

Abstract
Objective. To study short-term and longterm clinical and radiographic outcomes in patients with early rheumatoid arthritis (RA) in the first decade of the biologic treatment era.
Methods. Patients with early RA diagnosed at a rheumatology outpatient clinic were consecutively enrolled between 1999 and 2001. Data were collected on demographic characteristics, disease activity, patient-reported outcomes, and treatments. Radiographs of hands and feet were performed at baseline and after 2, 5, and 10 years and scored according to the Sharp/van der Heijde method, yielding a modified total Sharp score (mTSS).
Results. Mean baseline age for the 94 included patients (36 men and 58 women) was 50.4 years and symptom duration 12.3 months; 67.8% were rheumatoid factor–positive. The proportion of patients in remission and in low, moderate, and high disease activity status was at baseline 4.3%, 1.1%, 35.1%, and 59.6% and at 10 years 52.1%, 20.5%, 27.4%, and 0.0%, respectively. For the period 0–2 years, 62.8% had used prednisolone, 91.5% synthetic disease-modifying antirheumatic drug (DMARD), and 18.1% biologic DMARD, and for the period 2–10 years the numbers were 50.6%, 89.3%, and 62.7%, respectively. At baseline, 70% of the patients had erosions on radiographs. Mean annual change in mTSS was for 0–2 years 3.4, 2–5 years 1.7, and 5–10 years 1.2.
Conclusion. A large proportion of our patients with RA diagnosed and treated in the new biologic treatment era achieved a status of clinical remission or low disease activity and had only a minor increase in radiographic joint damage after the first years of followup.
- RHEUMATOID ARTHRITIS
- CLINICAL OUTCOME
- DISEASE ACTIVITY
- PATIENT-REPORTED OUTCOME MEASURES
- RADIOGRAPHIC JOINT DAMAGE
The introduction of biologic disease-modifying antirheumatic drugs (bDMARD) in the treatment of rheumatoid arthritis (RA) has had a major influence on patient treatment in rheumatology1. Later in the same era of biologic treatment, early and target-directed treatment of RA has been shown to improve clinical and radiographic outcome2 and has become a recommended standard of clinical care3.
After the introduction of bDMARD in 1999, numerous registries were established to examine their effectiveness and safety4. The effectiveness of tumor necrosis factor (TNF) inhibitors on clinical outcome in patients with RA, demonstrated in numerous randomized controlled trials5,6,7, has been confirmed in patient registries8,9,10,11,12. Registry data demonstrating a favorable radiographic outcome in patients with RA treated with bDMARD are less common13,14. There is a lack of real-life data reflecting the longterm outcome in clinical status and especially radiographic joint damage in patients who were diagnosed with RA and followed in clinical practice in the new treatment era.
The primary aim of our study was to describe short-term and longterm clinical and radiographic outcome in patients diagnosed with RA treated in the era of bDMARD. We also examine potential predictors of radiographic joint damage and assess for potential associations between clinical outcomes and radiographic joint damage in these patients.
MATERIALS AND METHODS
Study design
Our study was designed as a prospective longterm observational study of patients diagnosed with RA and followed in a rheumatology outpatient clinic in Norway. The patients were consecutively enrolled between 1999 and 2001. To be included, patients had to fulfill the American College of Rheumatology (ACR) 1987 revised classification criteria for RA15. The patients had to agree and have the intention to participate in a longterm followup study with predefined study visits as described below. Patients with reduced life expectancies and patients who could not give confirmed consent were not asked to participate. All participating patients were informed that treatment would be given according to the treating doctor’s judgment during followup and that participation in the study would not influence treatment choice. The main purpose for the standardized visits was to collect data according to protocol. Treatment adjustments were intended to be performed at ordinary clinical visits but could also be performed at the predefined study visits.
