

Abstract
Objective. To determine the predictive value of functional autoantibodies against vascular receptors for the development of ischemic digital ulcers (DU) in patients with systemic sclerosis (SSc).
Methods. Angiotensin II Type 1 receptor (AT1R) and endothelin 1 Type A receptor (ETAR) autoantibodies were measured at baseline in a prospective cohort of 90 patients with SSc together with 5 validated angiogenic markers. The primary outcome was the occurrence of at least 1 new ischemic DU during the 5-year followup.
Results. Twenty-four patients developed at least 1 new DU during the followup period. Univariate Cox analysis revealed that concentrations above the median value of anti-AT1R and anti-ETAR antibodies were predictive of the occurrence of ischemic DU (HR 2.85, 95% CI 1.19–6.84 and HR 3.39, 95% CI 1.35–8.50, respectively). A first multivariate Cox analysis including functional autoantibodies and clinical predictors of new DU confirmed anti-ETAR autoantibodies as independent predictors of the occurrence of new ischemic DU (HR 3.15, 95% CI 1.22–8.13) together with a history of DU at baseline. In a second model implemented with angiogenic markers, anti-ETAR autoantibodies remained an independent predictor of the occurrence of new ischemic DU (HR 9.59, 95% CI 1.75–52.64) together with the presence at baseline of active DU or history of DU.
Conclusion. Anti-ETAR autoantibodies can be used together with the presence of current or past DU to identify patients with SSc who are at risk for the development of subsequent DU. These autoantibodies may allow for earlier management and therapeutic intervention.
Systemic sclerosis (SSc) is a connective tissue disease characterized by widespread vascular lesions and fibrosis of the skin, internal organs, and small vessels1. Microvascular alterations are key features of SSc, underlying many disease manifestations including ischemic digital ulcers (DU)2. DU are frequent in SSc, averaging 30% prevalence according to the EUSTAR (European League Against Rheumatism Scleroderma Trials and Research group) registry, and represent a heavy burden because of their major effect on quality of life3,4,5,6,7. In addition, DU are thought as a clinical variable of severe vasculopathy that can be associated with or predict other vascular lesions7,8,9. Treatment of DU remains challenging and the identification of reliable predictors of DU is still a clinical need in SSc4,5. So far, a past history of DU appears as the strongest risk factor for subsequent DU. We have previously shown that angiogenic markers may predict the occurrence of DU in SSc10. In parallel, a cross-sectional study reported an association between DU and functional autoantibodies against angiotensin II Type 1 receptor (AT1R) and endothelin 1 Type A receptor (ETAR)11,12. Therefore, our aim was to examine prospectively the value of these functional autoantibodies against vascular receptors to predict the occurrence of DU and compare it with other markers, including clinical variables and angiogenic markers.
MATERIALS AND METHODS
Design
Prospective observational cohort study.
Study population
Unselected patients with SSc hospitalized in the Rheumatology A Department, Cochin Hospital, Paris, for routine followup of the disease with available serum samples. Patients treated with angiotensin-converting enzyme (ACE) inhibitors and endothelin receptor antagonists were excluded. Our study complied with the recommendations of the Declaration of Helsinki, and all patients granted their informed consent to undergo the study-related procedures that were approved by the local Ethics Committee.
Setting
First visit between September 2007 and November 2008. Patients were then seen by his/her usual physician on a regular basis of 3- to 6–month intervals, as indicated by their disease severity, and were hospitalized at least annually for systemic evaluation. The final study observation was planned as the last observation of the last trimester of the year 2013 (or the last available observation) or the last observation at the time of death from any cause, with analyses and completion of the database performed during the first trimester of the year 2014.
Main outcome measure
The main outcome measure was the occurrence of the first new ischemic DU, defined by a painful area ≥ 2 mm in diameter with visible depth and loss of dermis, amenable to healing, and in a location judged compatible with a vascular etiology, defined in our study as volar surface of the digit distal to the proximal interphalangeal digital crease. DU attributable to a condition other than SSc and nonischemic DU located over subcutaneous calcifications or over extensor surfaces of joints were not taken into consideration.
Clinical and routine laboratory assessments
The following data were collected for all patients: age, sex, disease duration (date of the first non-Raynaud symptom), cutaneous subset according to the criteria reported by LeRoy, et al13, skin involvement according to the modified Rodnan skin score (mRSS)14, and treatment received.
Routine laboratory studies obtained on the morning of hospital admission included complete blood cell count, Westergren erythrocyte sedimentation rate (ESR), C-reactive protein (CRP) level, serum creatinine concentration, and tests for anticentromere and antitopoisomerase I antibodies.
