

Abstract
Objective. The diagnostic values of antiproteinase 3 and antimyeloperoxidase tests using antineutrophil cytoplasmic antibodies (ANCA) are well established. Our study determined whether an increase in ANCA level was a predictor of disease flareup.
Methods. Our study included 126 patients with ANCA-associated renal vasculitis treated at 9 nephrology centers in Japan. The relationship between increased ANCA levels and relapse was assessed using time-dependent multivariate Cox regression models adjusted for clinically relevant factors. The outcome of interest was the time from remission to first relapse.
Results. During the observation period [median 41 mos, interquartile range (IQR) 23–66 mos], 118 patients (95.8%) achieved remission at least once. After achieving remission, 34 patients relapsed (21.7%). Time-dependent multivariate Cox regression models revealed that lung involvement (adjusted HR 2.29, 95% CI 1.13–4.65, p = 0.022) and increased ANCA levels (adjusted HR 17.4, 95% CI 8.42–36.0, p < 0.001) were significantly associated with relapse. The median time from ANCA level increase to relapse was 0.6 months (IQR 0–2.1 mos).
Conclusion. In our study, an increase in ANCA level during remission was associated with a risk of disease relapse. A rise in ANCA level may be useful for guiding treatment decisions in appropriate subsets of patients with ANCA-associated vasculitis.
- ANTINEUTROPHIL CYTOPLASMIC ANTIBODIES
- ANCA-ASSOCIATED VASCULITIS
- GRANULOMATOSIS WITH POLYANGIITIS
- MICROSCOPIC POLYANGIITIS
- ANCA LEVEL
- RELAPSE
Antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV) includes granulomatosis with polyangiitis (GPA) and microscopic polyangiitis (MPA). Most patients with GPA or MPA achieve clinical remission with initial immunosuppressive therapy1,2,3,4,5, but 11–57% experience relapse6,7,8,9,10,11,12. Most relapses respond to immunosuppressive therapy. However, some are refractory, resulting in considerable morbidity and mortality associated with worsening end-organ damage.
Although the diagnostic values of antiproteinase 3 (anti-PR3) and antimyeloperoxidase (anti-MPO) ANCA tests are well established13,14,15,16, it is controversial whether an increase in ANCA level predicts disease flareup. Some studies indicate that persistently high or increasing ANCA levels are associated with an increased risk of disease relapse17,18,19. Meanwhile, others demonstrate that an elevated ANCA level does not predict disease flareups in a timely manner20,21. Therefore, the temporal relationship between an increase in ANCA level and the occurrence of disease flareup is considered weak.
In contrast to previous studies, the demographics of our present study are based mainly on MPA rather than GPA, and the proportion of kidney involvement is higher. Reports from Japan also suggest that most patients with AAV are classified as having MPA and that MPO-ANCA–associated disease is much more common than PR3-ANCA–associated disease22, with GPA apparently being much rarer. Therefore, previous findings based mainly on patients with GPA remain to be confirmed in patients with MPA with kidney involvement.
Our study determined whether an increased ANCA level was an independent predictor of relapse and described treatment methods for patients with MPO-ANCA–positive MPA in Japan. Our multicenter observational cohort study was based at 9 major nephrology centers in Nagoya, Japan.
MATERIALS AND METHODS
Study population and data source
Our cohort study included patients aged > 15 years diagnosed with AAV including GPA and MPA on the basis of the European Medicines Agency algorithm23 with a consensus methodology for the classification of the AAV between January 2004 and December 2012. The study involved Nagoya University, Chubu Rosai Hospital, Japanese Red Cross Nagoya Daiichi Hospital, Tsushima City Hospital, Kasugai Municipal Hospital, Nagoya Kyoritsu Hospital, Anjo Kosei Hospital, Ichinomiya Municipal Hospital, Handa City Hospital, or Tosei General Hospital. Of 131 such patients, we excluded 5 (3.8%) because of a history of malignancies (n = 1), missing data (n = 1), a lack of immunosuppressive therapy (n = 2), or ANCA-negative test results at the time of initial visit (n = 1). Finally, 126 patients with AAV (93.3%) who received immunosuppressive therapy were included.
Our study was conducted using a linkable anonymous dataset. No informed consent was required. The study protocol and consent procedure were approved by the respective ethics committees of the 9 centers listed above (approval number: 2012-0268).