Patients and data collection
The systematic collection of demographic, clinical, and treatment data was performed at baseline and after 6 months, and 2, 5, and 10 years of followup. Demographic data reported in our study included age, sex, body mass index (BMI), smoking status, and symptom duration prior to inclusion. Disease activity measures included the laboratory data C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) and 28 swollen and 28 tender joint counts performed by experienced rheumatologists and trained nurses. The composite Disease Activity Score (DAS) containing 28 swollen and 28 tender joint count and ESR (DAS28-ESR3) was also calculated. DAS28-ESR3 was used because data on patient’s global assessment for use in DAS28 calculation were not collected. We applied the same cutoffs as used for DAS28-ESR to define remission (≤ 2.6) and low (2.6 < DAS28 ≤ 3.2), moderate (3.2 < DAS28 ≤ 5.1), and high (DAS28 > 5.1) disease activity16. We also registered data for rheumatoid factor (RF) at baseline and anticitrullinated protein antibody (ACPA) during followup because ACPA tests were not used in our clinical practice when this study started.
Patient-reported outcome (PRO) included joint pain reported by the patient on a visual analog scale (VAS 0–100 mm) and the Modified Health Assessment Questionnaire (MHAQ) assessing physical function17.
At all visits and between visits, the use of prednisolone and synthetic and biologic DMARD were registered.
For each patient, cumulative doses of intramuscular and intraarticular glucocorticosteroids (GC) between visits were calculated and transformed into equivalent prednisolone doses. Cumulative doses of prednisolone and total cumulative GC dose were calculated for the individual patient.
Radiographs of hands and feet
Conventional radiographs of hands, wrists, and feet were performed at baseline and at 2-, 5-, and 10-year followup visits. Joint damage was scored by 1 experienced reader (PB) according to the Sharp/van der Heijde method, yielding a modified total Sharp score (mTSS), with a total score range from 0 to 44818. The intrareader reproducibility expressed as intraclass correlation coefficient was for mTSS 0.83. The smallest detectable change (SDC) for mTSS was 4.9 mTSS units/yr.
Statistical analysis
All analyses were performed with available data without imputation of missing data. Continuous variables with normal distribution were presented as mean (SD) whereas variables with non-normal distribution also were presented with median and interquartile range (IQR). Categorical variables were presented as numbers and percentage.
Mean values for disease activity measures and PRO were calculated for the time period 0–2 (baseline, 6-month, and 2-yr visit), 2–10 (2-, 5-, and 10-yr visit) and for the whole 0–10 year period based on available data from all the visits.
Mean and median annual change in mTSS was calculated for the time periods between the visits based on available radiographic data. Baseline erosive disease was defined as erosions present on baseline radiographs. Percentage of patients with annual progression in radiographic joint damage for the various time periods was calculated with the following cutoffs: > 0, > 1, > 2 units in mTSS and the SDC cutoff.
For group comparison we used t test for continuous variables if normally distributed and the Mann-Whitney U test if not normally distributed, and chi-squared test for categorical variables.
Cumulative probability plots were drafted for annual change in mTSS for the periods 0–2, 2–5, 5–10, and 2–10 years.
We used unadjusted and adjusted linear regression analysis (enter procedure) to look for baseline predictors of change in mTSS for the periods 0–2 and 0–10 years. Tested baseline variables with a p value < 0.20 in unadjusted analyses were tested in adjusted analysis.
Unadjusted and adjusted linear regression analysis was also used to explore for associates with change in mTSS for the periods 0–2 years, 2–10 years, and 0–10 years. Tested variables included mean values for disease activity measures and PRO for the periods and treatment used in the periods. We adjusted for baseline predictors, which in unadjusted analysis were found to be significantly associated with change in mTSS for the periods 0–2, 2–10, and 0–10 years.
Statistical tests were performed using PASW Statistics 18 (IBM SPSS statistics). Significance level was p < 0.05.
Ethical and legal aspects
The study was approved by the regional committee for ethics and medical research in Norway (REK-S-98093). All patients gave written informed consent before inclusion.
