

Abstract
Objective. Although there is increasing reliance on patient-reported outcomes (PRO) for disease management, there is little known about the differences in PRO across juvenile idiopathic arthritis (JIA) categories. The purpose of our study was to assess PRO across JIA categories, including pain, quality of life, and physical function, and to determine clinical factors associated with differences in these measures across categories.
Methods. This was a longitudinal cohort study of patients with JIA at a tertiary care pediatric rheumatology clinic. Subjects, PRO, and clinical variables were identified by querying the electronic medical record. Mixed-effects regression assessed pain, quality of life, and function.
Results. Subjects with enthesitis-related arthritis (ERA) and undifferentiated JIA had significantly more pain, poorer quality of life, and poorer physical function. The ERA and undifferentiated JIA categories, physician’s global disease activity assessment, female sex, and nonsteroidal antiinflammatory drug use were significantly associated with more pain, poorer quality of life, and poorer function. In models limited to ERA, female sex and tender enthesis count were significant predictors of decreased function.
Conclusion. ERA and undifferentiated JIA categories had poorer PRO than other JIA categories. Further work is needed to address ways to improve PRO in children with JIA, with a special focus on children with ERA and undifferentiated JIA.
Patient-reported outcomes (PRO) provide insight to knowledge only known to the patient. The ability to open jars and tie shoelaces, the patient’s perception of limitations from disease, and the overall disease burden are some of the information that can be collected using PRO. Surveys of the PRO of pain, quality of life, and physical function are being increasingly used in research and have rising importance in the clinical management of pediatric rheumatologic conditions1. PRO is used by the US Food and Drug Administration for medical product labeling, the US Affordable Care Act to create the Patient-Centered Outcomes Research Institute, and the US National Institutes of Health development of the Patient-Reported Outcomes Measurement Information System. It is not uncommon for discordance between PRO and physician-reported outcomes2,3,4,5. This is not surprising because physicians and patients and their families conceptualize disease differently and value somewhat different outcomes. Thus, full evaluation of disease activity and treatment goals should include both physician assessment and parent or child reports. Despite this mounting importance, there is minimal literature on PRO, such as pain, quality of life, and physical function, across categories of juvenile idiopathic arthritis (JIA).
JIA is a group of related chronic inflammatory arthritic conditions diagnosed in children < 16 years of age. There are 7 categories of JIA defined by the International League of Associations for Rheumatology (ILAR): oligoarticular, systemic, polyarticular rheumatoid factor (RF)-positive, polyarticular RF-negative, psoriatic, enthesitis-related, and undifferentiated arthritis6. Although JIA is a group of heterogeneous conditions, many of the categories are combined for both clinical treatment guidelines7 as well as clinical trials8,9. In particular, those patients with polyarticular disease are often considered as a group regardless of distinguishing features such as the presence of RF, psoriasis, enthesitis, or sacroiliitis. Therefore, among these JIA categories, differential PRO response patterns have not been systematically evaluated.
Investigation of associated clinical characteristics with PRO are not well described across JIA categories. Prior work leveraging national cross-sectional registry data from The Childhood Arthritis and Rheumatology Research Alliance as well as several small single-center studies demonstrated that children with enthesitis-related arthritis (ERA) have more pain and lower physical function than other JIA sub-types10,11,12. However, all of these studies included limited patient-level factors.
Our study used a longitudinal cohort design to evaluate PRO. To our knowledge, ours is one of the largest studies evaluating PRO and associated patient-level clinical factors10,13. Greater understanding of PRO may lead to a better appreciation of the perspectives of young children with JIA and their parents, as well as improved disease management. The purpose of the study was (1) to characterize PRO, including pain, quality of life, and physical function in a sample of children with JIA; and (2) to determine clinical factors associated with increased pain, decreased quality of life, and decreased physical function.
MATERIALS AND METHODS
Ethical approval
The protocol for the conduct of our study was approved by the Committee for the Protection of Human Subjects at the Children’s Hospital of Philadelphia.
