

Abstract
Objective. Analyses were conducted to examine the baseline burden of illness and compare the effect of etanercept (ETN) versus placebo (PBO) on quality of life (QOL) in patients with nonradiographic axial spondyloarthritis (nr-axSpA) who failed nonsteroidal antiinflammatory drugs (NSAID).
Methods. Patients fulfilling the Assessment of Spondyloarthritis International Society axSpA criteria, not meeting the modified New York criteria for ankylosing spondylitis (AS), who were symptomatic 3 months to 5 years, with a Bath AS Disease Activity Index score ≥ 4, and failed ≥ 2 NSAID were randomized to ETN 50 mg weekly or PBO (double-blind) for 12 weeks, followed by open-label ETN 50 mg for 92 weeks. Stable NSAID were allowed throughout our study. QOL outcomes over 24 weeks were analyzed using ANCOVA models.
Results. At baseline, Multidimensional Fatigue Inventory (MFI; ETN mean 14.7, PBO mean 15.0), EQ-5D utility (0.52, 0.57), EQ-5D visual analog scale (56.5, 56.4), and Medical Outcomes Study (MOS) Sleep Index II (45.5, 48.1) were worse than population norms (6.6–8.0, 0.86, 82.5, and 25.8, respectively). At Week 12, Bath AS Patient Global Score, nocturnal and average back pain, MOS Short Form-36 (SF-36) physical component, and Work Productivity and Activity Index (WPAI) presenteeism and activity impairment favored ETN (p < 0.05). Nonsignificant improvements for ETN were seen in other WPAI domains, MFI, MOS-Sleep Index I and II, Hospital Anxiety and Depression Scale, EQ-5D utility score, and SF-36 mental component (p > 0.05). At Week 24, patients in the PBO group who had switched to ETN at Week 12 showed improvement in most QOL assessments, similar to that seen in patients receiving ETN for 24 weeks.
Conclusion. Improvements favored ETN in QOL and productivity measures, with limited improvement on general QOL measures. Short disease duration, a short PBO-controlled period, and a wide range of QOL scores at baseline may have influenced improvements.
- ETANERCEPT
- QUALITY OF LIFE
- WORK
- SPONDYLOARTHROPATHIES
- NONRADIOGRAPHIC AXIAL SPONDYLOARTHRITIS
- TUMOR NECROSIS FACTOR-α
In 2009, the Assessment of Spondyloarthritis International Society (ASAS) recognized the need to define a subgroup of patients with spondyloarthritis (SpA) who have axial disease (axSpA)1,2,3. Patients are included in this subgroup according to either imaging or clinical criteria. To meet the imaging criteria, patients are required to have acute inflammation on magnetic resonance imaging (MRI) or definite sacroiliitis on radiograph4 and at least 1 SpA feature. To meet the clinical criteria, patients do not need to have sacroiliitis on imaging, but need to be positive for HLA-B27 and have at least 2 other SpA features. Those who meet the axSpA criteria without radiographic evidence are defined as nonradiographic axSpA (nr-axSpA)1,2,3.
Considering the recent classification of nr-axSpA, data are limited on its place within the matrix of SpA and ankylosing spondylitis (AS), including its natural progression, outcomes, and treatment response. Progression of nr-axSpA to radiographic SpA has been estimated to be about 10% over 2 years and about 20% in patients with C-reactive protein (CRP) positivity and/or active inflammation on MRI of the sacroiliac (SI) joints at baseline5. The exact interrelationship between nr-axSpA and AS has not been established, with evidence and opinions supporting theories that nr-axSpA may be a mild form of AS, earlier on the disease progression continuum to AS, separate and distinct entities, or different but overlapping entities5,6,7,8,9.
Despite these unknowns, published findings identify nr-axSpA as having similar levels of disease activity, pain, and fatigue as those with established, radiographically visible axSpA and similar symptoms and burden of disease as those with AS10,11,12,13,14. In general, axSpA causes permanent structural changes, leading to progressive disability, and is associated with significant pain, fatigue, impaired physical function, limited spinal mobility, work disability, and an overall diminished health-related quality of life (HRQOL)10. The effect of axSpA on patient health can be extensive, with the potential for progressive deformity and subsequent loss of function, limiting a person’s ability to work productively and to carry out normal daily activities, thus causing significant health and socioeconomic burdens for the patient and society10.