RESULTS
Patients and disease measures
A total of 94 patients with RA (36 men and 58 women; 91 white and 3 Asian) were included. Baseline mean age was 50.4 years, BMI 25.9 kg/m2, and time from symptom onset to inclusion was 12.3 months. At baseline, 37.6% were current smokers and 67.8% were RF-positive. Among those tested during followup for ACPA (n = 83), 66.3% were positive. Further, among the 76 patients with RA who at baseline had radiographs performed, erosions were present in 53 patients (69.7%). Among the 94 included patients, all had a 2-year visit, but 2 patients had no visit at 6 months. In the period between the 2-year and 5-year visit, 3 patients had died and 2 did not want to come to further study visits. One patient with a final 10-year visit had not had a visit at 5 years. In the period between the 5-year and 10-year visits, 5 patients had died, 1 had moved from the hospital area, 1 had developed dementia, and 7 did not want to come to further study visits.
In Table 1, measures of disease activity and PRO data at baseline and for the various timepoints of followup are displayed.
Disease activity and health status in patients with early rheumatoid arthritis who were followed for 10 years. Continuous variables with normal distribution are presented as mean (SD). Variables with non-normal distribution are also presented as median with interquartile range [IQR]. Categorical variables are presented as n (%). Numbers vary from the number of participants at the visits because of missing values.