Pulmonary and cardiac assessments
Echocardiography was performed by a senior cardiologist according to the American Society of Echocardiography recommendations. In particular, left ventricular ejection fraction was determined using the Simpson method and systolic pulmonary arterial pressure (sPAP) was based on the tricuspid and/or pulmonary regurgitation, adding 10 mmHg for auricular pressure. Pulmonary hypertension (PH) was suspected at baseline or during followup based on (1) an estimated echocardiographic sPAP > 40 mmHg, (2) a DLCO < 50% predicted in absence of pulmonary fibrosis, or (3) an unexplained dyspnea as previously published8,15 and had to be confirmed by right heart catheterization as a resting mean pulmonary artery pressure ≥ 25 mmHg together with a pulmonary capillary wedge pressure of ≤ 15 mmHg (precapillary PH).
Pulmonary involvement was assessed by chest radiograph, computed tomography (CT), and measurement of forced vital capacity and the diffusing capacity for carbon monoxide/alveolar volume ratio.
Functional antibody and angiogenic marker assessment at baseline
Anti-AT1R and anti-ETAR autoantibodies were detected in cooperation with CellTrend GmbH with a commercially available solid-phase assay (One Lambda Inc.) as described previously11. This ELISA was validated according to the Food and Drug Administration’s “Guidance for Industry: Bioanalytical Method Validation.” The interassay variability was 7% and the intraassay variability was 6%.
Serum levels of vascular endothelial growth factor (VEGF), placenta growth factor (PlGF), and soluble vascular cell adhesion molecule (sVCAM) were measured using the quantitative sandwich ELISA technique (Quantikine kits, R&D Systems) as previously reported10,11. Concentrations were calculated using a standard curve generated with specific standards provided by the manufacturer. Analytical ranges and intra/interassay coefficients of variation are provided in Supplementary Table 1 (available from the authors on request).
Endothelial progenitor cell and circulating endothelial cell quantification by flow cytometry
We used a method previously described and validated to enrich mononuclear cells and quantify endothelial progenitor cells (EPC) and circulating endothelial cells (CEC) by flow cytometry10,16,17.
Statistical analysis
All data are presented as median [interquartile range (IQR)] for continuous variables and numbers and percentages for categorical variables, unless stated otherwise. Data were analyzed with the Mann-Whitney U (unpaired data) test, chi-square, or Fisher’s exact test as indicated.
To estimate the cutoff of functional antibodies and endothelial markers, we compared levels of functional antibodies, EPC, CEC, VEGF, PlGF, and sVCAM between patients with SSc and a group of 20 healthy controls (15 women, 55 ± 16 yrs old) assessed during the same study period. The results revealed that the median value of functional antibodies and all angiogenic markers detected in patients with SSc were above the 95th percentile of the levels observed in the controls; therefore, to evaluate their predictive value on clinical outcomes, functional antibodies, EPC, CEC, VEGF, PlGF, and sVCAM were considered as categorical variables, and associations were assessed according to the median value of each variable, as used in a previous published study10.
The association between baseline serum levels of autoantibodies and/or angiogenic markers and the prespecified endpoints were first analyzed in univariate Cox models followed by multivariate analysis including all variables with p < 0.2 in univariate analysis. Event-free survival was evaluated using the Kaplan-Meier method. Correlations between baseline levels of endothelial markers were assessed using Spearman rank correlation test. Statistical analysis was performed with the use of Medcalc software (version 11.4.4, Medcalc software bvba) and XL STAT (v2013.6.02). Receiver-operating characteristic (ROC) curves were generated to assess the diagnostic value of functional antibodies for detecting patients with new ischemic DU.
RESULTS
Characteristics of patients with SSc at inclusion
Baseline characteristics of the included 90 patients with SSc are reported in Table 1. Ten patients died during the followup period (causes of death were pulmonary fibrosis in 6 patients, PH in 3 patients, and neoplasia in a single patient) and 7 patients were lost to followup.
Baseline characteristics of patients with SSc. Values are n (%) unless otherwise specified.
No significant difference was observed between patients with or without current or past DU at baseline regarding age at disease onset (p = 0.112), cutaneous subset (p = 0.665), sex (p = 0.136), positive anticentromere (p = 0.380), topoisomerase I antibodies (p = 0.110), increased ESR (p = 0.458), and CRP levels (p = 0.335).