Data collection
Baseline characteristics preceding the initiation of immunosuppressive therapy were collected retrospectively from medical records, including age, sex, serum creatinine concentration, and MPO- and PR3-ANCA levels. Details of the use of corticosteroids and/or other immunosuppressive agents during followup were also collected.
We retrospectively scored disease activity at months 3, 6, 12, 18, and 24 and at relapse, according to the Birmingham Vasculitis Activity Score (BVAS) 200324. Further, the disease severity of each patient was classified as localized, early systemic, generalized, or severe according to the European League Against Rheumatism recommendation for conducting a clinical study in systemic vasculitis25,26. Organ involvement was evaluated as previously described23,27.
The patients were generally seen every month, and ANCA levels were tested at each visit. Serum samples were diluted 1:500 (Nipro Medical Corporation) or 1:101 (Medical and Biological Laboratories Co. Ltd.) and subsequently tested as previously described28. In patients whose ANCA levels were negative, we defined a negative-to-positive conversion of MPO- or PR3-ANCA status as an increase in MPO- or PR3-ANCA levels exceeding the cutoff of ≥ 10 IU. To determine whether the criteria for increased ANCA were fulfilled, we compared the ANCA level at each visit with those from the 2 previous visits. In general, 3 clinical visits corresponded to a 2-month period. In patients who never achieved a negative ANCA level, we defined an increase of at least 100% as an increase in MPO- or PR3-ANCA levels according to previously described criteria, with slight modifications19.
Patients were followed until April 2014 and censored at the time of death if they died before April 2014. Remission was defined as the absence of clinical signs and symptoms of active vasculitis (BVAS = 0) for at least 2 months. Relapse was defined as clinical signs of vasculitic activity in any organ system following remission6.
Outcome
The outcome of interest in our study was the time from remission to first relapse.
Statistical analysis
To identify predictors independently associated with the primary outcome, potential covariates were examined using the log-rank test. In addition, univariate and multivariate time-dependent Cox regression models were used to evaluate the effect of ANCA level increase on relapse, as described19. For the time-dependent models, laboratory values were updated monthly, and the value of the last visit was imputed for those who had missing values. We adjusted for baseline data, including age, sex, serum creatinine level, and lung involvement, and followup data including the dose of prednisolone (PSL; mg/day) and use of immunosuppressants, using time-dependent Cox regression models. The cumulative probability of experiencing relapse was calculated using the Kaplan–Meier method and log-rank test. The level of statistical significance was set at p < 0.05. All statistical analyses were performed using JMP version 10.0.0 (SAS Institute; www.jmp.com) and SAS version 9.4 (SAS Institute; www.sas.com).
RESULTS
Study participants and clinical characteristics
Our present study included 126 patients with AAV. The baseline characteristics of the patient population are summarized in Table 1. The median age was 70 years [interquartile range (IQR) 63–75 yrs], and the population included 71 men (56.3%). Regarding disease, 99 (78.6%), 8 (6.3%), and 19 (15.1%) patients had MPA, GPA, and renal-limited disease, respectively. Anti-MPO and anti-PR3 antibodies were present in 123 (97.6%) and 3 (2.4%) patients, respectively. The mean creatinine level was 2.7 mg/dl (IQR 1.6–4.4 mg/dl), and all patients had kidney involvement with active urine sediment. Patients with extrarenal manifestations of vasculitis included 38 patients (30.2%) with lung involvement; 8 with ear, nose, and throat involvement (6.3%); 14 with nervous system involvement (11.1%); and 5 with cutaneous involvement (4.0%).
Baseline characteristics of patients with AAV (n = 126). Values are median (IQR) or n (%).
Treatment during the observation period
All patients received immunosuppressive therapy (Table 1). Because of the retrospective nature of our study, the immunosuppressive therapy protocol was not predetermined and depended exclusively on individual nephrologists. Induction therapy was typically initiated with 3 daily pulses of methylprednisolone followed by daily oral PSL. The most commonly used induction therapy was a combination of methylprednisolone pulse and oral PSL. PSL was started at 40 mg/day (IQR 30–47 mg/day) for the first month and tapered to 15 mg/day (IQR 11–18 mg/day) over 3 months. Five patients (4.6%) received an additional short course of plasma exchange as part of the induction therapy. During followup, 68 patients (54.0%) received PSL alone, whereas the others also received immunosuppressive agents, including intravenous (n = 16, 12.7%) or oral cyclophosphamide (CYC; n = 19, 15.1%), azathioprine (AZA; n = 21, 16.7%), and mizoribine (n = 13, 10.3%), usually after induction therapy.