The current standard of care in the treatment of axSpA includes therapy with nonsteroidal antiinflammatory drugs (NSAID) or antitumor necrosis factor (anti-TNF) agents recommended for patients who are unresponsive to NSAID15,16,17,18. Little is known, however, regarding the potential benefits of anti-TNF in patients who fall into the nr-axSpA classification, and limited data exist on their effect on QOL7,19. However, early treatment with anti-TNF therapy has been established in other rheumatic diseases to improve mobility and QOL, and reduce the overall progression of disease. The objective of this analysis was to examine the baseline burden of illness and compare the effect of etanercept (ETN) versus placebo (PBO) on QOL in patients with nr-axSpA who had an insufficient response to NSAID.
MATERIALS AND METHODS
Patients and study design
Our ongoing nr-axSpA study was a multicenter, double-blind, 2-period, randomized phase IIIB clinical controlled trial conducted in 14 countries in Europe, Asia, and Latin America beginning May 2011, with interim data presented herein through February 2013 (ClinicalTrials.gov NCT01258738). Eligible patients were aged ≥ 18 to < 50 years and satisfied the ASAS classification criteria for axSpA; they did not meet the modified radiographic 1984 New York criteria for AS3. Eligible patients also had a symptom duration of > 3 months to < 5 years, active disease defined by a Bath AS Disease Activity Index (BASDAI) score ≥ 4, and inflammatory back pain. Patients were unresponsive to at least 2 NSAID taken separately for a total combined duration of more than 4 weeks. NSAID therapy had to be at a stable, optimally tolerated dose for at least 14 days prior to study baseline.
MRI were performed locally, collected, and read by 1 of 2 central readers to evaluate the presence of SI joint inflammation. Positive sacroiliitis was defined as active inflammatory lesions of the SI joints with definite bone marrow edema/osteitis, suggestive of sacroiliitis associated with SpA based on the ASAS criteria for a positive MRI status3. Patients who did not have inflammation based on MRI readings and were HLA-B27−negative did not meet the ASAS-defined axSpA classification and were excluded from our study. Additional details regarding inclusion and exclusion criteria of our study have been reported elsewhere20.
Enrolled patients were randomized (1:1) to receive either ETN 50 mg once weekly (QW) subcutaneously or PBO double-blind for 12 weeks. Patients in both treatment groups continued their background NSAID therapy at stable, optimal, tolerated dosages as determined by the study investigator. All patients who completed the 12-week, double-blind period were eligible to enter into a 92-week, open-label treatment period in which all patients received ETN 50 mg QW plus their respective background NSAID therapy.
In both the double-blind and open-label periods, chronic use of only 1 NSAID at a time was permitted at stable, optimal doses. In the double-blind period, if patients could not tolerate NSAID therapy, it could be reduced or discontinued for up to 2 weeks, but those who were still intolerant upon restarting, even at a lower dosage, were discontinued from our study. In the open-label period, NSAID therapy could be reduced, substituted with another NSAID of equivalent antiinflammatory dosage, or discontinued.
Assessments
Health outcomes assessments were conducted to explore the patients’ own perceptions about their level of disease activity, effect of disease on productivity, and HRQOL. Patients completed all questionnaires using pen and paper. These questionnaires were completed prior to any procedures being performed at the visit, if possible. Every effort was made to obtain unbiased responses from the patients; site staff and the investigator did not influence the patients’ responses.
