

Abstract
Objective. To describe early radiographic findings in patients from the Swedish psoriatic arthritis (SwePsA) registry, progression of destruction, correlations with clinical disease variables, and predictors of destruction.
Methods. Hand and foot radiographs were available for 72 of 197 SwePsA patients followed for 5 years. Clinical data were collected according to the SwePsA protocol.
Results. Disease characteristics and clinical improvement were similar in men and women. Radiographic abnormalities were more pronounced in men. Total Wassenberg radiographic score at baseline was 0 in 45% of men and 51% of women. One man and one woman had a score > 10. At 5 years, total score was 0 in 14% of men and 40% of women (p = 0.018); 17% of men and 7% of women had scores > 10. Mean total scores for men and women had increased. Baseline erythrocyte sedimentation rate was associated with baseline total radiographic score. In men, swollen joint count was positively, and in women tender joint count negatively, correlated to total radiographic score. After 5 years, only male scores, mainly hand scores, significantly correlated with 28-joint Disease Activity Score and Disease Activity Index for Psoriatic Arthritis scores, swollen joint count, and dactylitis. Achieving remission or minimal disease activity after 5 years protected against structural damage, mainly in men.
Conclusion. Radiographic progression in early PsA was generally slow but substantial. Male sex appears to be a risk factor for early radiographic damage while the presence of baseline radiographic damage and dactylitis developing during followup seem to predict further destruction. Hand and foot radiograph scoring cannot be substituted with clinical signs.
The psoriatic disease complex consists of skin psoriasis, psoriatic arthritis (PsA), and psoriatic nail disease1. This heterogeneous disorder has highly variable patterns of joint and skin disease of varying degrees of severity. In southern Sweden, 18% of patients with psoriasis also have arthritis, and the local prevalence of PsA is 0.34%2. The joint disease spectrum ranges from mild monoarthritis or oligoarthritis to very severe erosive and destructive polyarthritis. Several disease subsets have been defined based on joint involvement3,4. The clinical picture may change spontaneously with time or after treatment with disease-modifying antirheumatic drugs (DMARD)4. The medical profession is increasingly aware of PsA being associated with musculoskeletal morbidity, resulting in reduced health-related quality of life5, as well as an association with an increased prevalence of comorbidities common to psoriasis, such as cardiovascular disease and metabolic syndrome, and premature death. Osteoporosis and an increased risk of severe infection must also be considered6.
The disease burden of PsA was recently estimated to be as significant as or even greater than the burden of a number of other chronic diseases, including other inflammatory arthritic diseases5, where the risk of lymphoma is increased in rheumatoid arthritis (RA) but only slightly increased in PsA7. In PsA, the early detection of inflammatory peripheral or axial joint involvement may be important to reduce inflammation and prevent destruction, deformity, and functional disability in affected joints. Only a few studies have focused on the radiographic appearance of early PsA4,8,9, reporting high rates of destruction in early disease and showing the importance of imaging in the followup of these patients. Haroon, et al10 evaluated the rate of progression of joint damage in a cohort of patients with disease duration of more than 10 years and found that even a delay of 6 months from the onset of symptoms to the first consultation can lead to the development of more joint erosion and worse longterm physical function. The same study found significantly less frequent drug-free remission and more frequent arthritis mutilans among patients presenting more than 1 year after symptom onset. The authors concluded that adverse clinical, radiographic, quality of life, and physical function outcomes occur early in the course of the disease, and that early diagnosis and treatment is vital for improved outcomes10.
The Swedish Early PsA (SwePsA) registry11,12,13 was established in 2000 to enable studies on early PsA in the Swedish population; to evaluate the course of the disease, socioeconomic issues, and workforce participation; to identify markers of disease progression; and to describe treatment patterns and effects in real-life care. Detailed clinical evaluations from the 5-year followup have been13,14,15,16 and will be published elsewhere. The purpose of the current report is to describe the early radiographic findings in patients with PsA included in the SwePsA registry using the Wassenberg17 score to evaluate the progression of structural damage from diagnosis to the 5-year followup, evaluate patients without progression, analyze correlations with clinical disease variables in early PsA, and identify predictors of progressive destructive joint disease.