Remission and relapse
Outcome data are shown in Table 2. During a median of 41 months of followup (IQR 23–66 mos), 118 patients (93.7%) achieved remission at least once. The median time to first remission was 2 months.
Outcomes of patients with AAV (n = 126). Values are n (%) or median (IQR).
After achieving remission, 34 patients (27%) relapsed at least once during the entire observational period. The median time from first remission to first relapse was 28 months (IQR 14–47 mos).
At relapse, the median BVAS 2003 score was 11 (IQR 8–14). Among patients with relapse, the kidneys were affected in 22 (64.7%); general symptoms including arthritis/arthralgia and fever occurred in 18 (52.9%); ear, nose, and throat involvement occurred in 3 (8.8%); pulmonary system involvement in 7 (20.6%); and nervous system involvement in 4 (11.8%).
The 1-, 2-, and 5-year cumulative probabilities of first relapse were 0.11 (95% CI 0.06–0.19), 0.20 (95% CI 0.13–0.29), and 0.40 (95% CI 0.29–0.52), respectively (Figure 1).
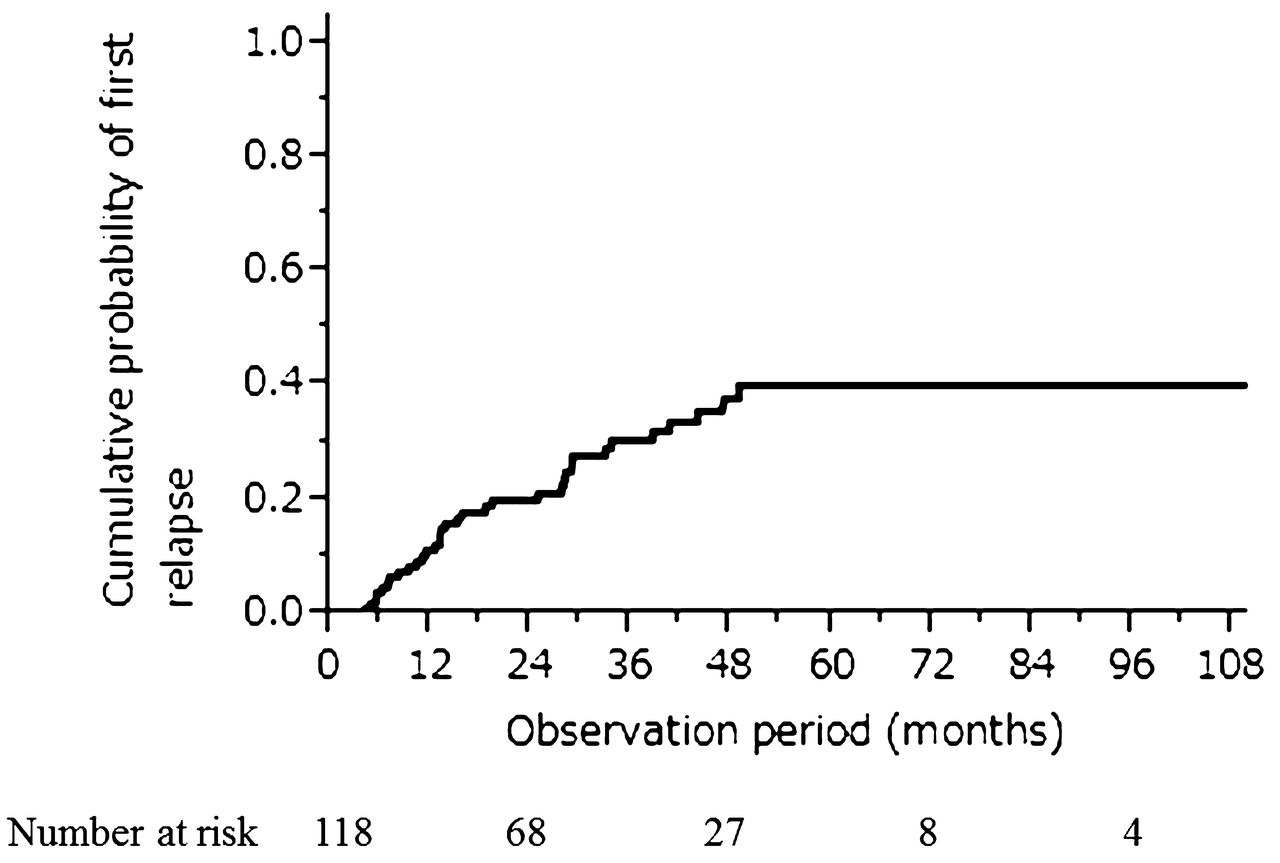
Cumulative probabilities of first relapse.