As shown in Table 1, joint pain and MHAQ improved significantly in the first 6 months and flattened out for the rest of the period, whereas the same pattern was seen after the 2-year visits for ESR. For CRP, swollen 28 and tender 28 joint counts and DAS28-ESR3 all showed numeric decreases during the followup period. During the study period, the prevalence of patients with no swollen 28 joint count was at baseline 1.1%, at 6 months 12.0%, at 2 years 33.0%, at 5 years 41.4%, and at 10 years 63.5%, and the corresponding values for no tender joints were 5.3%, 15.2%, 29.8%, 39.1%, and 55.4%, respectively.
Figure 1 shows the percentage of patients with RA in remission, and low, moderate, and high disease activity as defined by DAS28-ESR3 cutoff levels at the visit timepoints.

Percentage of early rheumatoid arthritis patients in remission, and low, moderate, and high disease activity status at baseline, 6 months, and 2, 5, and 10 years of followup visits. Disease activity status groups are defined by the disease activity score (calculated from 28 swollen and 28 tender joint count, and erythrocyte sedimentation rate) cutoff levels.
Radiographic joint damage
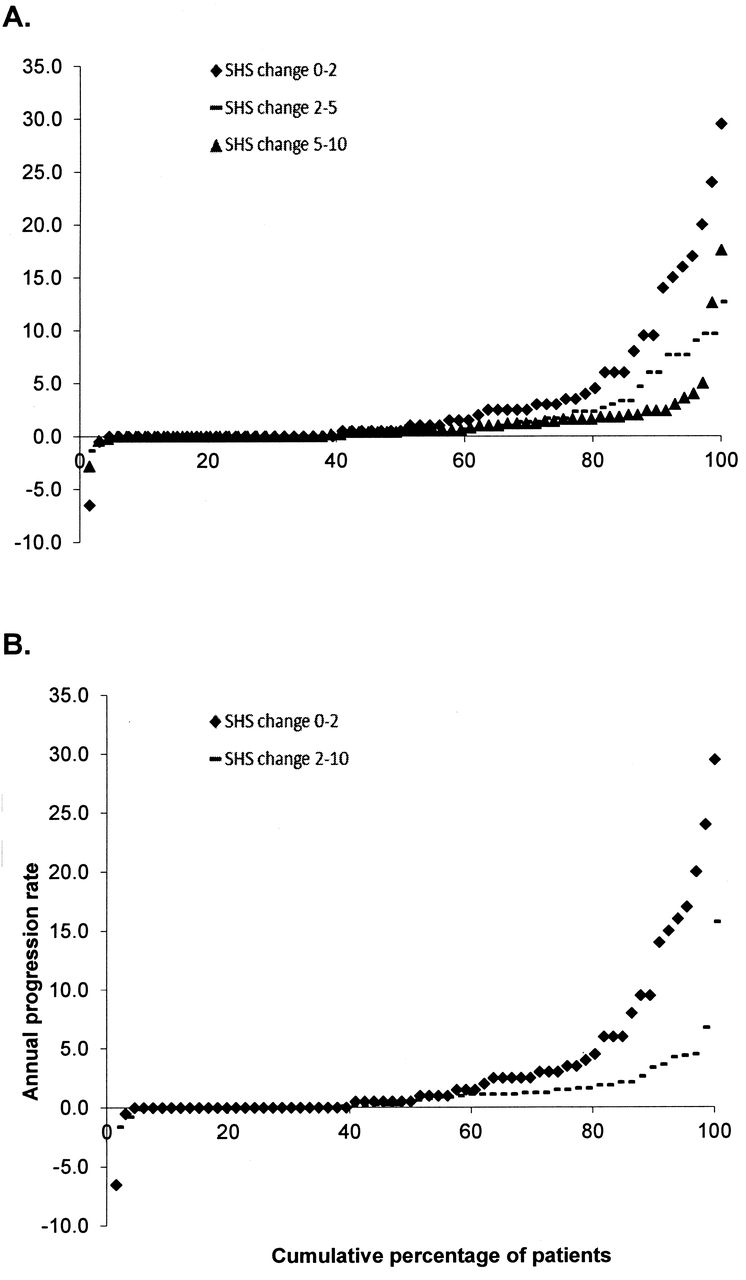
As shown in Table 2, radiographic joint damage significantly increased between all timepoints. In Table 2 and Figure 2, annual change in mTSS for different periods is displayed. A statistically significant difference was seen between annual change in mTSS between 0–2 years and the periods 2–5 years, 5–10 years, and 2–10 years. No significant difference was seen between the periods of 2–5 years and 5–10 years. The same pattern was seen when only patients with radiographs at all timepoints were included in the analysis (data not shown).
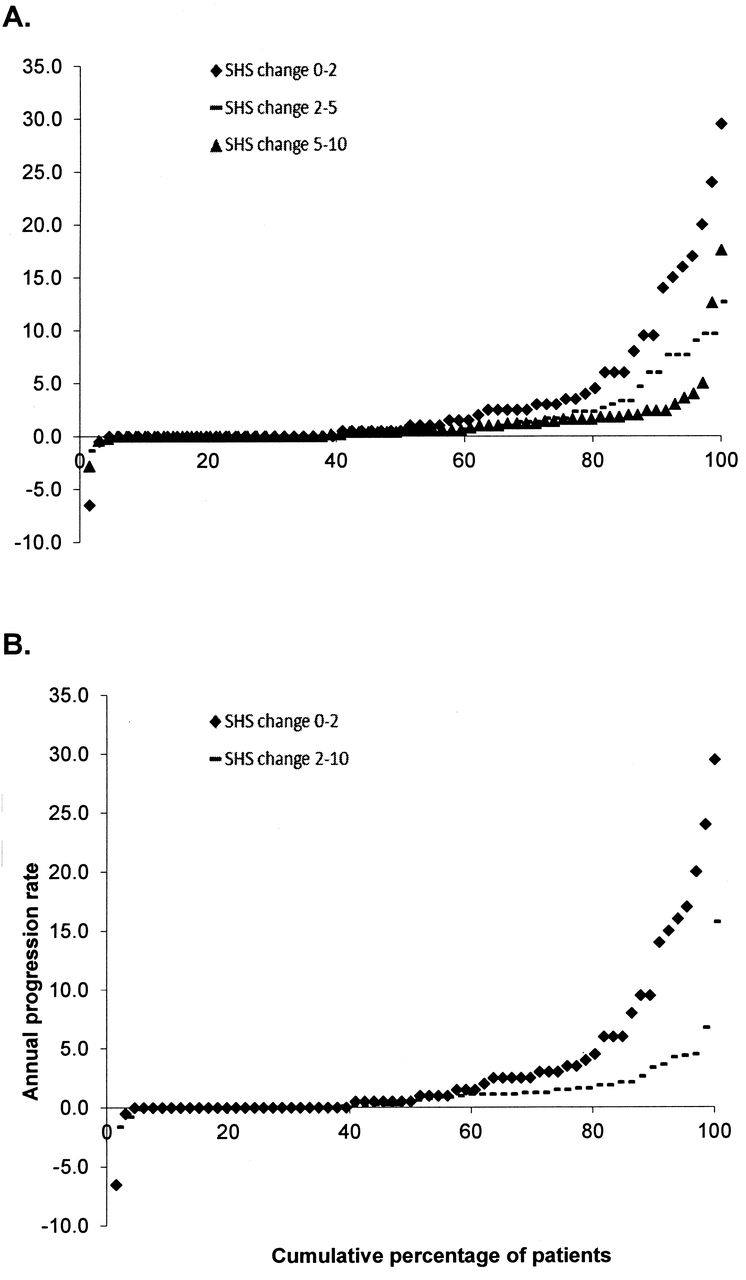
Cumulative probability plots presenting the individual early rheumatoid arthritis patients’ annual change in modified total Sharp score (mTSS; SHS). A. Periods 0–2, 2–5, and 5–10 years. B. Periods 0–2 and 2–10 years.