MATERIALS AND METHODS
In a prospective study approved by the ethics committee at Uppsala University, patients with early PsA were enrolled for longterm followup. The patients were from 6 rheumatology clinics in Sweden, to cover different genetic backgrounds and climates. The population and detailed enrollment process were described previously11,12,13, and patient inclusion and exclusion in the current report was as previously reported13, but with additional exclusions for missing radiographs (Figure 1).
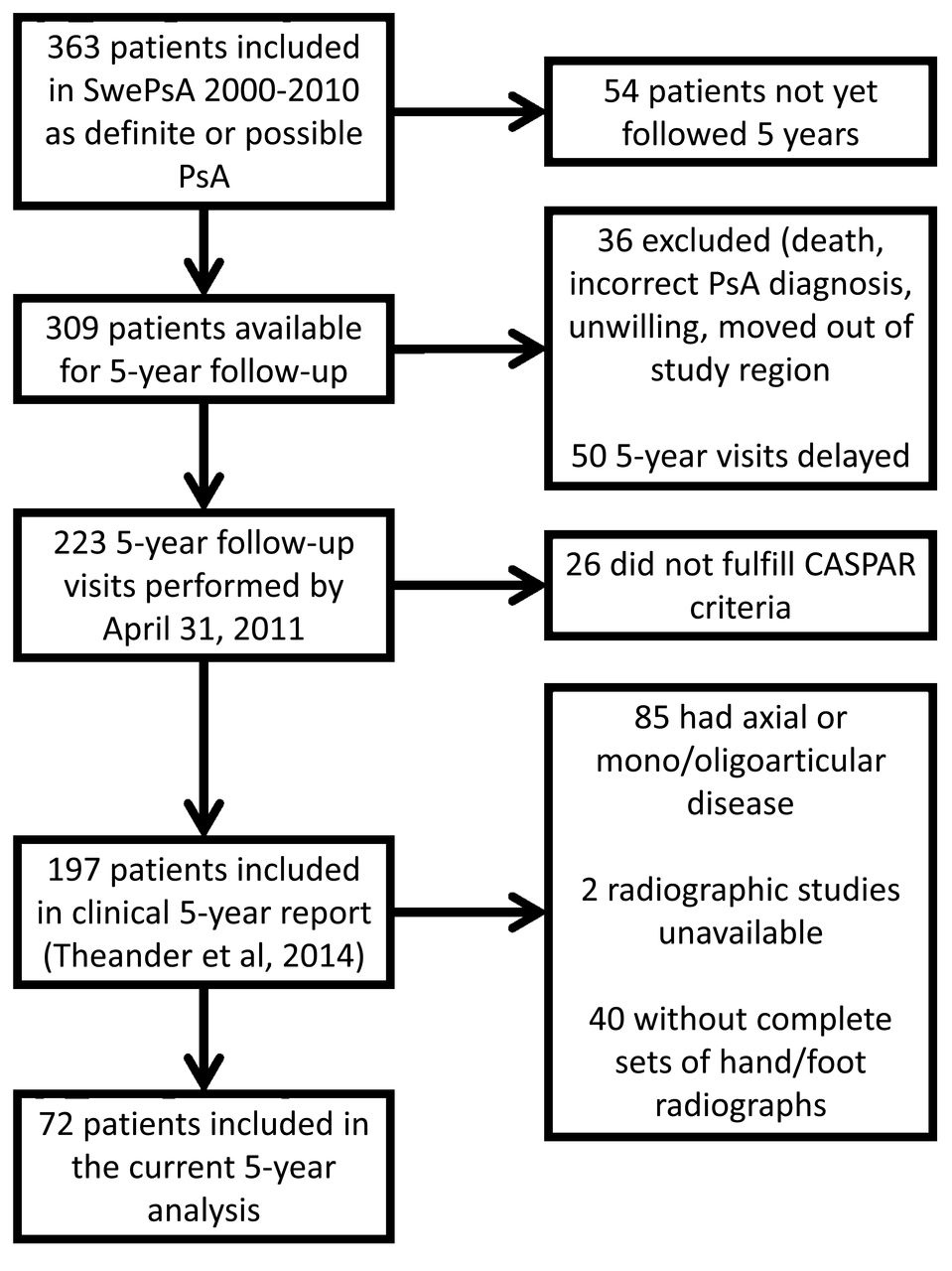
Flow chart of patient enrollment in the Swedish Early Psoriatic Arthritis Registry (SwePsA). PsA: psoriatic arthritis; CASPAR: ClASsification for Psoriatic ARthritis criteria.