Study design and subjects
This is a retrospective longitudinal cohort study. Subjects were included if they were evaluated at our single tertiary pediatric rheumatology clinic between June 2010 and December 2012, had a diagnosis of JIA according to the ILAR criteria6, and had a disease duration of < 3 years. All available visits for subjects were included in the analysis. Potential subjects were identified by querying the electronic medical record for patients with a diagnosis of JIA as indicated by the International Classification of Diseases-9-Clinical Modification codes 696.x, 714.xx, and 720.x. All JIA diagnoses and category assignment were confirmed using the JIA calculator software package14.
PRO questionnaires
Pain, quality of life, and physical function were assessed at each clinic visit as part of routine clinical care. All patients were provided with paper questionnaires to complete upon entering the clinic. These paper questionnaires were reviewed by the clinician, scored, and entered into our electronic medical record. Pain over the past week was assessed with the question, “How do you rate your/your child’s pain due to his/her illness in the past week?” with an ordinal numerical rating scale (NRS). This 11-point pain scale ranged from 0 to 10 with “no pain” listed at 0 and “very severe pain” listed at 1015,16,17. Studies have shown that the ordinal scale is comparable with the 10-cm linear scale15. Quality of life was evaluated using the Pediatric Rheumatology Quality of Life scale (PRQL)18. This 10-question tool assessed quality of life over the past 4 weeks and included domains of physical health and psychological health, and had been validated for use in children with JIA in the United States19. Scores ranged from 0 to 30 with higher scores indicating worse quality of life. Physical function was estimated with the Childhood Health Assessment Questionnaire (CHAQ); this 2-page, 30-question survey assessed the 8 domains of dressing and grooming, arising, eating, walking, hygiene, reach, grip, and activities20. CHAQ scores ranged from 0 to 3 with a higher score indicating worse function. Parents rated health status by answering the question, “Considering all the ways that your rheumatic condition affects you/your child, how do you rate how he/she is doing in the past week?” using an 11-point ordinal NRS.
Physician-reported global disease activity assessment
Physician’s global disease activity assessment was reported by the physician at the end of each clinic visit as part of routine clinical care using an 11-point ordinal NRS ranging from 0 to 10, with 0 corresponding to “not active” and 10 corresponding to “very active.”
Clinical disease data collection
Demographics (sex, age at diagnosis, antinuclear antibodies, RF, HLA-B27 status) were abstracted from the electronic medical record. Clinical disease elements (active joint count, tender enthesis count) and current medication use at each visit were also abstracted from the electronic medical record. Intraarticular glucocorticoid exposure was carried forward by 1 visit to account for exposure at the prior visit.
Statistical analysis
Differences in baseline demographics and clinical characteristics were evaluated using the Kruskal-Wallis equality of populations rank test or chi-square test as appropriate. Median and interquartile range (IQR) or mean and 95% CI were used as appropriate. Less than 25% of PRO and less than 15% of physician-reported outcomes were missing in our dataset. All clinic variables, including age, disease duration, medication exposure, and physical examination findings, were complete.
Model development
We tested the association of clinical attributes with pain over time using mixed-effects ordinal logistic regression (proportional odds) with random intercepts. Quality of life (PRQL) and physical function (CHAQ) were evaluated over time using mixed-effects linear regression with random intercepts. Variables with p ≤ 0.20 in univariate analysis were included in multivariate analysis. Variables in multivariate models were considered statistically significant if p ≤ 0.05. Subject was a random effect in all models. Fixed effects examined for all PRO outcomes in univariate analysis included JIA category, physician’s global disease activity assessment, disease duration (in yrs), subject age, female sex, active joint count, nonsteroidal antiinflammatory drug (NSAID) use, systemic glucocorticoid use, disease-modifying antirheumatic drug (DMARD) use, biologic use, and intraarticular glucocorticoid use. For examination of significant features associated with pain, quality of life, and function within the ERA and undifferentiated JIA categories, fixed effects tested in univariate analysis included physician’s global disease activity assessment, disease duration (in yrs), subject age, female sex, active joint count, tender enthesis count, sacroiliac tenderness, HLA-B27 positivity (ERA only), NSAID use, systemic glucocorticoid use, DMARD use, biologic use, and intraarticular glucocorticoid use.