HRQOL findings from the 12-week, double-blind, randomized period and the first 12 weeks of the open-label period (i.e., to Week 24) are reported herein and are grouped into 4 general categories: (1) general well-being/fatigue/pain, (2) utility/HRQOL, (3) work productivity, and (4) sleep/anxiety/depression. Specific assessments in each QOL category are listed in Table 1. BASDAI, Bath AS Functional Index (BASFI), Bath AS Metrology Index (BASMI), patient’s global assessment of disease activity, total back pain score, and duration of morning stiffness have been previously reported in the primary analysis20. For study sites in Russia and the Czech Republic, only select questionnaires were translated (BASDAI, BASFI, patient’s assessment of disease, total pain, and nocturnal back pain assessments), which resulted in lower patient numbers for some QOL assessments. QOL analyses were conducted in the modified intent-to-treat (mITT) population, defined as all randomized patients who met the ASAS classification criteria for axSpA, received ≥ 1 dose of study drug, and had ≥ 1 on-treatment assessment. The efficacy and safety results from this trial were recently published20.
Patient-reported outcomes at baseline. Modified intent-to-treat population, observed case. Data are mean (SD).
Our study was conducted in compliance with the Declaration of Helsinki, the International Conference on Harmonisation Good Clinical Practice guidelines, and all applicable local/country specific regulations. Prior to the start of our study, independent ethics committees or institutional review boards in each country or local region reviewed and approved our study, and written and informed consent were received from all patients.
Statistical analyses
Between-group statistical comparisons on adjusted mean values were only performed for the first 12 weeks of our study using an ANCOVA model with treatment, MRI sacroiliitis positive/negative, and geographic region as factors and baseline score as a covariate. For timepoints after 12 weeks, unadjusted mean values were evaluated using descriptive statistics because all patients were receiving open-label ETN 50 mg QW. Categorical endpoints were analyzed using the Cochran-Mantel-Haenszel chi-square test, stratified by MRI sacroiliitis positive/negative and geographic region. Observed cases analyses were conducted.
RESULTS
During the 12-week, double-blind study period, a total of 225 patients were randomized and 224 received the study drug. Of these, 9 patients did not satisfy the ASAS criteria, and a total of 215 patients (ETN, n = 106; PBO, n = 109) were included in the mITT population. A total of 206 patients (ETN, n = 100; PBO, n = 106) completed the double-blind period (Week 12), with 9 patients discontinuing the study (ETN, n = 6; PBO, n = 3). The majority of discontinuations were caused by adverse events (n = 4), followed by protocol deviations (n = 2) and no longer being willing to participate in the study (n = 3). Of these, 205 patients entered the open-label period (1 patient completed Week 12, but did not continue to receive open-label treatment), and 198 patients reached the 24-week timepoint (ETN/ETN, n = 96; PBO/ETN, n = 102). Through the first 12 weeks of the open-label period, 7 patients discontinued the study (ETN/ETN, n = 4; PBO/ETN, n = 3), with the majority of discontinuations attributable to being no longer willing to participate (n = 3) and 1 patient each because of adverse events, lost to followup, protocol deviation, and insufficient clinical response.
Demographic and disease characteristics were well balanced between the ETN and PBO groups at baseline, with no significant between-group differences observed20. Of the 215 patients in the mITT population, baseline mean (SD) age was 32.0 years (7.8), 60.5% were men, 73.5% were white, mean disease duration was 2.4 years (1.8), and mean CRP level was 6.6 (10.5) mg/l20. The most common ASAS classification criteria feature was inflammatory back pain (88 patients, ETN group; 92 patients, PBO group). In our study, 82.1% patients in the ETN group and 79.8% patients in the PBO group had sacroiliitis on MRI and ≥ 1 SpA feature, satisfying the ASAS criteria for the imaging arm; the remaining patients did not have sacroiliitis on MRI, but were HLA-B27−positive with at least 2 SpA features, fulfilling the criteria for the clinical arm.
General well-being, fatigue, and pain
Patients’ general well-being, fatigue, and pain at baseline indicate a moderate to compromised unfavorable effect on HRQOL and moderate to severe disease activity (Table 1). At baseline, the Multidimensional Fatigue Inventory (MFI) general scores were 14.7 for the ETN group and 15.0 for the PBO group, which were worse than the population norms of 6.6 to 8.021.