According to the SwePsA protocol, hand and foot radiographs were taken for polyarticular disease or when those joints showed signs of inflammation at baseline, and radiography was repeated at followup. Clinical data were collected according to the SwePsA protocol, with disease activity measured by the research team at each center using the Disease Activity Score for 28 joints (DAS28)18 and the Disease Activity Index for Psoriatic Arthritis (DAPSA) score19,20 [calculated as the swollen joint count (SJC) of 66 joints + tender joint count (TJC) of 68 joints + patient global assessment visual analog scale (VAS; in cm) + pain VAS (in cm) + C-reactive protein (CRP; in mg/dl)]. Correlations between the DAS28 and DAPSA score, their component items, function, Psoriasis Area and Severity Index (PASI), radiographic scores, and progression were analyzed.
Digital radiographs were evaluated using a clinical picture archiving and communications system with high-resolution monitors. At 1 center, imaging was performed with an analog film-screen technique until early 2011, after which a digital imaging system was installed. In the other centers, digital imaging was provided by the local radiology departments for most of the study period. Analog films were scored using a conventional light box and magnifying glass when necessary. Some analog films were scanned locally into digital format with a commercially available radiograph film scanner.
Radiographs were scored according to the Wassenberg/Ratingen scoring system for PsA17 by a musculoskeletal radiologist with 23 years’ experience in arthritis imaging and blinded to all clinical variables (Table 1). Images were mostly scored in chronological order; for practical reasons, such as delayed delivery of radiographs for reading, this was not always possible. The availability of complete 5-year hand and foot radiographs was mandatory for inclusion in the current analysis. When baseline radiographs were missing but 2-year radiographs with score 0 were available, baseline radiographic scores were imputed as a score of 0 (i.e., no progression between baseline and 2-year followup).
Wassenberg psoriatic arthritis score. In the Wassenberg scoring system, all distal and proximal interphalangeal joints in the hand, metacarpophalangeal joints, the wrist (30 joints), interphalangeal joint 1 in the feet, and metatarsophalangeal joints 2–5 were scored for destructive and proliferative changes typical of PsA. A total of 40 joints are scored, with a possible total score of 0 to 360. The hand score accounts for 75% of the maximum17. From Wassenberg, et al, Z Rheumatol 2001;60:156–66; reproduced with permission from Springer-Verlag Berlin Heidelberg.
Statistical analysis
Descriptive statistics were used to report relevant demographic and clinical features, as well as radiographic findings. Data at inclusion and the 5-year followup were compared using paired t tests. Subgroups of patients were compared by chi-square and t tests. Correlation analysis between measures and variables was performed using the Spearman rank test because of the skewed distribution of the radiographic scores. To analyze predictors of radiographic outcome and progression between baseline and 5-year followup, univariate and multivariate linear regression and logistic regression were performed and the results expressed as β or OR with p values and 95% CI. These variables were used as potential predictors based on earlier results and published data: sex, baseline age, symptom duration before inclusion, disease activity (DAS28 or DAPSA), joint counts, presence of dactylitis, tenosynovitis, or enthesitis, Health Assessment Questionnaire (HAQ), skin and nail psoriasis, and patient-related measures such as pain and global disease assessment. Calculations were performed in the Statistical Package for Social Sciences (SPSS) for Macintosh, version 21.
RESULTS
In 72 patients [29 men (35%) and 43 women (38%)] with PsA fulfilling the ClASsification for Psoriatic ARthritis (CASPAR) criteria21, the mean (SD) age at inclusion was 47.8 (14.7) years (range 21.0–80.4 yrs) for the entire cohort; 46.4 (14.5) years (range 24.3–77.8 yrs) for men, and 48.7 (15.0) years (range 21.0–80.4 yrs) for women (p = 0.52). As a result of the radiography protocol in SwePsA, the majority of patients with available hand and foot radiographs had polyarticular disease. No patients had arthritis mutilans or axial disease only, and 3 men and none of the women had combined axial and peripheral disease (Table 2). Radiographs of both hands and feet were available for 26 patients at baseline and 5 years, for 16 patients at 2 and 5 years, and for 30 patients at all 3 timepoints.