Severity of pain was classified into mild (> 0 to ≤ 3.5), moderate (> 3.5 to ≤ 6.0), and severe (> 6.0)21. Severity of decreased function was classified into mild (> 0 to ≤ 0.13), moderate (> 0.13 to ≤ 1.75), and severe (>1.75)22.
Correlation of physician rating with PRO
Correlation between physician’s global disease activity assessment with patient/parent rating of pain, quality of life, physical function, and health status were performed using Spearman rank correlation coefficient. Spearman ρ coefficient of < 0.4, ≥ 0.4 to < 0.7, and ≥ 0.7 indicated poor, moderate, and high correlation, respectively23. All analyses were performed using Stata 13.1 (StataCorp).
RESULTS
Patients
During the study period, there were 398 patients evaluated at 1577 visits. There were 152 patients (38%) with newly diagnosed JIA. Age and sex distribution within JIA categories were in accordance with previously published JIA cohorts10,11 (Table 1). As expected, oligoarticular JIA was the most prevalent JIA category, followed by ERA and polyarticular RF-negative. There were significant differences in pain, quality of life, and function across JIA categories (all p < 0.01). Physician’s assessment of disease trended toward significance (p = 0.06) and health status was significantly different across categories (p < 0.01).
Baseline characteristics of children with new and prevalent JIA diagnoses who are included in the study, across JIA categories in 398 JIA subjects. Values are median (IQR) or n (%) unless otherwise specified.
Pain
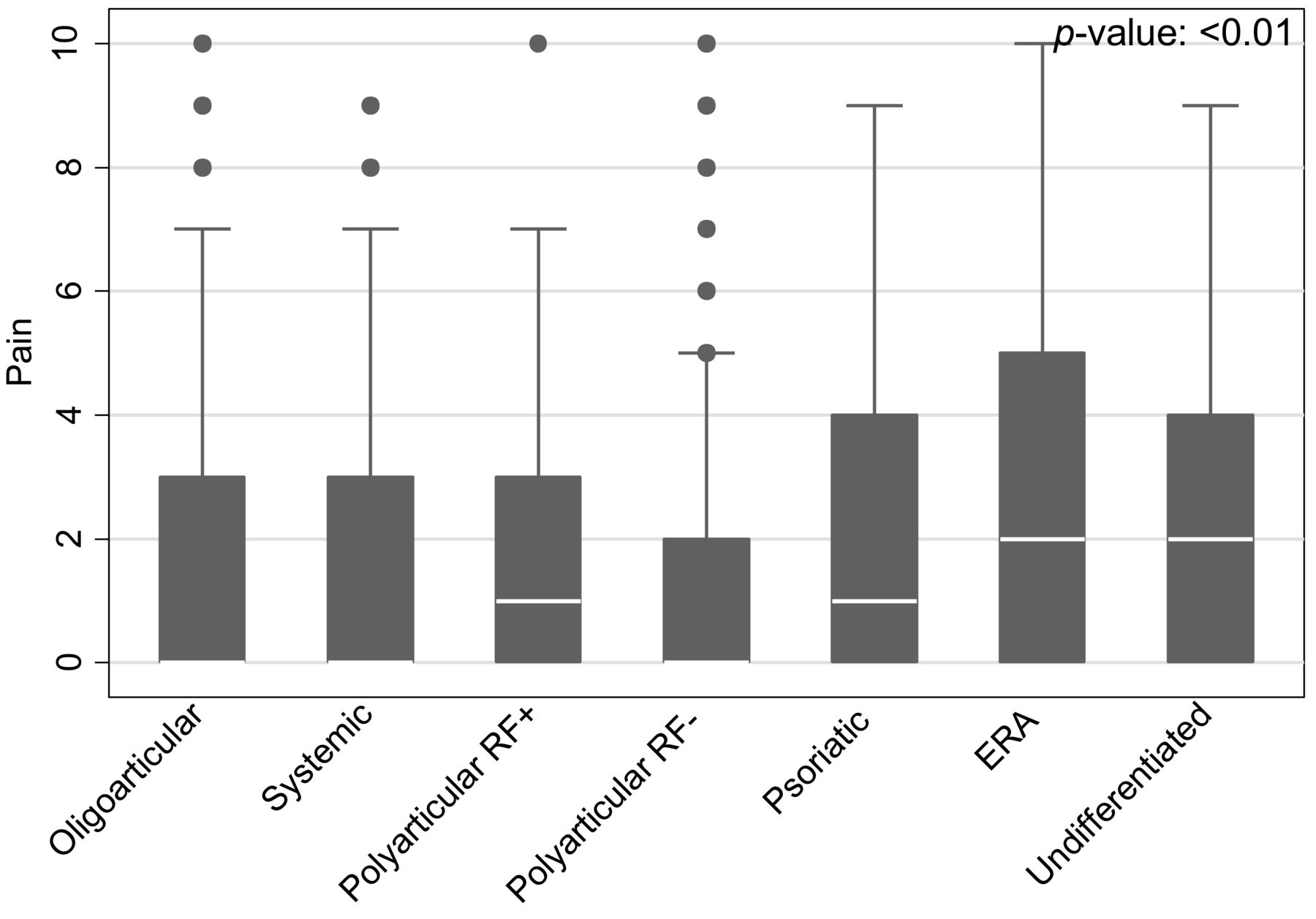