A statistically significant improvement in adjusted mean change from baseline was seen in the ETN group for Bath AS Patient Global Score (BAS-G) and nocturnal and average back pain compared to PBO after 12 weeks of treatment (p < 0.05). All MFI items demonstrated improvement from baseline after the double-blind period at Week 12 in both treatment groups with no statistically significant differences observed between groups (Table 2). The MFI items largely remained steady in the ETN/ETN group through Week 24 over the course of the open-label period. MFI response improved in patients who switched from PBO to ETN treatment at Week 12 (no significant between-group differences) and reached a response at Week 24 that was comparable with those observed in patients who continued with ETN.
Improvements in patient-reported outcomes at weeks 12 and 24. Modified intent-to-treat population, observed case.
Utility scores and HRQOL
Baseline values for the EQ-5D visual analog scale (VAS) scores were 56.5 for the ETN group and 56.4 for the PBO group, and were worse than the population norm of 82.5 (Table 1)22,23. At Week 12, the ETN group demonstrated statistically significant improvements in mean percent change from baseline compared with PBO in EQ-5D VAS of 16.3% and 5.8% in the ETN and PBO groups, respectively (p < 0.05; Table 2). The EQ-5D VAS score continued to show an improving trend in the ETN/ETN group over the course of the open-label period. Patients who switched from PBO to ETN treatment at the start of the open-label period reached responses at Week 24 that were comparable with the responses observed in those who were originally randomized to ETN, which were statistically significant from baseline in both groups.
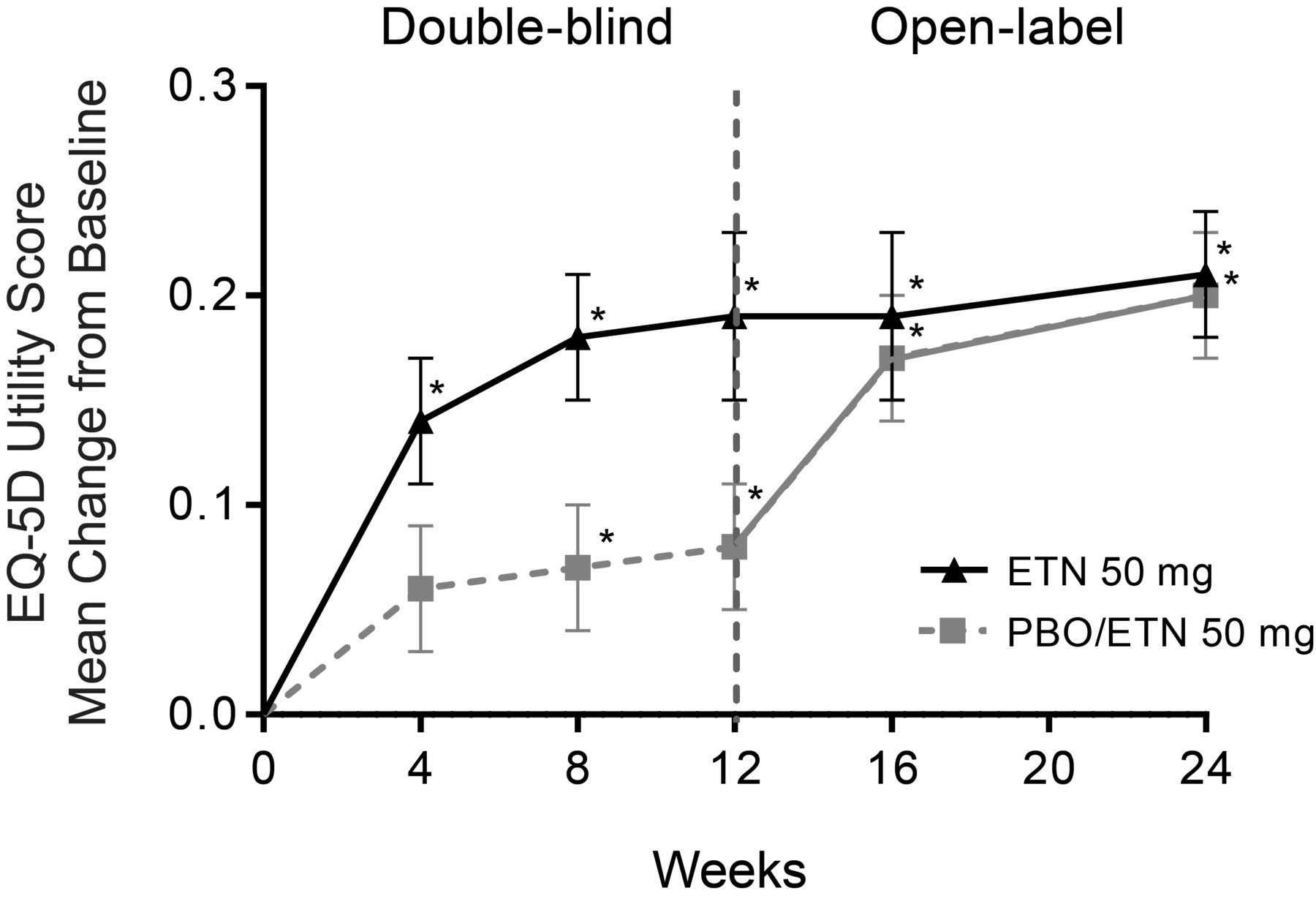