Occurrence of ischemic DU
During a median followup period of 60 months, new ischemic DU occurred in 24 patients with SSc (15 patients with current or history of DU at baseline and 9 patients with no previous DU). The median time to development of new DU after study inclusion was 21 months, which is in accordance with a recent study performed with the EUSTAR registry18.
Baseline values of functional antibodies
The median (IQR) serum levels of anti-AT1R and anti-ETAR antibodies were 8.92 (4.57–12.63) and 7.24 (2.50–10.82) units, respectively. A strong correlation between anti-AT1R and anti-ETAR autoantibodies was observed (R 0.87, p < 0.001). Baseline values of anti-AT1R and anti-ETAR autoantibodies were not associated with the presence of current or past DU at baseline (p = 0.539 and p = 0.962, respectively). Anti-AT1R and anti-ETAR antibodies were associated with manifestations of fibrosis, as previously reported11: patients with above the median value of anti-AT1R and anti-ETAR antibodies were more likely to have an mRSS > 14 (p = 0.007 and p = 0.027, respectively) and pulmonary fibrosis on CT scan (p < 0.001 for both comparisons).
Predictive value of functional antibodies for the occurrence of ischemic DU
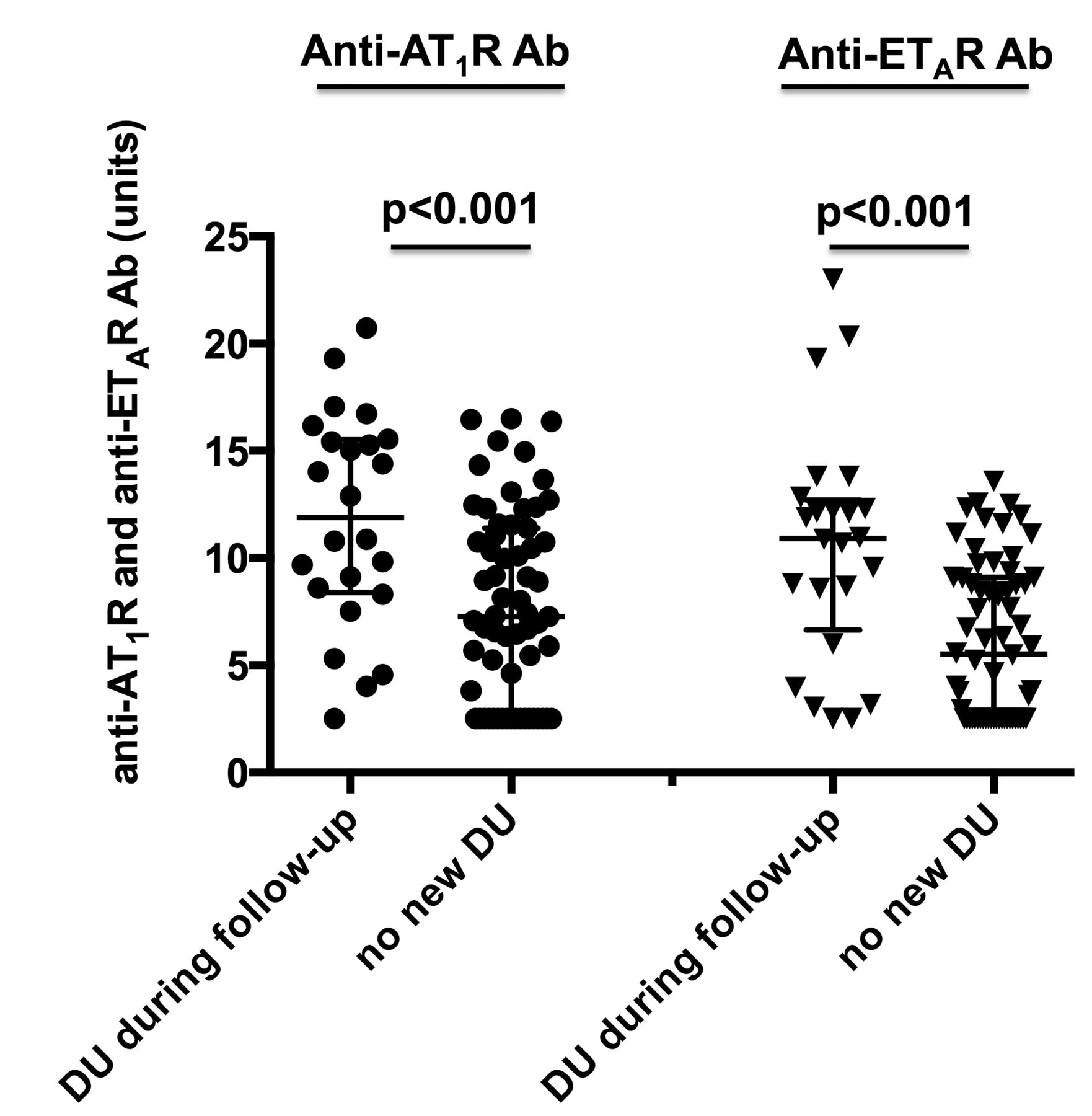
In univariate analysis, baseline serum levels of anti-AT1R and anti-ETAR antibodies were significantly higher in patients who subsequently developed new DU (medianQ1–Q3 11.888.38–15.51 vs 7.252.50–11.39 units, p < 0.001 and 10.906.64–12.70 vs 5.512.50–9.01 units, p < 0.001; Figure 1).
