

Abstract
Objective. Few studies have examined the relationship between gout and erectile dysfunction (ED). We investigated whether patients with gout exhibited an increased risk of ED.
Methods. This longitudinal nationwide cohort study investigated the incidence and risk of ED in 19,368 men with gout who were newly diagnosed between January 2002 and December 2008. A total of 77,472 controls without gout were randomly selected from the general population and frequency-matched according to age and sex. The patients were followed up from the date on which they were included in the study cohort to the date of an ED event, censoring, or December 31, 2010. We conducted the Cox proportional hazard model to estimate the effects of gout on ED risk including age and comorbidities.
Results. The gout cohort exhibited a 1.21-fold adjusted HR of subsequent ED development compared with the non-gout cohort (95% CI 1.03–1.44). The incidence of ED increased with age in both cohorts and was higher among the patients in the gout cohort than among those in the non-gout cohort. Compared to the patients without gout and comorbidities, the patients with both gout and any type of comorbidity exhibited a 2.04-fold risk of developing ED (95% CI 1.63–2.57). Further, the patients with gout who had numerous comorbidities exhibited the dose-response effect in developing ED.
Conclusion. This nationwide cohort study revealed that ED risk is significantly higher in patients with gout than in the general population.
Gout, of which the global prevalence is about 0.08%, is the most common cause of inflammatory arthritis in men worldwide1. Previous reports have focused on the pharmacological and nonpharmacological treatment of gout2,3,4. Gout frequently coexists with diabetes and hypertension, and is often neglected as a genuine risk factor for vascular disease5,6. Studies have demonstrated that gout is an independent risk factor for cardiovascular disease (CVD) and cerebrovascular disease7,8.
Erectile dysfunction (ED) is defined as the failure to attain or maintain an adequate erection during sexual activity. It affects millions of men worldwide9,10,11 and constitutes one of the most prevalent sexual problems12. The prevalence of ED is strongly correlated with age13. Feldman, et al used a self-administered questionnaire in the context of the Massachusetts male aging study and reported that ED affected about 40% of men at age 40; further, the prevalence increases to nearly 70% in men aged 7014. ED may cause low self-esteem, performance anxiety, and marital discontent. However, older men with ED do not like to discuss it with their physicians; therefore, ED remains underdiagnosed and undertreated15,16.
Various chronic medical illnesses, including diabetes, CVD, and depression, are related to ED17,18. However, the relationship between gout and ED is not clear. Therefore, we investigated the causal association between gout and the development of ED in Taiwan. The results were obtained from a nationwide retrospective cohort study assessing the possibility that the risk of ED is increased among patients with gout.
MATERIALS AND METHODS
Data sources
The National Health Insurance (NHI) program in Taiwan is a single-payer, compulsory insurance system that was established in 1995 by the Bureau of National Health Insurance (BNHI), Ministry of Health and Welfare. The insurance program provides healthcare to 99% of the 23.74 million citizens of Taiwan and maintains contracts with 97% of the nation’s healthcare institutions19. The National Health Research Institute is authorized to establish the NHI Research Database (NHIRD), as well as to manage registration and claim data for the 23 million insured citizens. The current study used a subset of the NHIRD that consisted of 1 million randomly sampled beneficiaries enrolled in the NHI program. All of the NHI datasets can be interlinked through the de-identification of people; thus, NHI reimbursement data are suitable for public academic research. Each NHI dataset includes information on medical facility registries, inpatient orders, ambulatory care, dental services, prescription drugs, and physicians providing services as well as registration files containing encrypted identification data. Diagnoses are coded according to the International Classification of Diseases, 9th ed, Clinical Modification (ICD-9-CM). The high accuracy and validity of ICD-9-CM diagnoses in the NHIRD have been described in previous studies20,21. This cohort study was approved by the Ethics Review Board of China Medical University Hospital (CTU 103-1/CMUH 103-REC1-088).