Of a total of 34 relapses, 10 relapses (29.4%) occurred in patients who had discontinued immunosuppression. In 3 patients (8.8%), only immunosuppressive agents including AZA (n = 1), methotrexate (n = 1), and mizoribine (n = 1) were used after PSL was stopped. In another 21 patients (61.8%), 14 (41.2%) were prescribed only PSL after immunosuppressive agents were stopped, while 7 (20.6%) were prescribed PSL and immunosuppressive agents including AZA (n = 2), CYC (n = 3), cyclosporine (n = 1), and mizoribine (n = 1) at the time of relapse.
At relapse, the steroid dose was increased in all of the patients and the immunosuppressive agent was changed in 8 (23.5%), indicating an intention to treat at relapse. PSL dose was increased from 6 mg (IQR 0–10) to 20 mg (IQR 15–30) and was continued for about 2 weeks to 1 month and gradually tapered. Of the 8 patients with a change in immunosuppressive therapy, 1 was changed from mizoribine to oral CYC, 5 received newly added AZA, 1 received added CYC, and 1 received newly added intravenous CYC. After treatment, 30 patients (88.2%) re-achieved remission.
Five (15.6%) of the 32 patients who received permanent dialysis experienced relapse. All patients who experienced relapse had general symptoms, while some experienced pulmonary hemorrhage (n = 2), multiple cerebral infarction/cutaneous lesions (n = 1), or polyarthritis (n = 2). At relapse, the ANCA levels of all the patients who had received dialysis were elevated, and the patients were treated by increasing the dose of prednisone only.
