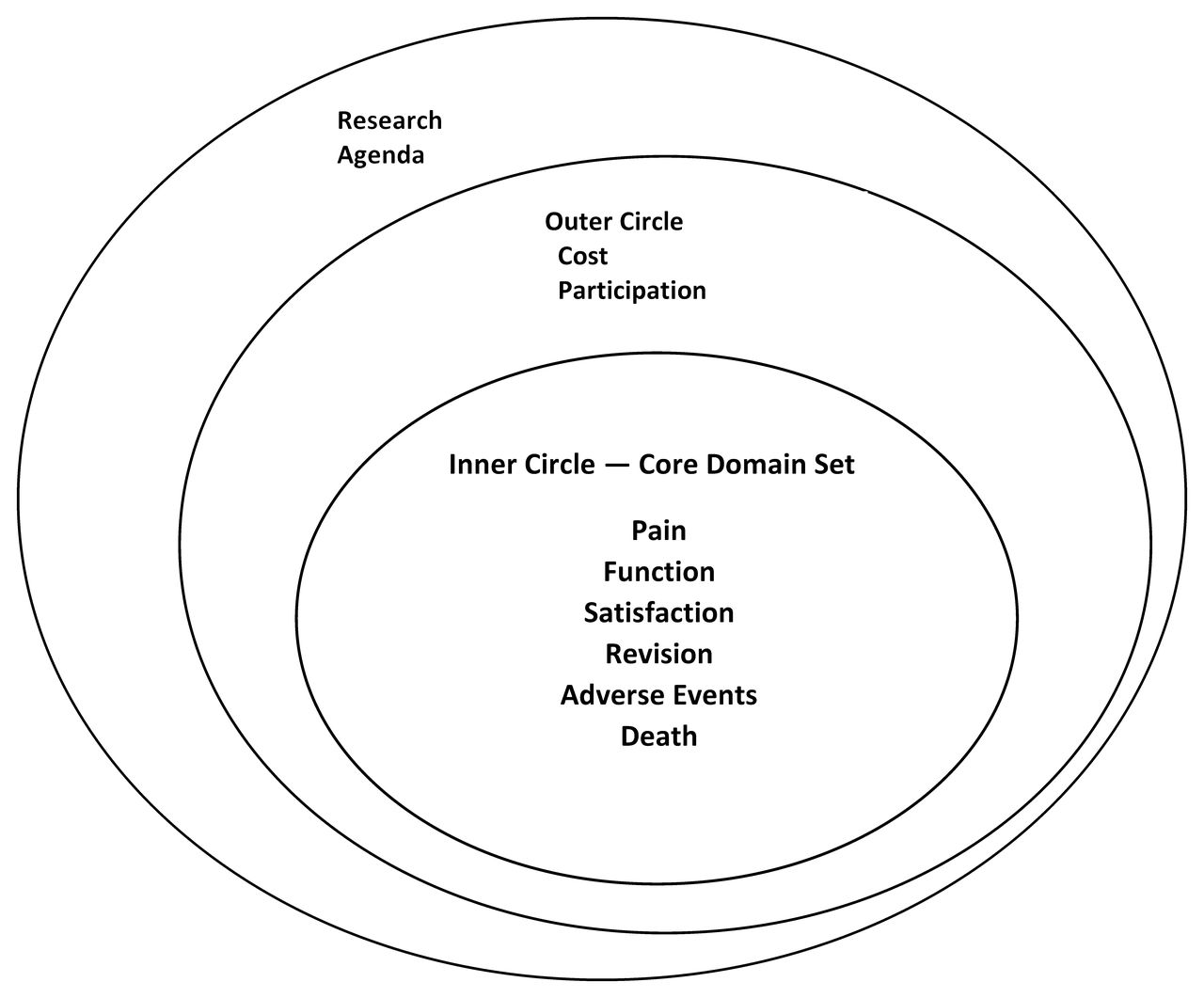
Working group participants reviewed and discussed various outcome domains proposed for inner versus outer circle for core domains. A preliminary core domain set for TJR clinical trials was endorsed during the face-to-face working group meeting at OMERACT 2014, using a Delphi process (Figure 1). This included pain, function, patient satisfaction, revision, adverse events, and death. Participants also brought several important questions for discussion, summarized as follows:

Proposed preliminary core domain set for outcome domains for TJR clinical trials. TJR: total joint replacement.
Pain
Discussants said that both pre- and post-TJR pain severity are important. They also clarified that the domain should be specified as joint pain. Other issues they raised were the persistence of pain even after treatment of the index joint, due to the involvement of other lower extremity joints or the opposite side joint.
Function/functional ability
This was hotly debated because there were differing views regarding how to measure this domain. Discussants argued about whether this meant only daily activity or active sport in the very young individuals. People agreed in general that this should be measured, but were not clear how to best define this domain.
Quality of life
The working group discussed the issue of joint-specific versus generic quality of life instruments and the importance of patient satisfaction as outcomes. Medical Outcome Study Short Form-36 and its utility and limitations were briefly discussed. Some participants were interested in seeing a joint-specific, health-related quality of life assessment.
Revision
Surgeons considered revision a very important outcome.
Cost
Participants recommended pushing this domain to the outer core.
Research agenda
(1) Consider how we should measure function: Will this depend on what activities of daily living patients usually perform and value? Will this vary for the young, athletic patients versus older patients? For patients who are employed outside the home versus those who work at home? (2) Conduct a prospective study on ways to measure change in function post-TJR that are most relevant to patients.