At baseline, the EQ-5D utility scores of 0.52 and 0.57 in the ETN and PBO groups, respectively, were worse than the population norm of 0.86 and similar to the preferred base utility scores of those with rheumatoid arthritis (RA; 0.39–0.60) and heart disease (0.64)22,24,25. After 12 weeks, a greater proportion of patients treated with ETN achieved the minimal clinically important difference (MCID) ≥ 0.05 (ETN 60.0%, PBO 43.0%; p < 0.05). EQ-5D utility scores improved slightly throughout the open-label period for both treatment groups with an increase in those who achieved MCID in the PBO/ETN group (ETN/ETN 59.8%, PBO/ETN 65.6%; Table 2, Figure 1).
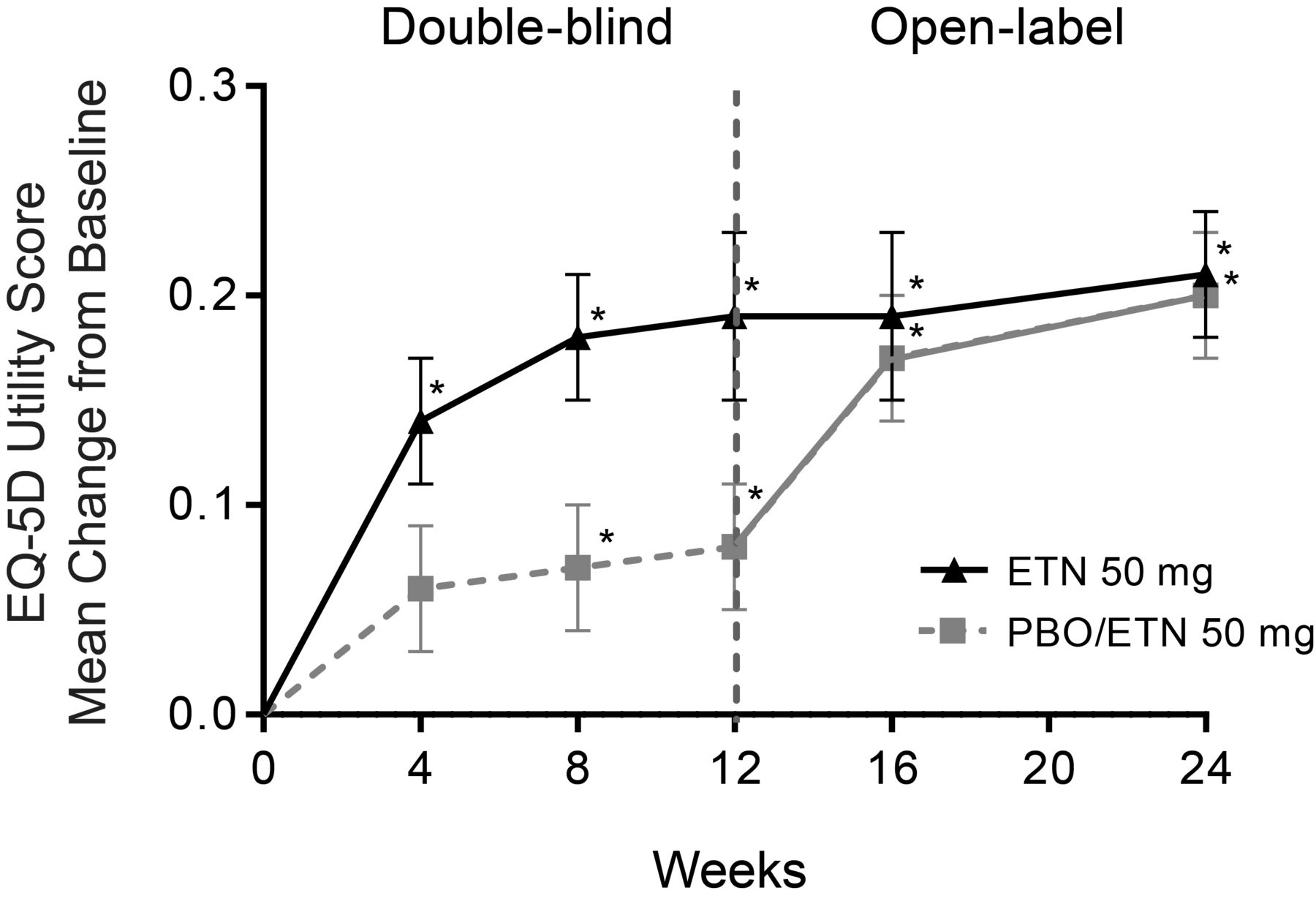
Improvement in EQ-5D use score. * p ≤ 0.05 within treatment group versus baseline. ETN: etanercept; PBO: placebo.
The Medical Outcomes Study Short Form-36 (SF-36) physical component summary (PCS) and mental component summary (MCS) scores were similar between treatment groups at baseline (Table 1). At Week 12, ETN had statistically significant improvement compared with PBO in SF-36 PCS, with no difference between treatment groups in MCS (Table 2). The SF-36 PCS continued to show an improving trend in the ETN/ETN group at Week 24 in patients who switched from PBO to ETN treatment at the start of the open-label period, reaching responses at Week 24 that were comparable with those observed in patients originally randomized to ETN. The SF-36 MCS showed a slight improvement in both treatment groups in the double-blind period that was significant from baseline at Week 24.
QOL as measured by the AS Quality of Life score (ASQOL) showed no statistically significant differences between treatment groups during the double-blind period. The mean ASQOL continued to show an improving trend in the ETN/ETN group at Week 24, with patients who switched from PBO to ETN treatment