Study patients
We included in the gout cohort men aged 18 to 64 years with gout (ICD-9-CM Code 274) who were newly diagnosed by physicians between January 2002 and December 2008. The date of gout diagnosis was used as the index date. We excluded patients with a history of gout or ED preceding the index date. The comparison cohort was composed of randomly selected patients with no history of gout or ED, and these patients were frequency-matched with the patients with gout according to sex, age, and index date. Four people were assigned to the comparison cohort for each patient with gout.
Outcome measures
In general, the primary outcome was newly diagnosed ED (ICD-9-CM Code 607.84) that was identified by the urologists or physicians of internal or family medicine based on the patient’s medical record, recent symptoms, scores of the Sexual Health Inventory for Men (SHIM) questionnaire, physical examination, and laboratory studies. The followup person-years were determined by calculating the interval between the index date and the date on which any of the following events occurred: the date of ED diagnosis, the date of withdrawal from the NHI program, the date of death, or December 31, 2011.
Covariates and comorbid diseases
The patients were stratified according to age into the following groups: ≤ 34 years, 35–44 years, 45–54 years, and 55–64 years. The comorbidities included in our study were diabetes (ICD-9-CM Code 250), congestive heart failure (ICD-9-CM Code 428), ischemic heart disease (ICD-9 Codes 410–414), hypertension (ICD-9 Codes 401–405), depression (ICD-9-CM Codes 296.2, 296.3, 300.4, 311), and chronic renal failure (ICD-9 Code 585). Further, we incorporated urate-lowering agents, including allopurinol, probenecid, benzbromarone, sulfinpyrazone, and febuxostat, into consideration for investigating the effect of urate-lowering therapy (ULT) on the development of ED.
Statistical analysis
All statistical analyses were performed using SPSS 17.0 software (SPSS Inc.). Differences in the proportional distribution of the demographic characteristics and comorbidities of the patients with gout and patients without gout were compared and tested using the chi-square test. The mean ages of both cohorts were measured and tested using the Student t test. The followup person-years were used to estimate the incidence density of ED. The incidence density rates of ED for the incidence rate ratios (IRR) of the gout cohort to the non-gout cohort and 95% CI were calculated based on the demographic statuses and comorbidities of the patients. The IRR were determined using the Poisson assumption. We assessed the overall, age-specific, and comorbidity-specific incidence of ED in both the gout and non-gout cohorts, and used Cox proportional hazard regression analysis to estimate the HR with 95% CI of ED development in the gout cohort and compared the results with those of the non-gout cohort. In addition, we measured the incidence and the HR for the interaction between gout and comorbidities on ED development. To assess the difference in the ED-free rates between the 2 cohorts, we applied Kaplan-Meier analysis and the log-rank test. All of the tests were performed at a 2-tailed significance level of 0.05.
RESULTS
Demographic characteristics and comorbidities of the patients with gout and people without gout
The gout cohort was composed of 19,368 patients and the comparison cohort was composed of 77,472 people without gout. The age distributions of the patients in the 2 cohorts were the same. The mean age of the patients in both cohorts were 42.7 ± 12.0 years. The prevalence of comorbid diseases, such as diabetes (11.2% vs 7.1%), ischemic heart disease (6.7% vs 4.1%), congestive heart failure (1.1% vs 0.6%), hypertension (25.5% vs 13.0%), and chronic renal failure (1.0% vs 0.6%), was significantly higher in the gout cohort than in the comparison cohort (Table 1).
Demographic characteristics and comorbidities in patients with and without gout. Data measured by chi-square test.
For patients without ED, the patients with gout had a significantly greater number of physician visits than did the non-gout cohort (21.9 ± 19.6 vs 16.5 ± 16.9, p < 0.001); whereas, for patients diagnosed with ED, the number of physician visits for the patients with gout was not significantly different from that of the non-gout cohort (49.7 ± 40.2 vs 51.0 ± 72.0 visits per person-yrs, p = 0.816). Further, the number of ED diagnoses made by the urologists was not significantly different between the patients with gout and the non-gout cohort (80.6% vs 82.4%, p = 0.582).