Pain prevalence and pain intensity significantly varied across JIA categories (p < 0.01). Patients with ERA and undifferentiated JIA reported a significantly higher prevalence of pain, and patients with ERA, psoriatic, and undifferentiated arthritis reported moderate and severe pain more frequently than other subtypes (p < 0.01). Median pain intensity over the past week was highest in ERA (2, IQR 0–5) and undifferentiated (2, IQR 0–4) and was lowest in oligoarticular and systemic (both 0, IQR 0–3) and polyarticular RF-negative (0, IQR 0–2; Figure 1). Statistically significant predictors of pain in a multivariate model included ERA (β 1.30, 95% CI 0.72–1.89), undifferentiated JIA (β 1.06, 95% CI 0.32–1.80), physician’s global disease activity assessment (β 0.64, 95% CI 0.54–0.74), female sex (β 0.85, 95% CI 0.41–1.28), NSAID (β 0.58, 95% CI 0.28–0.88), and intraarticular glucocorticoid use (β 0.58, 95% CI 0.10–1.07; Table 2). There was no significant interaction between biologic and DMARD exposure (p = 0.13) and no significant association of biologic or DMARD exposure and pain.
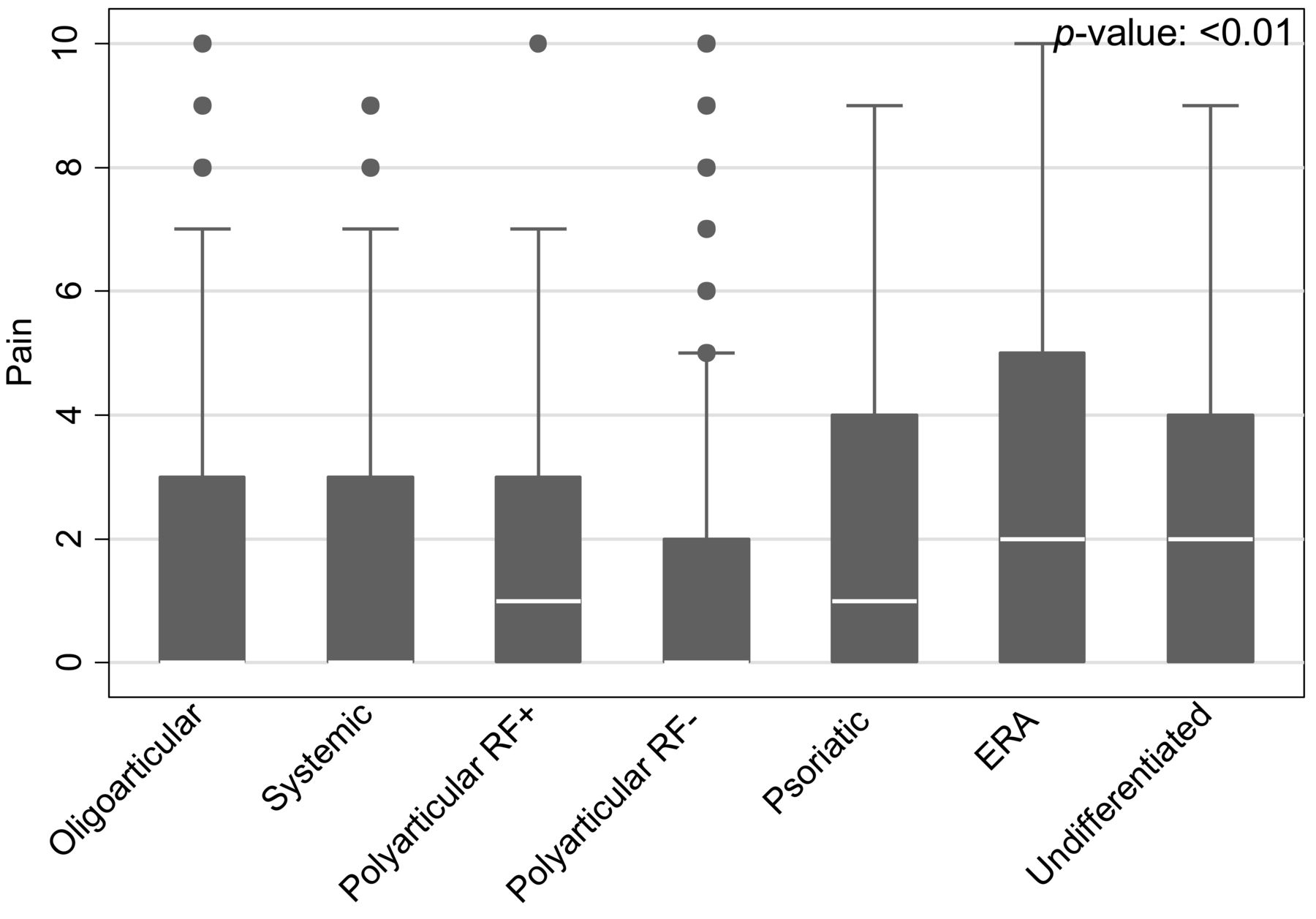
Box plot of pain scores across JIA categories. Number of visits for oligoarticular: 451, systemic: 91, RF+: 42, RF−: 213, psoriatic: 80, ERA: 257, and undifferentiated: 92. JIA: juvenile idiopathic arthritis; RF+: polyarticular rheumatoid factor-positive; RF−: polyarticular RF-negative; ERA: enthesitis-related arthritis.
Factors associated with pain, quality of life, and physical function across JIA categories. Mixed-effects multivariate analysis of clinical variables associated with PRO. Variables with p < 0.20 in univariate analysis were included in multivariate analysis. Subject was a random effect in all models. Values are ß (95% CI).