Modified total Sharp score (mTSS) at baseline and followup visits and annual changes in mTSS for the followup time periods in patients with early rheumatoid arthritis followed for 10 years.
In Table 2, the percentage of patients with annual radiographic progression exceeding various cutoffs is shown. The percentage of patients with increase in mTSS > SDC was for the periods 0–2, 2–5, 5–10, and 2–10 years 19.7, 13.0, 4.3, and 3.5%, respectively.
Treatment
Table 3 shows the percentage of patients with RA using prednisolone, and synthetic and bDMARD in monotherapy or in various combinations at the specific visits. The percentage of patients receiving no treatment was higher at the 5- and 10-year visits than at 6 months. For patients receiving no treatment, DAS28-ESR3 declined from 3.95 at 6 months to 3.47, 3.11, and 2.43 at the 2-, 5-, and 10-year visits, respectively.
Percentage of patients with early rheumatoid arthritis taking prednisolone and synthetic and biologic disease-modifying antirheumatic drugs (DMARD) at specific visits. Figures are shown as n (%) unless otherwise specified.
All patients who had been treated with bDMARD during followup had used TNF inhibitors. In the period of 2–5 years, 1 patient also had tried anakinra and in the period 5–10 years, 4 had tried rituximab and 3 tocilizumab.
In patients using methotrexate (MTX) at the followup visits, the mean (SD) dosage at 6 months, and 2, 5, and 10 years was 13.6 (4.0), 13.7 (3.9), 14.6 (3.5), and 14.4 (3.1) mg/week, respectively.
For the period 0–2 years, 62.8% had used prednisolone, 91.5% synthetic DMARD, and 18.1% bDMARD. The corresponding numbers for the period 2–10 years were 50.6% for prednisolone, 89.3% for synthetic DMARD, and 62.7% for bDMARD. The percentage of patients who had received GC in any form was 83.0% for the period 0–2 years and 82.7% for the period 2–10 years. Only 2 patients had not been treated with prednisolone, synthetic, or bDMARD during followup; however, they had been treated with other drugs, e.g., with non-oral administration of GC.
For cumulative prednisolone use, the median (IQR) dose was 2.9 g (3.6) for the period 0–2 years and 2.9 g (8.6) for the period 2–10 years, and cumulative doses for any GC used transformed into prednisolone equivalent doses were 2.8 g (7.4) and 1.7 g (11.30), respectively.
The mean daily doses of prednisolone for the period 0–2 years 3.9 mg (2.9), and for the period 2–10 years 1.8 mg (1.9), and daily doses for prednisolone equivalent for any GC for the periods median 3.8 (IQR 9.7) and median 0.8 (3.7) mg/day, respectively.
Predictors and associations with radiographic joint damage
In Table 4 the results from unadjusted and adjusted linear regression analysis for baseline predictors and associations with change in radiographic joint damage are shown.
Unadjusted and adjusted linear regression analyses between baseline characteristics, mean measures, treatment, and annual change in modified total Sharp score (mTSS) in patients with early rheumatoid arthritis followed for 10 years, for the periods 0–2, 2–10, and 0–10 years. Data are presented with unstandardized beta (B) and p values.