Remission and ANCA levels
Among 118 patients with remission, 94 patients (79.7%) achieved negative ANCA level. In the other 24 patients (20.3%), the ANCA level remained positive, although in all of the patients, the level decreased compared with that at baseline.
Relapse and ANCA levels
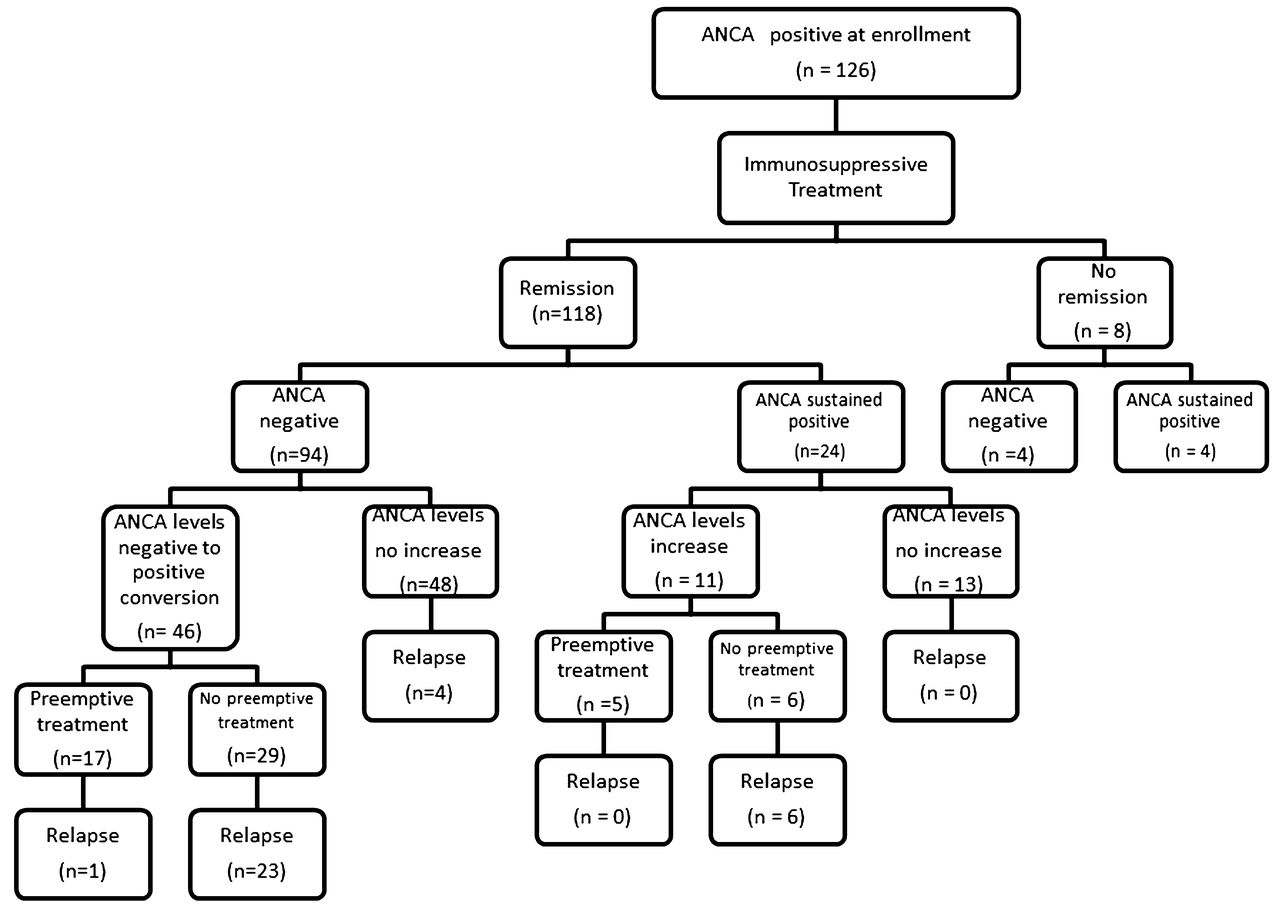
Among 94 patients with remission who achieved negative ANCA levels, negative-to-positive ANCA level conversion was found in 46 (48.9%; Figure 2). Among them, 17 patients (37.0%) received immunosuppressive medications preemptively, while 29 (63.0%) did not receive treatment increases. Immunosuppressive therapy changes included increasing PSL (n = 15), changing the immunosuppressive agent (n = 1), and increasing the dose of immunosuppressive agents (n = 1). Among the 17 patients who received preemptive immunosuppressive therapy after negative-to-positive ANCA level conversion, only 1 relapse (5.9%) was observed; meanwhile, in those who did not receive preemptive therapy following rising levels, 23 patients (79.3%) relapsed. Among the 48 patients who sustained negative ANCA levels after remission, only 4 relapsed (8.3%).