Comparison of the incidence and HR of ED between the gout cohort and the comparison cohort
The objective of our study was to investigate the effect of gout on the development of ED. In this causal study, it was found that, compared with the patients without gout, the patients with gout exhibited a higher incidence rate of ED (12.36 vs 9.07 per 10,000 person-yrs, p < 0.001), and the adjusted HR was 1.21 (95% CI 1.03–1.44, p < 0.001) after we controlled for age and comorbidities. The incidence rates of ED increased with age in both cohorts. The unadjusted IRR of ED was used to compare the patients with gout with the non-gout cohorts based on individual age strata. On the other hand, the adjusted HR of the successive age strata shown in Table 2 were obtained by taking the whole cohort into consideration in the full model with the aged ≤ 34 group treated as the reference. As shown in the table, the incidence rate of ED was significantly higher in the gout cohort than in the non-gout cohort. After we adjusted for covariates, the risk of ED was the highest in the group of patients aged 55–64 years, and the adjusted HR was 5.68 (95% CI 4.17–7.73) compared with the group of patients ≤ 34 years of age. The adjusted HR increased with age, which was consistent with the observation reported in previous investigations13,14. Patients with 1 or more comorbidities exhibited a higher incidence rate of ED than did those without any comorbidity in both cohorts. After we adjusted for covariates, the patients with any type of comorbidities exhibited a 1.79-fold increased risk of ED compared with those with no comorbidity (95% CI 1.53–2.09).
Comparison of incidence rate and HR of ED stratified by age and comorbidity between patients with and without gout.
Interaction on the risk of ED between gout and any comorbidity
The interaction measurements between gout and any comorbidity on the risk of ED are shown in Table 3. Compared with the patients without gout or comorbidity, the patients without gout but with comorbidities exhibited a 1.92-fold risk of developing ED (95% CI 1.61–2.30), and the highest risk was observed in patients with both gout and comorbidities (adjusted HR 2.04, 95% CI 1.63–2.57).
Cox proportional hazards regression analysis for interaction of gout and comorbidity on risk of ED.
Association between the risk of ED and the number of comorbidities
Table 4 lists the incidence and risk of ED in patients with or without gout accompanied with various numbers of comorbidities. The patients with a different number of comorbidities exhibited a dose response effect of ED development compared to the non-gout participants with no comorbidity. Compared with the patients without gout and without comorbidity, the adjusted HR of increasing number of comorbidities increased in both cohorts (Table 4). For patients without comorbidity or with 2 or more comorbidities, the crude HR and adjusted HR of patients with gout were both higher than patients without gout.
HR and 95% CI of ED risk associated with the ULT and the number of comorbidities.
Additionally, compared with the patients without gout with no comorbidity, the HR of developing ED remained greater in the patients with gout without comorbidity receiving fewer than 90 days of ULT (adjusted HR 1.41, 95% CI 1.11–1.79), but reached no significant difference in those who received 90 days or more of ULT (adjusted HR 0.88, 95% CI 0.12–6.27).