DISCUSSION
To our knowledge, this is the first study providing longterm data on clinical and radiographic outcome in patients with early RA diagnosed and followed in the first decade of the biologic treatment era. Patients had a favorable longterm outcome both for measures of disease activity, PRO, and radiographic damage. During the 10-year followup period, mean DAS28-ESR3 was reduced from high disease activity at inclusion (5.2) to a mean value of 2.7, which is close to the remission cutoff (2.6). Expressed in European League Against Rheumatism disease activity categories, only 5% were in remission or had a status of low disease activity at inclusion, whereas at 10 years this proportion was 73%, and none of the patients had a status of high disease activity. This improvement during followup (Table 1) was also seen for other measures reflecting disease activity, both laboratory markers (CRP and ESR) and clinical measures (28 joint count). For joint pain and MHAQ, a significant improvement was seen only for the first 6-month period; thereafter, no significant change occurred. This is in contrast to disease activity measures that during followup showed improvement beyond the 6-month visit (Table 1). However, what should be emphasized is that about 35% of the patients with RA at the 10-year visit still had ≥ 1 swollen joint, indicating active disease. This highlights the need for further improvements in treating patients with RA, even in the new treatment era of bDMARD.
Improvement in disease activity measures for patients with RA in the first decade of the new millennium was also reported from the NORwegian Disease-Modifying Anti-Rheumatic Drug (NOR-DMARD) register19. From this register, about a 2-fold increase in 6-month remission rates was observed in MTX-treated patients (from 17.8 to 37.6%) as well as MTX + TNF inhibitor–treated patients (16.9 to 46.3%) in the period 2000–2010.
Early intervention has in several studies been shown to be a critical prognostic factor for both clinical and radiographic outcome in RA20,21,22,23, proving the concept of “window of opportunity,” which was first hypothesized in the early 1990s24. The prognostic importance of early aggressive treatment has been shown to be of particular importance for ACPA-positive patients with RA20,25,26. In our study, the time from symptom onset to inclusion was 12.3 months, which in 1999 and 2001 was considered early. Patients included in our study all fulfilled the old ACR 1987 revised classification criteria for RA15, and 70% had erosions on radiographs. In very early arthritis cohorts the presence of erosive disease in patients with RA has been reported as low as 16–25%20,25 and in a cohort of probable RA as low as about 5%25.
During the last decades, the effect of a treat-to-target strategy compared with ordinary clinical care on a favorable clinical and radiographic outcome in RA has been proven both in randomized controlled studies27,28 and in ordinary clinical care29,30,31. In the Dutch RA Monitoring remission induction cohort study, where the objective was to develop, implement, and evaluate a treat-to-target strategy aimed at achieving remission in very early RA (symptom duration < 1 yr) in daily clinical practice, 47% achieved DAS28 remission at 6 months and 68% at 12 months followup30. This treat-to-target strategy has also been shown to be cost-effective27,32 and feasible for daily clinical practice33. Further, a sustained beneficial effect has also been shown in patients with RA followed by the treat-to-target strategy31. The patients with RA in our study were not followed by a treat-to-target strategy but were treated according to the doctors’ overall clinical judgment. However, during the last decade there has been an increasing tendency among rheumatologists in Norway to use the treat-to-target strategy as part of standard clinical care.
In patients now diagnosed with RA, we could expect the prognosis to be even better than that shown in our patient cohort. The importance of this is further emphasized by a recent subanalysis from the FIN-RACo trial, showing that physician adherence to the tight control treatment strategy is important to achieve remission and maintain work capability in patients with early RA34.