at the start of the open-label period reaching responses at Week 24 that were comparable with those observed in patients originally randomized to ETN. The proportion of patients who had minimally clinically important decrease in ASQOL scores ≥ 1.8 from baseline was not statistically significant between treatment groups during the double-blind period (ETN 48.9%, PBO 50.0%, p = 0.862). However, the proportion increased to 60.2% and 64.8% from Week 12 to Week 24 in the ETN/ETN group and PBO/ETN group, respectively.
Work productivity in patients with nr-axSpA
At Week 12, both treatment groups demonstrated a statistically significant (p < 0.05) mean change (SE) from baseline in the AS Work Instability Score (WIS) with no differences between treatment groups [ETN −2.4 (0.6) vs −1.6 (0.6), p > 0.05]. Both groups continued to show slight improving trends during the open-label phase for a mean (SE) change of −3.1 (0.6) versus −2.6 (0.6) that was significant from baseline.
At baseline, 73.3% (66/90) and 66.3% (63/95) of those in the ETN and PBO groups, respectively, were employed as measured by the Work Productivity and Activity Impairment in AS (WPAI-AS) questionnaire. The percentage of patients who were employed showed little change throughout the course of the study with 70.6% (60/85) and 68.5% (63/92) employed at Week 12, and 68.3% (56/82) and 66.3% (59/89) at Week 24, respectively.
Patients receiving ETN experienced a significantly greater improvement versus PBO in presenteeism and activity impairment, but not absenteeism or overall work impairment domains of the WPAI-AS at Week 12 (p < 0.05; Table 2). After PBO patients switched to open-label ETN, all WPAI-AS items achieved similar responses to those who originally received ETN, which were significant from baseline with the exception of absenteeism.