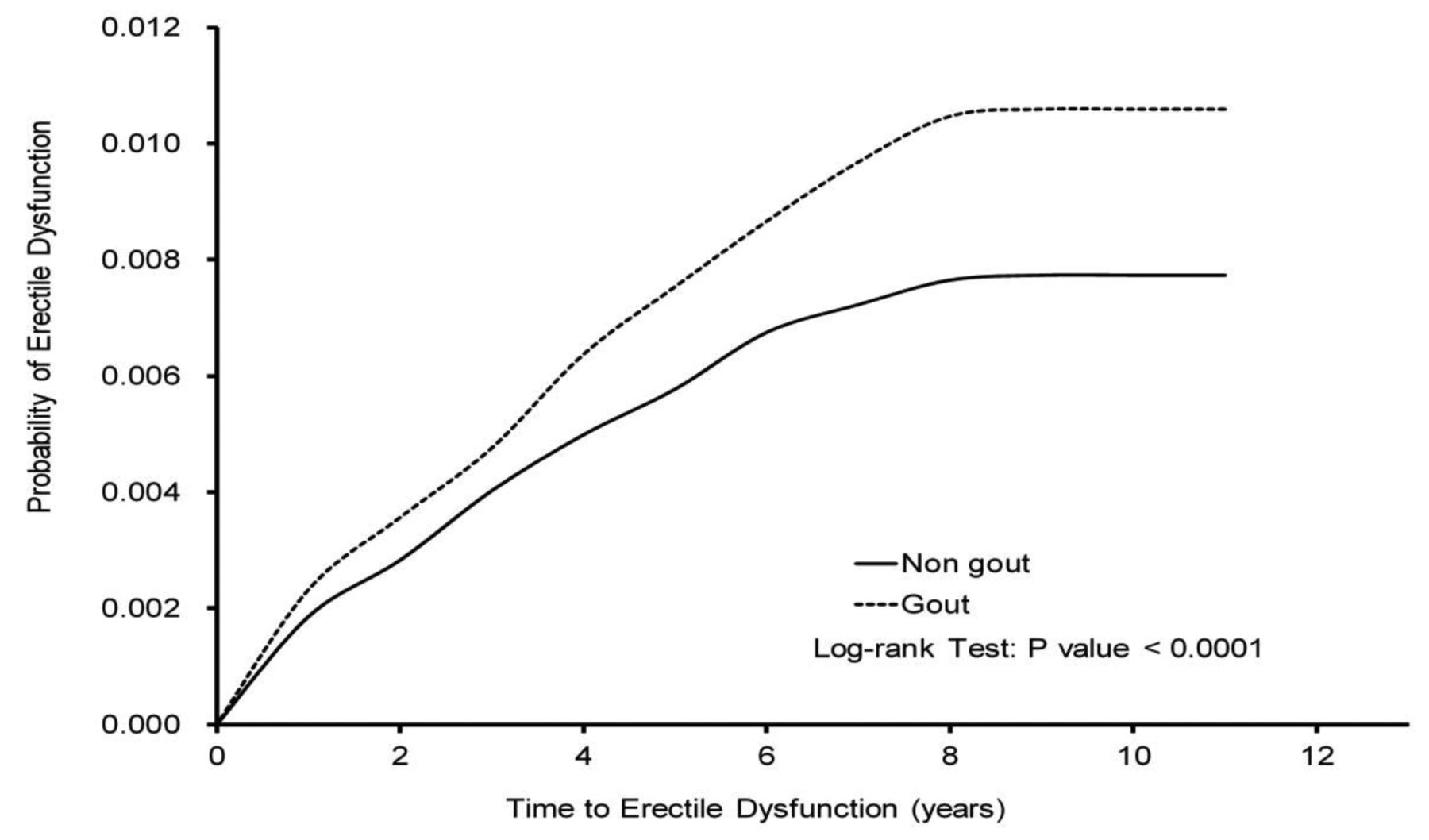
Probability of ED in the gout and non-gout cohorts during followup
Figure 1 shows the Kaplan-Meier curve of ED for the patients with gout and those without gout, in which the Y axis indicates the accumulated probability of acquired ED as a function of time (in years) after gout being diagnosed until ED occurred. The results indicated that the cumulative probability of ED was significantly greater in the patients with gout than in those in the non-gout cohort (log rank p < 0.0001).

Kaplan-Meier analysis comparing probabilities of ED between patients with gout and non-gout cohort. ED: erectile dysfunction.