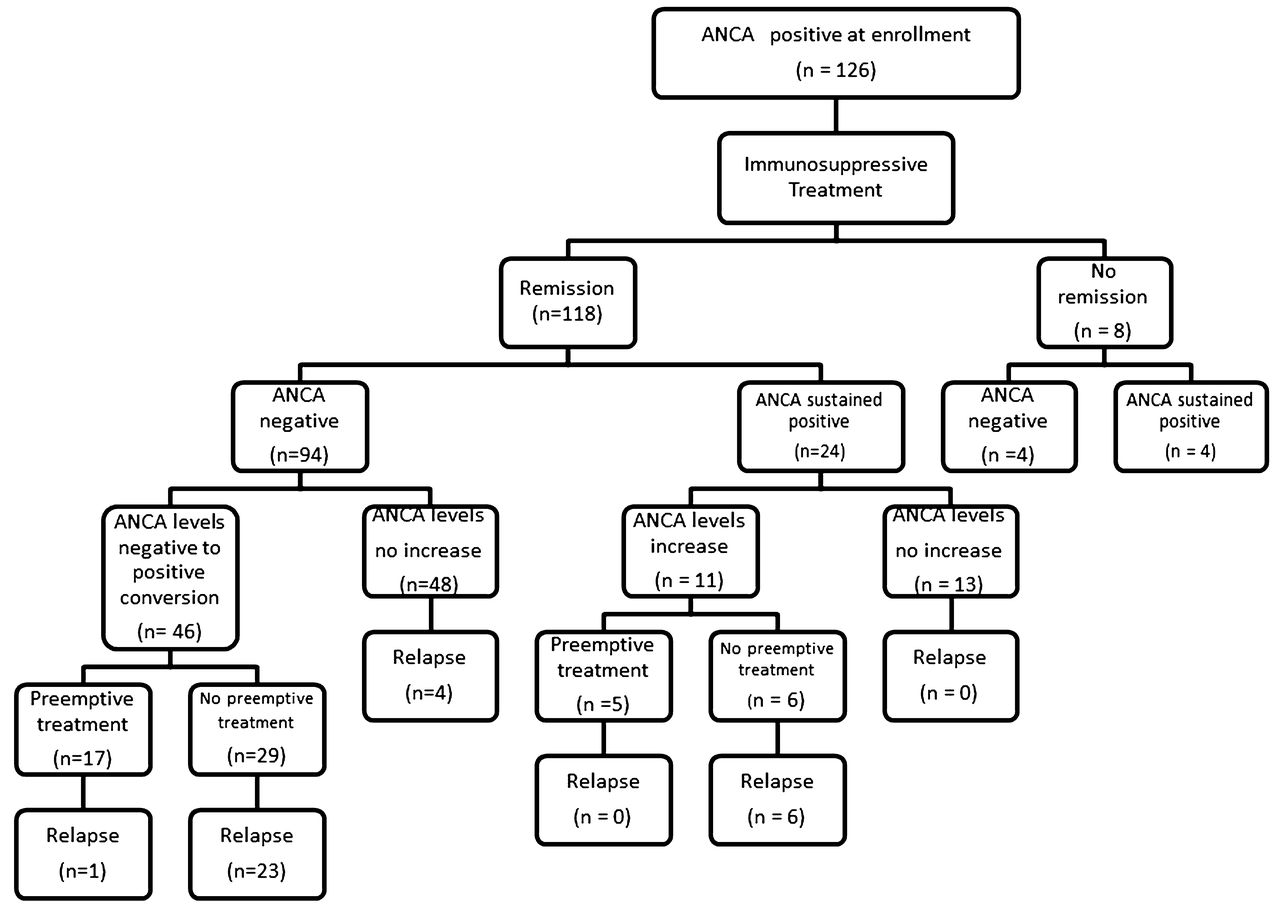
Antineutrophil cytoplasmic antibodies (ANCA) levels and preemptive treatment.
Among the 118 patients with remission, ANCA levels did not become negative in 24 (20.3%), although they had decreased from baseline levels. Among them, 11 patients (45.8%) developed ANCA level increases, and among these 11 patients, 5 (45.4%) received immunosuppressive medications preemptively and 6 (54.5%) did not receive increased treatment. Among the 5 patients who received preemptive immunosuppressive therapy, none relapsed; meanwhile, among those who did not receive preemptive therapy following ANCA level increases, all 6 patients relapsed.
Preemptive treatment and relapse
An increase in ANCA level was observed in 57 patients, including 46 with negative-to-positive ANCA level conversion and 11 with a 100% increase. Among these 57 patients, 22 received preemptive treatment, resulting in only 1 relapse (4.5%). Meanwhile, in the other 35 patients who did not receive preemptive treatment, 29 relapses were observed (82.9%). The median time from ANCA level increase to relapse was 0.6 months (IQR 0–2.1 mos). In 6 patients (17.6%), ANCA level increased concurrent with relapse. The longest interval from ANCA level increase to relapse was 10.1 months.
The rate of adverse events including death and infection was not significantly different between patients who received and did not receive preemptive treatment at the time of ANCA level increase (p = 1.000 and p = 0.767, respectively).
Endstage renal disease, hospitalization, and death
A total of 32 patients (25.3%) progressed to endstage renal disease requiring permanent dialysis, and 29 patients (23.0%) died during followup. The causes of death included infection (n = 15), vasculitis (n = 3), malignancy (n = 3), cerebrovascular diseases (n = 3), and other diseases (n = 5). Among those who died, 14 patients (43.8%) were dialysis-dependent. Hospitalization was required for infection (n = 38), aseptic osteonecrosis (n = 4), and cardiovascular diseases (n = 7).