Because ERA and undifferentiated JIA categories had significantly greater prevalence and intensity of pain, we investigated additional clinical factors associated with pain within these categories. Clinical attributes significantly associated with increased pain in children with ERA in a multivariate model included physician’s global disease activity assessment (β 0.68, 95% CI 0.46–0.89), female sex (β 1.42, 95% CI 0.69–2.15), and tender enthesis count (β 0.16, 95% CI 0.05–0.28). Longer disease duration (β −0.53, 95% CI −0.91 – −0.15) and HLA-B27 positivity (β −0.98, 95% CI −1.67 – −0.30) were inversely associated with pain (Table 3). Physician’s global disease activity assessment was the only variable significantly associated with pain in undifferentiated JIA (β 0.86, 95% CI 0.43–1.28; Table 4).
Factors associated with pain, quality of life, and physical function in children with ERA. Mixed-effects multivariate analysis of factors associated with PRO in children with ERA. Variables with p < 0.20 in univariate analysis were included in multivariate analysis. Subject was a random effect in all models. Values are ß (95% CI).
Factors associated with pain, quality of life, and physical function in children with undifferentiated JIA. Mixed-effects multivariate analysis of factors associated with PRO in these children. Variables with p < 0.20 in univariate analysis were included in multivariate analysis. Subject was a random effect in all models. Values are ß (95% CI).