Sleep, anxiety, and depression
At baseline, patients with nr-axSpA indicated that they had compromised sleep as measured by MOS sleep II scores of 45.5 in the ETN group and 48.1 in the PBO group, which were worse than population norm of 25.8 (Table 1)26.
In the individual items of MOS sleep, the mean change from baseline was only statistically significantly different between the 2 treatment groups at Week 12 for sleep quantity (p < 0.05) while all other items (awakening short of breath, optimal sleep, sleep adequacy, sleep somnolence, sleep disturbance, and snoring) showed no differences and largely remained steady through Week 24.
At baseline, the Hospital Anxiety and Depression Scale (HADS) scores for anxiety and depression were within the 0 to 7 normal range for these symptoms27. No statistically significant differences were noted between the treatment groups in HADS anxiety and depression after the double-blind phase at Week 12. Slight improvements were observed through Week 24 that were significant from baseline in both treatment groups for HADS anxiety and depression (p < 0.05).
DISCUSSION
Treatment with ETN in patients with nr-axSpA who had an inadequate response to ≥ 2 NSAID provided significant improvement in patient-reported outcome (PRO) measures for disease-specific, functional, and productivity domains such as BAS-G, WPAI, SF-36 (PCS), and nocturnal and average back pain compared with PBO. The continued improvement observed in the open-label period is consistent with the pattern of health outcomes seen with other indications (RA, AS, psoriatic arthritis, and psoriasis)28,29,30,31,32.
At Week 12, ETN showed significant differences compared with PBO in a variety of PRO measures, in particular items related to physical and functional activities. As expected, clinically meaningful improvements were observed once patients were switched from PBO to ETN at the beginning of the open-label period. Improvements in PRO in the open-label period for this group were generally comparable with or in some cases exceeded those observed for the patients who received ETN for the first 12 weeks. At the 24-week timepoint, regardless of treatment assignment at baseline, the health outcomes responses achieved were largely comparable.
Significant differences from baseline were observed in the ETN group for EQ-5D VAS and SF-36 PCS scores, and MCID was achieved in EQ-5D utility improvement. Although comparison of results observed across different clinical trials may be hazardous, the magnitude of treatment effect of ETN versus PBO for PRO, such as EQ-5D and SF-36 in our study in nr-axSpA, appears to be similar to that previously reported in radiographic axSpA (i.e., AS)28,33. Such similarities in the magnitude of treatment effect in patients with or without structural damage of the SI joints have been reported with other anti-TNF therapies and strongly support the benefit of this class of drugs in the entire axSpA spectrum34,35,36,37. In our present study of nr-axSpA, limited improvement was observed in general PRO measures such as sleep, fatigue, and anxiety/depression scales (ASQOL, AS WIS, and HADS). Data from previous clinical trials for AS in anti-TNF therapy have shown marked improvement in the domain of fatigue, but in our trial for patients with nr-axSpA, limited improvement was observed28,38,39. It is unknown whether the natural history of nr-axSpA is associated with higher levels of anxiety and depression and/or lower levels of general well-being. Short disease duration, a short PBO-controlled period, and a wide range of PRO scores at baseline may have influenced relative improvements.
Overall, PRO measures in patients with nr-axSpA continued to improve up to 24 weeks in patients who received ETN treatment throughout the double-blind and open-label periods with little or no notable plateau.
Footnotes
Funded by Pfizer Inc. W. Tsai and D.L. Saaibi were principal investigators for the clinical trial used in this analysis and have received consulting fees unrelated to the development of this manuscript. M. Dougados has received consultancy fees and has participated in symposia organized by Pfizer, both unrelated to the development of this manuscript. R. Bonin, J. Bukowski, R. Pedersen, B. Vlahos, and S. Kotak are employees of Pfizer. Medical writing support was provided by Stephanie Eide of Engage Scientific Solutions and was funded by Pfizer.
- Accepted for publication June 29, 2015.








{kind=link}