DISCUSSION
Most previous studies focused on cross-sectional investigations of the association between gout and ED22,23. It was reported that men with gout were more likely to have ED than men without gout by using self-reported questionnaires (76% vs 52%, p < 0.001)22 and by reviewing patient medical history, physical examination results, and recent laboratory studies accompanied by the filled SHIM questionnaire (39.8% vs 28.8%, p < 0.001)23 in the context of a US community-based study. Schlesinger, et al23 showed that after adjusting for age and comorbidities, including hypertension, low-density lipoprotein, diabetes, depression, obesity, and chronic kidney disease, gout was still significantly associated with ED. To our knowledge, to date no causal study regarding the association between gout and ED has been conducted. This is the first study to investigate the effect of gout on the risk of subsequent ED in an Asian population by using a nationwide cohort study. The study determined that patients with gout exhibited a 1.21-fold greater risk of ED development than did the non-gout comparison cohort. Previous studies have also indicated that the detrimental health effects of gout include an increased risk of cardiovascular and cerebrovascular events7,24,25.
As indicated in Table 2, among the patients with comorbidity, the incidence rate of ED in patients without gout (19.49 per 10,000 person-yrs) was similar to those with gout (19.58 per 10,000 person-yrs). The IRR of 1.00 (95% CI 0.78–1.25) indicates that comorbidities may dilute the influence of gout on ED. However, among those without comorbidities, the risk of ED for patients with gout was significantly higher than for those without gout with an IRR of 1.31 (95% CI 1.04–1.67), suggesting that gout might be an independent factor increasing the risk of ED. As presented in Table 3, the incidence rate of ED for patients who had no gout but had 1 or more comorbidities (19.49 per 10,000 person-yrs) was much higher than those who had gout but without comorbidities (8.7 per 10,000 person-yrs). However, the former cases were entangled with multiple factors, (i.e., 1 or more comorbidities) while in the latter, only 1 single factor had been involved (i.e., gout). Moreover, the incidence rate of ED for patients who had gout but without comorbidities was significantly higher than for those with neither gout nor comorbidity (8.7 vs 6.61 per 10,000 person-yrs) with an adjusted HR of 1.40 (95% CI 1.11–1.77). The patients with gout with 1 or more comorbidities had a 2.04-fold increased risk of ED compared with that of the non-gout cohort that did not have any comorbidities (Table 3). Again, these data indicate that gout is an independent factor in predicting the ED development.
The direction of causality in the relationship between gout and ED is not clear. The pathogenic mechanisms of gout indicate an inflammatory response that may contribute to vascular effects26. Inflammation may induce endothelial dysfunction and evolve into arteriosclerosis27,28. In addition, the inflammatory process can cause clotting, thereby reducing the activity of natural anticoagulant mechanisms and impairing the fibrinolytic system29,30. The comorbidities associated with gout include hypertension, diabetes, obesity, and chronic kidney diseases, all of which are associated with similar risks with vascular diseases31. The pathophysiological mechanisms of ED can be classified into 4 types: psychogenic, neurogenic, endocrinologic, and arteriogenic mechanisms32. Table 5 lists the pathophysiological mechanisms of ED associated with gout27,28,29,30 and other comorbidities, including diabetes17, ischemic heart disease33,34, congestive heart failure35,36, hypertension37,38, depression18, and chronic renal failure39.
Pathophysiological mechanism of erectile dysfunction associated with gout and other comorbid diseases.
The incidence of ED increased with age in both cohorts, exhibiting an especially marked increase after the age of 45; this result is consistent with those reported in previous studies40,41,42,43. In the population-based cohort studies of US citizens and Brazilians, it was observed that the incidence rates of ED in men 40 to 90 years old were 259 and 656 cases per 10,000 person-years, respectively40,43. In our population-based cohort study, the incidence rate of ED in men 18 to 64 years old without gout was only 9.07 cases per 10,000 person-years, which is much lower than the US and Brazilian populations. The difference of ED incidence between our study and the Western study might be associated with various races and age study groups. Biological aging causes older men to be more likely to have comorbid conditions than younger men. In addition to the aging process, reduced physical activity among older men may increase the risk of ED41,44.