Predictors of relapse
Time-dependent Cox regression models adjusted for clinically relevant factors showed that lung involvement (adjusted HR 2.29, 95% CI 1.13–4.65, p = 0.022) and an increase in ANCA level (adjusted HR 17.4, 95% CI 8.42–36.0, p < 0.001) were significantly associated with first relapse (Table 3). After excluding 3 PR3-ANCA–positive patients, the results were not significantly altered. However, the absolute value of the ANCA level was not associated with relapse (adjusted HR 1.00, 95% CI 1.00–1.00, p = 0.163).
Predictors of relapse. Adjusted for baseline characteristics (i.e., age, sex, lung involvement, and serum creatinine level) and followup data (i.e., ANCA level and immunosuppressive therapy including PSL, per 1.0 mg/day, and use of immunosuppressive agents).
DISCUSSION
The results show that an increased ANCA level is associated with an increased risk of relapse in Japanese patients with AAV. In contrast to previous studies, our present study included a majority of patients with MPA, and all the patients had kidney involvement. Our study also includes one of the largest sample sizes of patients with this disease ever reported, and the results are based on time-dependent Cox regression models. The results of our present study were compatible with those of recent literature19, and highlighted the clinical importance of ANCA level in predicting disease activity in renal AAV.
Some studies including small numbers of patients with AAV came to the same conclusions as our present study, i.e., persistently high or increasing ANCA levels are associated with an increased risk of disease relapse17. In contrast, other studies suggest that there is only a weak association between an increase in ANCA level and relapse; 1 of these studies was performed in a clinical trial cohort of 156 patients with serum samples drawn and ANCA assays performed at 3-month intervals20. Therefore, that study may have failed to demonstrate an independent association between ANCA level increase and AAV relapse because of the long measurement intervals. Further, a systematic review of AAV did not conclude that serial ANCA levels have clinical use29; therefore, the authors of that study recommended that instituting therapy should only be considered if there was unequivocal evidence of clinical relapse. A recently published study reported that longitudinal ANCA measurements may be useful in patients with renal involvement but were less useful in patients with nonrenal disease19. The results of our present study are actually consistent with the literature. However, in previous studies, patients with GPA were also included; and it remains to be confirmed whether these previous results are applicable to patients with MPA presenting mainly with kidney involvement. Our present study shows that an increase in ANCA level is associated with relapse in patients with AAV, which mainly included patients with MPA with kidney involvement; moreover, most patients with an increase in ANCA level without preemptive immunosuppressive therapy relapsed, whereas most patients with increases in ANCA level with preemptive therapy did not relapse. There is at present 1 randomized controlled trial performed by using such an approach, showing that preemptive therapy with CYC prevents relapses30, similar to the results of our present study.
On the other hand, the British Society for Rheumatology guideline31 recommends closely following patients with increasing ANCA levels, but not altering their therapy unless there are clear clinical signs of active disease; this is because therapies for AAV, including aggressive courses of corticosteroids and cytotoxic agents, may incur a substantial risk of adverse events, such as severe infections or malignancy. Thus, treating all patients with increased ANCA levels would result in unnecessary toxicity risks. Accordingly, the use of elevated ANCA levels as the sole measure to justify immunosuppressive therapy cannot be endorsed. However, given that patients who experience relapse have a considerable risk of developing serious damage10,32, including pulmonary hemorrhage and progressive renal insufficiency, and because our findings show that relapses can be prevented, preemptive treatment in patients who develop increasing ANCA levels during remission might be a reasonable strategy for such patients to avoid relapse and the serious consequences of AAV. In our present study, most physicians took into account the change in ANCA levels during the observation period and usually intensified immunosuppressive therapy shortly after ANCA level increased; meanwhile, in patients with decreasing levels, the dosages were correspondingly reduced. Patients with persistently high levels were treated more aggressively than patients whose levels decreased.