Patient and clinical disease characteristics at baseline and at the 5-year follow-up in 72 patients with early psoriatic arthritis.
The median symptom duration at inclusion was 12 months and was only slightly longer in men than in women (p = 0.52). Details about DAS28, DAPSA, HAQ, PASI, joint counts, VAS scales, and other disease-specific information are reported in Table 2. Apart from higher HAQ in women and more frequently detectable skin psoriasis in men, there were no significant differences between men and women at baseline.
Radiographic scores
No correlation was found between age at baseline and the total destruction score at inclusion (p = 0.13) or 5 years (p = 0.20). At baseline, 35 patients (49%, 95% CI 37%–60%) had no PsA-related radiographic changes [score 0; mean score 2.2, SD 3.3, range 0–22; men: n = 13, 45% (95% CI 26%–64%); women: n = 22, 51% (36%–67%); Table 3].
Wassenberg score17 at baseline and at the 5-year followup in 72 patients with early psoriatic arthritis. Data are n (SD), except for Score 0, which are n (%). * indicates significant p values.
Only 1 man and 1 woman had scores > 10. For men and women, the mean (SD) total scores at baseline were 3.2 (4.1) and 1.6 (2.5; p = 0.018); erosion scores 1.2 (2.3) and 0.3 (0.88; p = 0.025); and proliferation scores 1.9 (2.4) and 1.3 (2.0; p = 0.23), respectively. Foot scores at baseline were 1.04 (1.8) and 0.28 (0.74; p = 0.016) and hand scores 2.2 (3.2) and 1.3 (2.4; p = 0.16) for men and women, respectively. Thus, men had significantly greater radiographic damage than women. Although the foot scores contributed to 38% of the total score in men and 28% in women, the difference was not significant.
At 5-year visit, the median total score (Table 3) had increased significantly (p < 0.001) to 3 (mean 5.3, SD 8.7, range 0–60). The score was still 0 in only 21 patients [29%; men: n = 4, 14% (95% CI 0–27); women: n = 17, 40% (95% CI 24–55); p = 0.018]. Five men (17%) and 3 women (7%) had scores > 10. The mean total score was significantly higher in men than in women [8.0 (SD 12.0) vs 3.4 (SD 4.8), p = 0.027]. The mean (SD) erosion scores were 3.4 (8.2) and 0.86 (1.7; p = 0.051) and proliferation scores 4.6 (4.9) and 2.6 (3.5; p = 0.045) for men and women, respectively, at 5-year followup. Foot scores at 5-year followup were 2.5 (3.9) and 0.84 (2.1; p = 0.028) and hand scores 5.6 (8.5) and 2.6 (3.7; p = 0.047) in men and women, respectively. In men the foot scores contributed to 32% of the total score and in women 25%, but the difference was not significant.
Baseline and 5-year scores were highly correlated (for total scores: Spearman ρ 0.752, p < 0.001).
Correlations between baseline radiographic scores and clinical features
At baseline the total Wassenberg score correlated with erythrocyte sedimentation rate (ESR; ρ 0.27, p = 0.027). The SJC was significantly associated with total score (ρ 0.395, p = 0.034) and total hand score (ρ 0.425, p = 0.022) in men, but not in women. In contrast, the TJC was inversely associated with total score (ρ −0.330, p = 0.031) in women, but not in men. Current smokers did not present with higher scores than nonsmokers (2.2 vs 2.2, p > 0.05). Polyarticular disease at baseline was not associated with higher radiographic scores at baseline (2.5 vs 2.0, p > 0.05). Detectable skin psoriasis and nail psoriasis was associated with numerically, but not significantly, higher scores (2.4 vs 1.9 and 2.8 vs 2.0). Presenting with tenosynovitis (n = 18) was associated with significantly higher radiographic scores [3.8 (SD 4.7) vs 1.7 (SD 2.6), p = 0.021], which was also true in women [3.1 (SD 3.9)] with tenosynovitis vs 1.1 (SD 1.8) without tenosynovitis (p = 0.026) but not men [4.6 (SD 5.7) vs 2.7 (SD 3.3), p = 0.26]. In contrast, the presence of enthesitis, especially in the hip and heel region, was associated with lower radiographic scores at baseline [0.87 (SD 1.8) with peripheral enthesitis vs 2.8 (SD 3.7) without peripheral enthesitis, p = 0.024]. The significant association was not present when evaluating men and women separately. Dactylitis was present in 21 (30%) of the patients at baseline but was not associated with higher radiographic scores at this timepoint.