Men with comorbid diseases exhibited a 1.79-fold greater risk of ED than did those who did not have comorbidities (Table 2). Previous reports have indicated that the prevalence of ED is positively associated with cardiovascular risk factors such as diabetes and heart diseases45,46. Ischemic heart disease and ED are frequently comorbid and share common risk factors, including age, hypertension, and diabetes. The patients with gout who had any type of comorbid condition exhibited a multiplicative risk of developing ED compared with those with no gout or comorbid diseases. Further, the patients with gout who had various comorbidities exhibited a dose-response effect on the development of ED. In addition, the cumulative rate of ED was significantly greater in the gout cohort than in the non-gout cohort. These results are relatively robust because several multivariable model analyses were used to assess the increased risk of ED development.
Compared with non-gout with no comorbidity, the patients with gout without comorbidity receiving fewer than 90 days of ULT remained at a greater risk of ED. On the other hand, the patients with gout without comorbidity receiving 90 days or more of ULT reached no significant difference of ED risk compared with the non-gout cohort without comorbidity. This finding indicated that receiving ULT for more than 90 days may decrease the risk of ED development for patients with gout who had no comorbidity. Because gout is deemed a chronic disease, physicians are allowed to prescribe the third consecutive refill medication for patients with chronic diseases, according to the regulations of the NHI Bureau of Taiwan. Patients have to visit their physicians again for tracking of the disease progression and for additional consecutive prescriptions. It is assumed that patients with gout who have received more than 1 continuous medication prescription might have adhered to longterm treatments, resulting in better control of gout and a prevention of ED occurrence.
As listed below, several limitations must be considered when interpreting these findings:
Lack of lifestyle information in NHIRD. Because patients with gout are more likely to have comorbidities, an increased risk of ED in patients with gout may be associated with comorbidities that were either not measured or comorbidities that were not recorded in the patient’s records. For example, detailed lifestyle information, such as body mass index, physical activity levels, socioeconomic status, alcohol use, and smoking status, which could potentially confound the results of our study, are not provided in NHIRD.
ED diagnosis based on clinic visits and physician diagnoses. Most Taiwanese are shy or ashamed to visit physicians for ED; thus, the actual incidence of ED may have been underestimated.
Study cases selected based on ICD-9-CM codes. This potentially caused misclassification bias. However, the BNHI can audit the diagnosis and management codes by means of a peer review to minimize diagnostic uncertainty and misclassification.
Patients having more physician visits might be more likely to be diagnosed with ED. The patients with gout or without gout who had been diagnosed with ED had a higher number of physician visits than did patients who had no ED (Table 1). However, the association between the number of physician visits and probability of being diagnosed with ED is not clear, because other diseases or comorbidities may also increase the frequency of physician visits.
Our study is the first, to our knowledge, to provide epidemiologic data to address the relationship between gout and ED. The strength of our study lies in the use of a large sample size representing an Asian population to investigate the relationship. Each NHI beneficiary is assigned a unique personal identification number; therefore, every participant could be tracked in the NHIRD throughout the followup period. Moreover, the ED diagnoses were provided by physicians rather than self-reported by the patients.
Our nationwide population-based cohort study, which examined 19,368 patients with gout over a followup period of about 150,000 person-years, indicated that patients with gout are at a 1.21-fold greater risk of developing ED than the general population. These findings emphasize the importance of implementing a multidisciplinary approach to manage the potential risk factors contributing to the development of ED among patients with gout. Additional studies on the biological mechanisms of gout and its effect on the development of ED are warranted.
Footnotes
Supported by Taichung Hospital, Ministry of Health and Welfare under grant no. FL1030505007-2 and Ministry of Science and Technology under grant no. MOST104-2622-H-166-001.
- Accepted for publication April 21, 2015.








{kind=link}