Actually, the rate of adverse events was not significantly different between patients who received and did not receive preemptive treatment at the time of ANCA level increase. This suggests that this strategy could suppress the occurrence of severe relapse. Therefore, we posit that the benefits of preemptively increasing immunosuppressive treatment largely outweigh the risks. However, the number of patients who were preemptively treated is too small to conclude that this is a “safe” strategy, and therefore this finding should be validated by another study.
Remarkably, 4 patients relapsed with a negative ANCA. One patient showed a serum creatinine increase and CRP elevation, 1 had fever and a serum creatinine increase, 1 had polyneuropathy and CRP elevation, and 1 had polyarthritis and fever. All of the patients received increased steroid dosage, and 3 of 4 patients achieved re-remission. The remaining 1 patient achieved CRP-negative status, but the symptom of polyneuropathy did not recover. The clinical course that responded to a steroid increase was compatible with vasculitis rather than infection.
Regarding the regimen of immunosuppressive therapy, PSL monotherapy was a frequently used treatment for AAV in our cohort. However, PSL alone is relatively ineffective in patients with AAV, and deaths were less frequent when patients were treated with both PSL and immunosuppressive drugs. Therefore, a regimen consisting of PSL in combination with CYC is recommended33. Use of glucocorticoid monotherapy is not a typical standard of care treatment approach and may have affected the findings. Moreover, we still need to investigate the reason for the good prognosis of these patients, despite most of them receiving only monotherapy with low-dose PSL for remission, in contrast to the practice in Europe and the United States. There may be racial differences in response to immunosuppressive therapy, although the mechanism is unknown. This point needs to be investigated in large, well-characterized cohorts.
The best time to examine the ANCA level is unknown. In our present study, ANCA levels were checked almost every month, and the time from ANCA level increase to relapse was relatively short (median 0.6 mos, IQR 0–2.1 mos). Although there were few patients who relapsed without any increase in ANCA level, measurements at shorter intervals would be informative because the frequency of relapse in patients with increasing ANCA levels who were not treated preemptively was very high.
The target cutoff of ANCA level to administer preemptive treatment remains unclear. Our present study did not identify an absolute ANCA level as a predictor of relapse in patients with AAV. This may suggest that the trend of ANCA level in a given patient is more important than the absolute value. The generalizability of our results should be confirmed by another cohort study, and further studies are needed to determine which patients with increasing ANCA level should be treated preemptively.
Importantly, relapse occurred in patients already receiving dialysis more frequently in our study than a previous study34. All of the patients who experienced relapse had increased ANCA levels without any preemptive therapy, suggesting ANCA level should be monitored during followup in dialysis patients, because this may provide a better guide to initiating increased immunosuppressive therapy.
Our present study has certain limitations. First, it is a retrospective analysis, so treatment regimens were not standardized and sampling intervals for ANCA level were inconsistent. Therefore, the results should be corroborated by a well-designed prospective cohort study. Second, our study assessed the first relapse in patients with AAV and not multiple relapses in patients with AAV with frequent relapses. A similar finding of ANCA level increasing for multiple relapses in patients with AAV with frequent relapses remains to be observed. Third, it should be acknowledged that disease assessment may have been biased by the treating physician’s knowledge of the ANCA status. Fourth, because of the retrospective nature of our present study, we could not determine the basis for starting immunosuppressive therapy. Further, bias could be present because of the retrospective evaluation of BVAS in all of the patients. Finally, results may have differed owing to the different ELISA kits used or the changing of the ELISA kits used in each center. Therefore, the ANCA detection method was not standardized. This could be a major limitation of our study.
An increase in ANCA level during remission was associated with risk for disease relapse. A rise in ANCA level may be useful for guiding treatment decisions in appropriate subsets of patients with AAV.
Acknowledgment
We are grateful for the time and effort of the following nephrologists who supported our study: Dr. Shizunori Ichida, Dr. Hideaki Shimizu, Dr. Tomohiko Naruse, Dr. Hirofumi Tamai, Dr. Kei Kurata, Dr. Hirotake Kasuga, Dr. Arimasa Shirasaki, and Dr. Makoto Mizutani.
Footnotes
Supported in part by a Grant-in-Aid for Progressive Renal Diseases Research, Research on Rare and Intractable Disease, from the Ministry of Health, Labor, and Welfare of Japan.
- Accepted for publication June 15, 2015.








{kind=link}
{kind=link}