After 5 years total radiographic score and hand score correlated with SJC (ρ 0.278, p = 0.020 and 0.304, p = 0.020). In men, TJC also exhibited a trend of being associated with radiographic damage (ρ 0.387, p = 0.054 for total score). Disease activity, measured by the DAS28 and DAPSA scores, correlated with radiographic scores only in men, mainly in the hands. Tenosynovitis and enthesitis were not associated with radiographic scores. Dactylitis was associated with worse radiographic outcome only in men (total radiographic score: ρ 0.547, p = 0.002; hand score: ρ 0.491, p = 0.007; foot score: ρ 0.400, p = 0.032). The 7 men with dactylitis at 5 years had a high mean score of 10. Patients in remission (no swollen or tender joints and normal ESR and CRP) at 5-year followup (n = 10) had accumulated less radiographic damage [2.7 (SD 2.5) vs 6.3 (SD 10.2), p = 0.033]. Male patients achieving minimal disease activity (MDA) according to Coates, et al22 (n = 10) clearly had less damage because the mean (SD) total score was 3.4 (2.99) in those with MDA versus 10.94 (14.36) in those not achieving MDA (p = 0.045). Hand scores were significantly lower in men with MDA (p = 0.042) than in men not achieving MDA. No difference between MDA and non-MDA was found in women.
Predicting radiographic outcome
Only 4 men (14%, 95% CI 0–27) and 17 women (40%, 95% CI 24–55) showed no signs of radiographic damage at 5-year followup (Wassenberg score ≤ 1). Thus, male sex was a risk factor for structural abnormality (OR 4.09, 95% CI 1.2–13.8, p = 0.024). Baseline and 5-year scores were highly correlated, and radiographic changes at baseline predicted further radiographic damage at followup (OR 3.4, 95% CI 2.2–5.2, p < 0.001). In age-adjusted univariate linear regression analysis, these factors significantly predicted higher 5-year radiographic scores: baseline radiographic scores, male sex, presenting with tenosynovitis at baseline, and having been treated with methotrexate (MTX; Table 4). However, in multivariate analysis, only the baseline score remained significant, explaining 64% of the total score at 5 years. In contrast, further damage was not predicted by the DAS28, SJC, TJC, HAQ at baseline, months of delay, patient age, smoking at baseline, or any enthesitis or dactylitis at baseline (Table 4).
Univariate and multivariate linear regression analysis of 5-year data for all patients (n = 72), and for men and women separately.
Five-year radiographic results were not influenced by medication, other DMARD (except MTX), or the use of biologics. However, none of the 15 patients with the highest scores/most progression had received tumor necrosis factor blockers; all but 1 had been treated more or less continuously with MTX during the 5-year followup.
DISCUSSION
Radiographic destruction is an important outcome variable in clinical trials of RA and PsA. Results from our current study indicate that men improve clinically but develop radiographic changes, whereas women show less clinical improvement, especially in HAQ and TJC, but do not develop joint damage to the same extent as men. The only independent predictors of a high radiographic score at followup were elevated radiographic score at baseline and presenting with dactylitis at 5-year followup. The SJC correlated with radiographic scores, especially hand scores, primarily in men. Similarly, the DAS28 and DAPSA scores correlated with total and hand scores in men at 5-year followup. Dactylitis was also an important marker of damage, mainly in men. Patients in remission or in MDA state after 5 years had lower scores. This divergent sex-dependent behavior could be taken into consideration when planning care and treatment for patients with PsA. Women may require more interventions against functional deterioration and help coping with pain, whereas men may need followup radiography, especially in the presence of dactylitis, high disease activity, and a known propensity for radiographic destruction.