Quality of life
Children with ERA and psoriatic arthritis (PsA) had a higher prevalence of decreased quality of life within the past 4 weeks (p < 0.01), and undifferentiated JIA reported the highest median value of decreased quality of life (Figure 2). Variables associated with decreased quality of life in multivariate analysis included ERA (β 1.81, 95% CI 0.89–2.74), undifferentiated JIA (β 2.61, 95% CI 1.43–3.79), physician’s global disease activity assessment (β 0.60, 95% CI 0.46–0.73), female sex (β 1.33, 95% CI 0.66–2.01), active joint count (β 0.14, 95% CI 0.05–0.22), and NSAID use (β 0.72, 95% CI 0.31–1.13; Table 2). There was no significant interaction between biologic and DMARD exposure (p = 0.64) and no significant association of biologic exposure and quality of life.
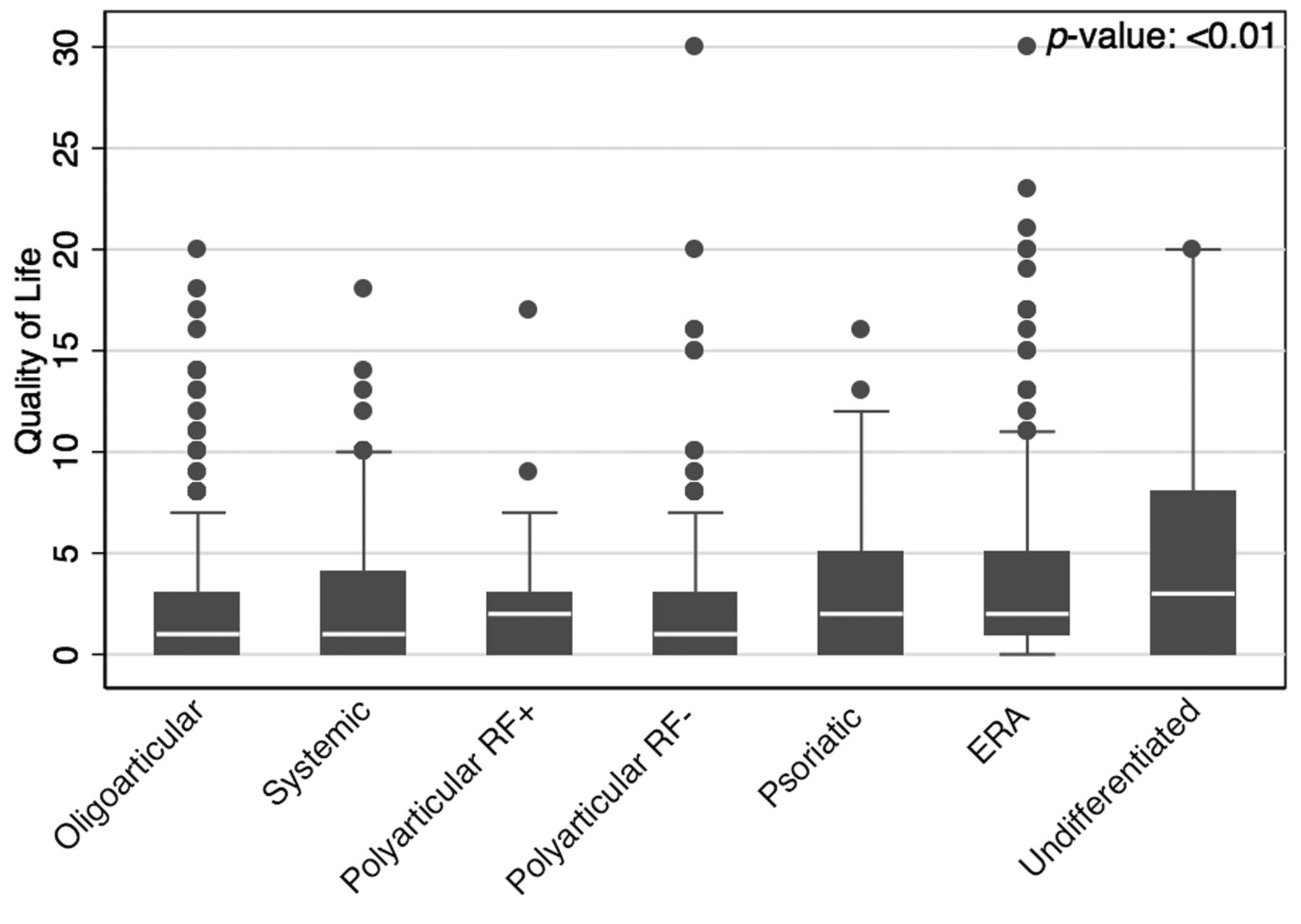
Box plot of quality of life values across JIA categories. Number of visits for oligoarticular arthritis: 449, systemic: 89, RF+: 43, RF−: 220, psoriatic: 81, ERA: 250, and undifferentiated: 94. JIA: juvenile idiopathic arthritis; RF+: polyarticular rheumatoid factor-positive; RF−: polyarticular RF-negative; ERA: enthesitis-related arthritis.