Our data suggest that the favorable outcome is attributed to the aggressive treatment in our patient cohort, with a large proportion of patients treated with prednisolone, synthetic DMARD, and bDMARD, as monotherapy or in various combinations (Table 3). The high proportion of patients using TNF inhibitors in our study, which from the 6-month visit increased from 4.3% to 52.0% at 10 years, may partly explain the lower rate of annual increase in mTSS in the periods 2–5 and the 5–10 years, compared with the 2 first years of followup. In our study, the proportion of patients with RA using TNF inhibitor monotherapy was 13.3% at the 10-year visit. This may have limited both the clinical and radiographic outcomes in our study. Despite encouraging data on triple combination treatment in the FIN-RACo study from 1999, only a small proportion of our patients with RA were taking triple combination treatment35.
In contrast to clinical registry data, there is a lack of registry data for radiographic joint damage. From the Danish DANBIO register, patients with RA who were treated with TNF inhibitors (median 1.5 yrs) had a lower rate of increase in radiographic damage score when compared with the previous period, when they were treated with synthetic DMARD (median 2 yrs)13. In that study, the annual median radiographic progression rate decreased significantly from 0.7 (IQR 0.0–2.9) in total Sharp score units in the DMARD period to 0.0 (0.0–0.9) units in the TNF-inhibitor period, and the corresponding mean values were 2.1 and 0.7 (p < 0.0001). In our study, the mean annual increase in annual mTSS was 3.4 in the first 2 years and 1.7 in the period 2–5 years and 1.2 in the period 5–10 years, whereas the median values were 0.8, 0.3, and 0.6, respectively.
What also should be emphasized is that the proportion of smokers (37.6%) seems high in our cohort compared with other studies. In the large multinational QUEST RA database, 15% were reported to be current smokers36. In a hospital population–based RA study, 24% were found to be current smokers in Norway and 15% in Finland37. Data in the literature suggest that smoking can weaken the effectiveness of RA medication38,39 and RA may be more severe in smokers than nonsmokers40. Smoking cessation as a nonpharmacological intervention may also be a strategy to reduce the burden of RA disease.
In the literature there are numerous articles searching for predictors or associations with joint damage in RA41,42. Consistently, markers of inflammation (e.g., ESR and CRP), RF, and/or ACPA, and erosions have been reported to be strong predictors of progression in radiographic joint damage in RA41,42. In our study we found that only baseline mTSS and mean values of laboratory inflammatory markers (ESR and CRP) for the period 0–2 years were associated with increase in mTSS the first 2 years of followup. Mean CRP for the period 2–10 years, and mean increase in mTSS for the period 0–2 years, were independently associated with an increase in mTSS for the period 0–2 years. However, when searching for independent predictors or associations with increase in mTSS for the whole 10-year period, the following variables were identified: baseline mTSS, mean CRP for the period, and RF, overall confirming results from previous reports.
Our study has several limitations. The number of patients is rather small and patients were recruited from only 1 outpatient clinic. Another limitation is the missing radiographic data. Lack of standardization of treatment during followup also makes it difficult to explore for associations. Further, the time periods between the visits were not equal, a major limitation when calculating mean values for disease activity and PRO measures for followup periods. Despite all the limitations, our study reflects the clinical outcome in a group of early patients with RA treated in an ordinary daily clinical practice with easy access to bDMARD in the new millennium.
Our study shows that patients with RA diagnosed in the new millennium can expect to have a favorable clinical and radiographic longterm outcome. This outcome probably could have been better if our patients had been treated earlier and treated consistently according to the treat-to-target recommendations3.
It is therefore the responsibility of each rheumatologist and rheumatology clinic to offer each patient with RA the best care and the best prognosis based on current knowledge by implementing early aggressive treatment strategies and by monitoring patients with early RA with a treatment target of remission. In patients with RA in the new millennium, both clinical remission and a status of low progression in radiographic damage can be achieved.
Acknowledgment
We gratefully acknowledge the expert technical assistance and help with data collection from Hege Sommerseth, Bodil Bjørnebye, Torun Dahl, Lise Nordheim Hoel, and Solvor Bergesen. Further, we thank statistician Are Pripp for his statistical advice.
Footnotes
Supported by an unrestricted grant to Martina Hansens Hospital from Pfizer Norway.
- Accepted for publication August 14, 2015.








{kind=link}
{kind=link}