Many patients in the current study, especially women, exhibited no or very little radiographic progression. Kane, et al4 described the presentation and development of PsA over 2 years in a cohort of early PsA, demonstrating high rates of destruction in the early phase of the disease. Gladman, et al8 compared patients who had 2 years’ disease duration at the time of presentation to the arthritis clinic and those with more longstanding disease, finding that those presenting with longer symptom duration had a higher degree of damage. In that study, 39.2% of patients with early PsA presented with radiographic joint damage, compared to 49% in the current study. Queiro-Silva, et al9 studied 71 patients with early PsA over a 10-year period and found that 45% developed erosive or deforming disease by the end of the study. In that study, polyarticular disease at onset (≥ 5 swollen joints) was strongly associated with erosive disease. Similarly, Haroon, et al10 demonstrated that a delay of 6 months after symptom onset before being seen by a rheumatologist contributed to joint destruction and worse longterm physical function.
The SwePsA registry previously reported that a short delay between symptom onset and diagnosis, preserved function, and male sex are the most important predictors of a favorable clinical outcome13, and that women in general have worse outcomes with regard to clinical variables such as disease activity, pain, function, and achieving MDA13. Surprisingly, the radiographic results in the current study are discordant, in that men had higher radiographic joint scores than women, and mainly in the feet. At baseline, men presented with scores about 3 times those of female patients. The differences were also significant at 5 years.
The Wassenberg scoring system for PsA17 was selected for the current study. An advantage of the Wassenberg score is that it was specifically developed to evaluate both destructive and proliferative changes in PsA. In addition, this scoring system evaluates most hand and foot joints commonly affected by PsA (Table 1). Interphalangeal joints 2–5 in the feet are excluded from the score because they are difficult to image reliably. The Wassenberg score has a possible total score of 0 to 360; destructive changes account for 200 points and proliferative changes for 160 points. The hand score accounts for 75% of the maximum score.
In a comparison of 4 scoring systems commonly used for PsA23, the modified Steinbrocker scoring system, the modified total Sharp scoring system, the Sharp-van der Heijde modified method, and the Wassenberg scoring system were used on 50 sets of images from patients examined at 2 timepoints and read by 2 examiners. The authors concluded that none of the scoring systems were sufficiently feasible and sensitive to change to easily be applied in large longitudinal observational studies, and they could not make a clear recommendation. That study was published after most of the scoring for the current study had been performed.
Observer variation has been reported when scoring radiographs for RA24 and inflammatory changes in PsA17. In our current study, the radiographic examinations were scored in chronological order when possible. This non-random scoring order has pros and cons25, with a certain amount of expectation bias being introduced and possible overestimation of change, such as reported for scoring spinal radiographs in ankylosing spondylitis when paired scoring was preferred (the same patient’s images in unknown chronological order)26. However, chronological scoring of RA hand radiographs has been shown to increase the sensitivity for small changes between examinations, whereas a paired reading order seems to underestimate progression27.
The limitations of the current study are the small sample size due to the SwePsA protocol of performing radiography only in polyarthritic or symptomatic patients/joints. The power for detecting minor changes is lower in men because of the restricted number of male patients. The general radiographic change was modest, with most changes being technically smaller than the minimal detectable change for an individual patient17,23. In addition, the selection of patients for radiography varied somewhat because some patients underwent radiography at every visit, and some less frequently based on current clinical symptoms, probably introducing selection bias for patients with swollen and tender joints. For some patients, the analog inclusion radiographs had been destroyed or could not be located, limiting the followup time to 3 instead of 5 years, although this was overcome by imputation. Linear interpolation and extrapolation of imaging data is a well-established imputation method in both RA and PsA clinical trials28 and was done in some cases in the current study to avoid losing too many patients.
After 5 years of PsA, many patients in the current study, especially women, had no or very little joint destruction. Radiographic progression in early PsA was slow in general but substantial in men, leaving only 14% without radiographic changes at 5 years, with a high prevalence of changes in male feet. Baseline scores were the main predictor of radiographic findings at followup while the development of dactylitis may be regarded as a warning sign of possible future radiographic damage. The results in the current study suggest that for followup and treatment decisions, radiography and scoring the hands and feet at baseline are important and cannot be substituted with clinical signs, especially in men.
Acknowledgment
We acknowledge Björn Svensson for initiating the SwePsA and Gunilla Holmström for earlier fruitful cooperation and support for SwePsA.
Footnotes
Supported by independent grants from the Swedish Psoriasis Foundation and Skåne University Hospital “SUS FONDER.” An independent grant for partial support of this study was given by Wyeth (Pfizer).
- Accepted for publication July 9, 2015.








{kind=link}