ERA and undifferentiated categories were associated with higher prevalence and more impaired quality of life than other JIA categories. In a multivariate analysis of children with ERA, significant predictors of decreased quality of life included physician’s global disease activity assessment (β 0.44, 95% CI 0.15–0.74), disease duration (β −0.70, 95% CI −1.34 – −0.07), female sex (β 1.96, 95% CI 0.47–3.44), and tender enthesis count (β 0.28, 95% CI 0.08–0.48; Table 3). For children with undifferentiated JIA, significant predictors of decreased quality of life were physician’s global disease activity assessment (β 1.07, 95% CI 0.36–1.78), female sex (β 4.56, 95% CI 1.96–7.17), and NSAID use (β 3.27, 95% CI 1.23–5.31; Table 4).
Physical function
Children with polyarticular RF-positive, polyarticular RF-negative, and ERA reported the highest prevalence of decreased physical function. Polyarticular RF-positive, ERA, and undifferentiated JIA reported moderate and severe impairment in function more commonly than other JIA categories (p < 0.01). In multivariate analysis, factors associated with decreased function in all patients with JIA included ERA (β 0.15, 95% CI 0.06–0.24), undifferentiated JIA (β 0.15, 95% CI 0.02–0.28), physician’s global disease assessment (β 0.06, 95% CI 0.04–0.07), female sex (β 0.10, 95% CI 0.03–0.18), active joint count (β 0.01, 95% CI 0.01–0.02), and NSAID use (β 0.07, 95% CI 0.03–0.11; Table 2). There was no significant interaction between biologic and DMARD exposure (p = 0.66) and no significant association of biologic exposure and function.
ERA and undifferentiated JIA reported higher intensity of decreased physical function than other JIA categories. In multivariate analysis of children with ERA, significant factors associated with decreased physical function included female sex (β 0.28, 95% CI 0.10–0.45), tender enthesis count (β 0.06, 95% CI 0.04–0.08), and systemic glucocorticoid use (β 0.16, 95% CI 0.01–0.31; Table 3). For children with undifferentiated JIA, significant factors associated with decreased function were physician’s global disease activity assessment (β 0.05, 95% CI 0.01–0.10), female sex (β 0.31, 95% CI 0.05–0.57), active joint count (β 0.09, 95% CI 0.03–0.14), and NSAID use (β 0.22, 95% CI 0.07–0.37; Table 4).
Correlation of physician rating with PRO
The Spearman correlations for physician’s global disease activity assessment with parent/patient-reported pain, quality of life, physical function, and health status were moderate (0.53, 0.40, 0.43, and 0.53, respectively, all p < 0.01).
DISCUSSION
Ours is one of the largest studies to evaluate pain, quality of life, and function over time across JIA categories. We found statistically significant differences in PRO across JIA categories, notably in children with ERA and undifferentiated JIA who consistently reported the poorest PRO. Children with ERA and undifferentiated JIA had significantly more pain, worse quality of life, and poorer function than children in the other JIA categories. Physician’s overall disease activity assessment only moderately mirrored PRO. Interestingly, in this cohort, physicians gave the highest disease activity scores to children with RF-negative polyarticular disease, PsA, and ERA. This discordance highlights that disease manifestations and the relevance of PRO to overall disease activity assessment are contemplated and valued differently by patients and their parents and physicians.