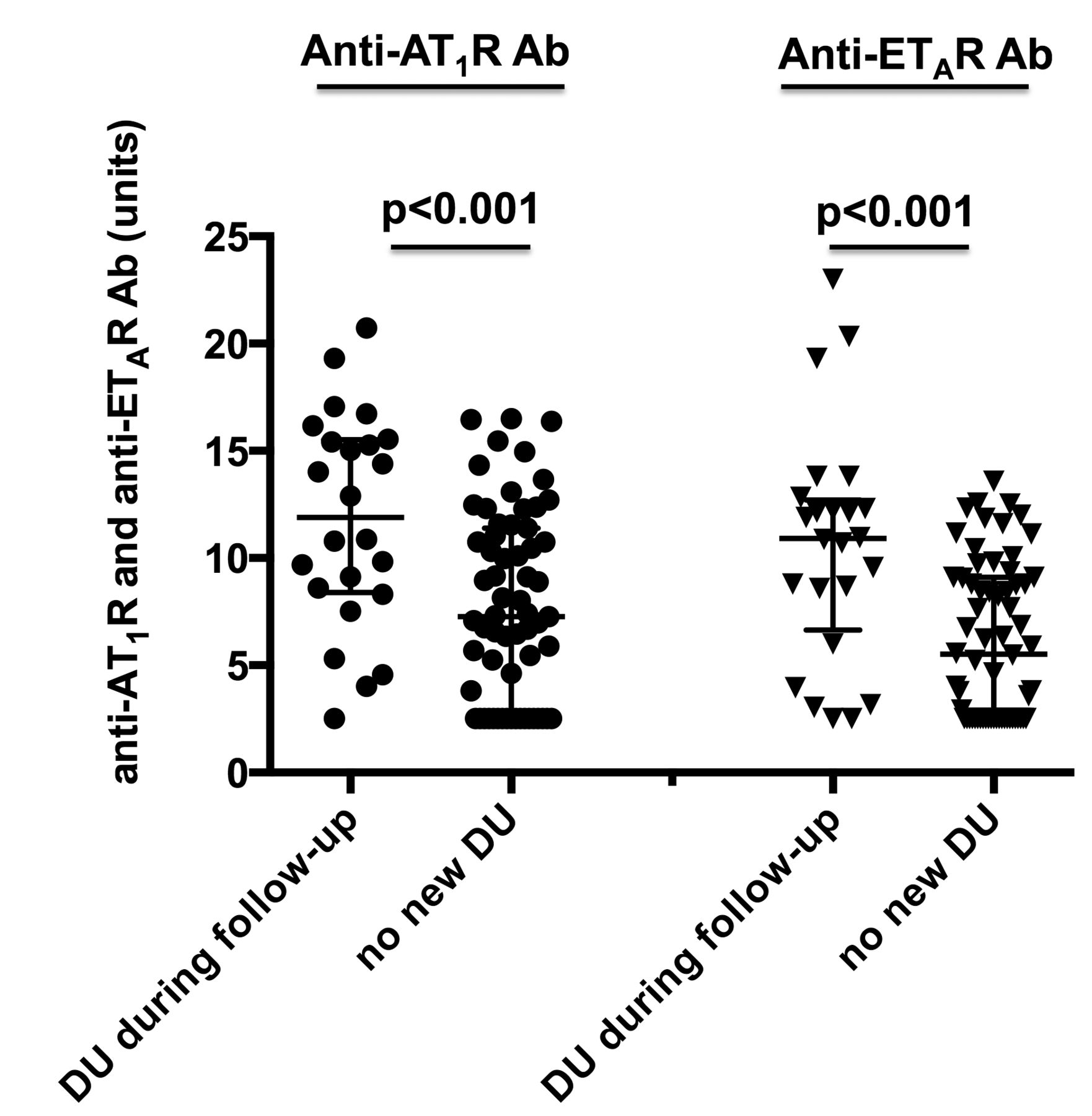
Baseline serum levels of anti-AT1R and anti-ETAR Ab according to the subsequent development of DU. Patients who developed new DU during the followup period had significantly higher median levels of anti-AT1R and anti-ETAR Ab than patients who did not develop this complication. Results are expressed by median ± interquartile range. A single data point was outside the axis limits in the group anti-AT1R antibody and no occurrence of new DU (40 units). Anti-AT1R: antiangiotensin II Type 1 receptor; anti-ETAR: antiendothelin 1 Type A receptor; DU: digital ulcers; Ab: autoantibodies.