Challenge: Engagement and shared ownership with orthopedic surgeons
The name OMERACT is synonymous with and well known in the rheumatology community, but not so in the orthopedic community. For the TJR working group to have any meaningful influence and to harmonize outcome measures in TJR clinical trials, which are largely conceived and run within the orthopedic community, it may be necessary to consider in part rebranding this part of OMERACT and/or allowing shared ownership.
We propose an “International Consensus of Outcome Measures in TJR Clinical Trials,” building on our TJR working group initiative at the OMERACT. This structure will be based on the framework of the Proceedings of the International Consensus Meeting on Periprosthetic Joint Infection chaired by Parvizi and Gehrke in 201340,41, pending receipt of funding for a large group meeting. Such a meeting will provide the opportunity to discuss and define meaningful outcomes in TJR through a collegial collaboration by examining the evidence, evaluating performance, and determining quality and value in pursuit of best practice. We seek to improve patient outcome after TJR, reduce the burden of revision and improve survivorship, and improve value through identifying those measures that identify best practice and help reduce variation in care.
Next Steps
Our first objective is to define the final core domain set from the proposed preliminary core domain set. Once we have completed the identification of a core domain set, outcome measures will be identified, leading to the development of a core outcome measurement set for TJR clinical trials. We will also explore additional aspects of TJR outcome, such as standardization of TJR clinical trial reporting. Future plans include collaboration with other groups that are leading efforts in registries, such as ISAR and the International Consortium for Health Outcomes Measurement, to identify a core domain set of outcomes for TJR registries as well. The resulting list of domains/areas may be smaller compared to TJR clinical trials, given a more limited scope, limited resources, and lack of an intervention being tested. Our future agenda will be discussed with the other organizations leading this effort.
Acknowledgment
Co-author Dr. Andrew P. Sprowson died unexpectedly on March 13, 2015. The authors remember him as an orthopedic surgeon with immense enthusiasm for research and for robust clinical evidence in the field of joint replacement surgery. He was an integral part of the special interest group for joint arthroplasty within OMERACT, and a great friend. He left a wife and 2 children.
We thank working group members who participated in the preconference teleconferences and provided feedback on our plans to achieve consensus and on the preconference paper, including Dr. Patricia Franklin and Dr. Steven Graves. We also thank patient partners Amye Leong and Marieke Scholte for providing critical feedback during discussions, in person, and during conference calls. Finally, we thank all the group members for informal feedback to the discussions during teleconferences, which have helped to shape our agenda and work to date.
Current special interest group (SIG) members and proposed collaborators: Co-chairs: Jasvinder Singh (USA), Michael Dohm (USA), Andrew Sprowson (UK), and Rachelle Buchbinder (Australia). OMERACT Executive Liaison: Laure Gossec (France). Fellows: Peter Wall (UK) and Bethan Richards (Australia). Patient partners: Amye Leong (USA); Marieke Scholte (Netherlands). A partial list of other SIG core members: Matt Costa (UK); George Wells (Canada); Maxime Dougados (Europe); Gillian Hawker (Canada); Mario Lenza; Dirk Stengel (Germany); Gustavo Zanoli (Italy); Laure Gossec (France); Bing Bingham (USA); Vibeke Strand (USA); Daniel Riddle (USA); David Lewallen (Mayo registry; USA); Patricia Franklin (USA); Eric Bohm (Canada); Ashley Blom (UK registry, UK); Damian Griffin (UK); Cori Borkhoff (Canada).
Footnotes
↵* Dr. Sprowson died March 13, 2015.
JAS is supported by grants from the US Agency for Health Quality and Research Center for Education and Research on Therapeutics, National Institute of Arthritis, Musculoskeletal and Skin Diseases P50, National Institute of Aging U01, National Cancer Institute, the resources and the use of facilities at the Veterans Affair (VA) Medical Center at Birmingham, Alabama, and research contract CE-1304-6631 from the Patient Centered Outcomes Research. JAS has received research grants from Takeda and Savient and consultant fees from Savient, Takeda, Regeneron, and Allergan. JAS is a member of the American College of Rheumatology’s Guidelines Subcommittee of the Quality of Care Committee; the VA Rheumatology Field Advisory Committee; and the executive of OMERACT, an organization that develops outcome measures in rheumatology and receives arms-length funding from 36 companies.
REFERENCES
In this issue








{kind=link}
Jump to section
- Article
- Abstract
- Step 1. Systematic Reviews and Studies to Identify Gaps in Outcome Measurement in TJR Trials and Their Methodological Quality and Application of OMERACT Filter 2.0 to the Development of Outcomes
- Step 2. Active Patient Engagement in the Validation Process
- Step 3. Involve Multistakeholder International Collaborators Interested in TJR Outcome
- Step 4. Make a Working Group of TJR Trialists, Registry Leaders, Patients, and Methodologists
- Step 5. Conduct Delphi and Consensus Meetings Online and In-person to Develop Data-driven Consensus for Core Domains for Patients with Endstage Refractory Arthritis Seeking TJR
- Step 6. Develop a Core Domain Set for Endorsement by the Larger Community of Stakeholders
- Step 7. Do TJR Outcome Measures Meet Truth, Discrimination, and Feasibility?
- Next Steps
- Acknowledgment
- Footnotes
- REFERENCES
- Figures & Data
- Info & Metrics
- References
- eLetters