These results need to be interpreted in light of several limitations. Ours is a retrospective study, so data collection was not complete, as it would be with a prospective trial. While PRO at our institution are routinely collected as part of clinical care, there were some missing data. However, < 25% of PRO and < 15% of physician-reported outcomes were missing in our dataset. Spectrum and/or selection bias are possible as our results are from a single-center tertiary care medical center. However, our rheumatologists treat patients with a wide variation in symptoms and severity of disease, and thus our patients should represent the full breadth of cases that present across other institutions.
There are several interesting findings from our study that warrant further discussion. First, the children who had poorer PRO (pain, quality of life, and function) were those in the JIA categories under the broader umbrella term “juvenile spondyloarthritis” (SpA). The term SpA primarily encompasses the ERA, psoriatic, and undifferentiated JIA categories, but also includes juvenile ankylosing spondylitis, reactive arthritis, and inflammatory bowel disease-associated arthritis. Distinct features of SpA in comparison with other JIA categories include enthesitis, axial disease, skin, and nail findings. Interestingly, some of these unique attributes were significant or trended toward being significantly associated with pain in the restricted analyses of PRO for these categories. While not statistically significant, PsA also trended to having increased pain and decreased quality of life. These results suggest that some of our treatment algorithms or medications themselves may not be as effective for these disease manifestations, and specifically, despite advent of newer pharmacotherapies, patients with ERA continue to report worse PRO12. Indeed, several pediatric and adult studies show enthesitis and axial disease may not respond as well as arthritis to traditional DMARD and/or biologic therapy24,25,26,27.
Second, our results are in accordance with prior studies that suggest altered pain perception in adults and children with SpA28. A study has shown that children with ERA have lower thresholds of pain at the enthesis than healthy children10. This altered perception occurred at enthesis with and without underlying ultrasound-confirmed tendinopathy or increased Doppler blood flow. However, it is unknown whether these altered pain perceptions are unique to SpA or whether they exist across all JIA categories29,30. Although children with JIA can have more pain than healthy children, it is unknown whether this is primarily from their disease or secondary to psychological factors and deconditioning from having a chronic disease31.
Third, while we included as many clinical variables as available in our medical charts, our models could not perfectly predict the outcomes of pain, quality of life, and physical function. This highlights that these constructs are very complex and despite having access to qualitative and quantitative variables, there are still other unidentified factors that likely contribute to pain, quality of life, and physical function. The presence of fatigue and amplified musculoskeletal pain have been reported to influence PRO32,33, and this was not systematically recorded in our cohort. Another study suggests that patients place emphasis on being like their peers without a chronic condition and emphasize the psychosocial aspect of living with JIA34, and these domains were not fully identified by our PRO. Similarly, we do not have measures of baseline physical activity, school performance, comorbid conditions, or psychological diagnosis that may also influence PRO.
Our findings highlight that there are significant differences in PRO across JIA categories. Those children with ERA and undifferentiated JIA had poorer outcomes in all PRO assessed. Additionally, despite the poorer PRO, physician’s assessments of disease activity in these children were only moderately correlated. Our results highlight the importance of assessing both physician-reported outcomes and PRO as part of both routine care and clinical studies. Further work is needed to address ways to improve PRO in children with JIA, with a special focus on children with ERA and undifferentiated JIA.
Acknowledgment
The authors thank The Children’s Hospital of Philadelphia Center for Biomedical Informatics, Andrew Klink, and Keshia Maughn for helping prepare analytic datasets.
Footnotes
Supported by the Rheumatology Research Foundation, Clinical and Translational Science Awards grants NCRR UL1RR024134 and NCATS UL1TR000003, and The US National Institute of Child Health and Human Development Clinical Pharmacoepidemiology Training Grant 5T32HD645674. Dr. Weiss’s work was supported by the US National Institute of Arthritis and Musculoskeletal and Skin Diseases grant 1K23AR05974901A1.
- Accepted for publication June 22, 2015.








{kind=link}
{kind=link}