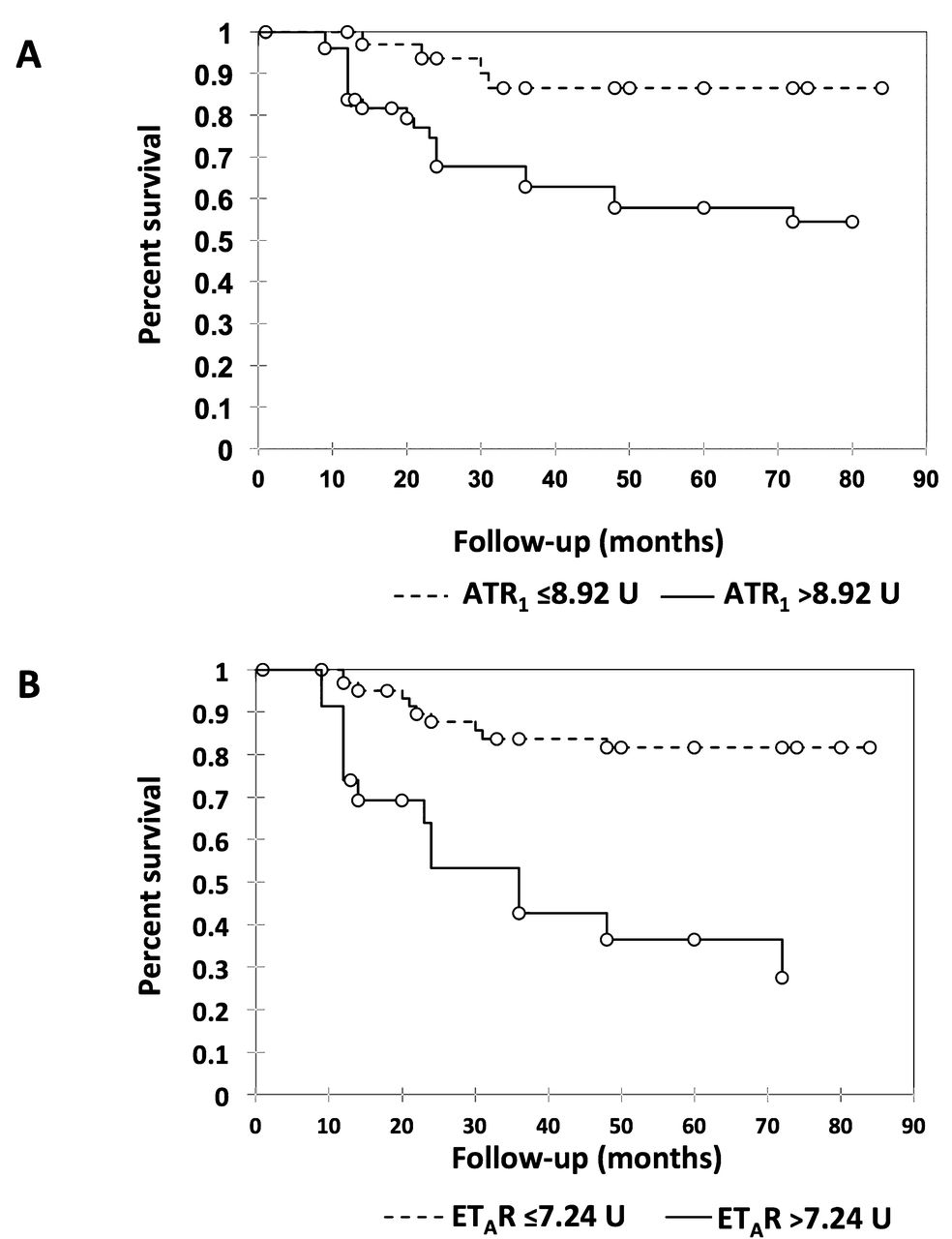
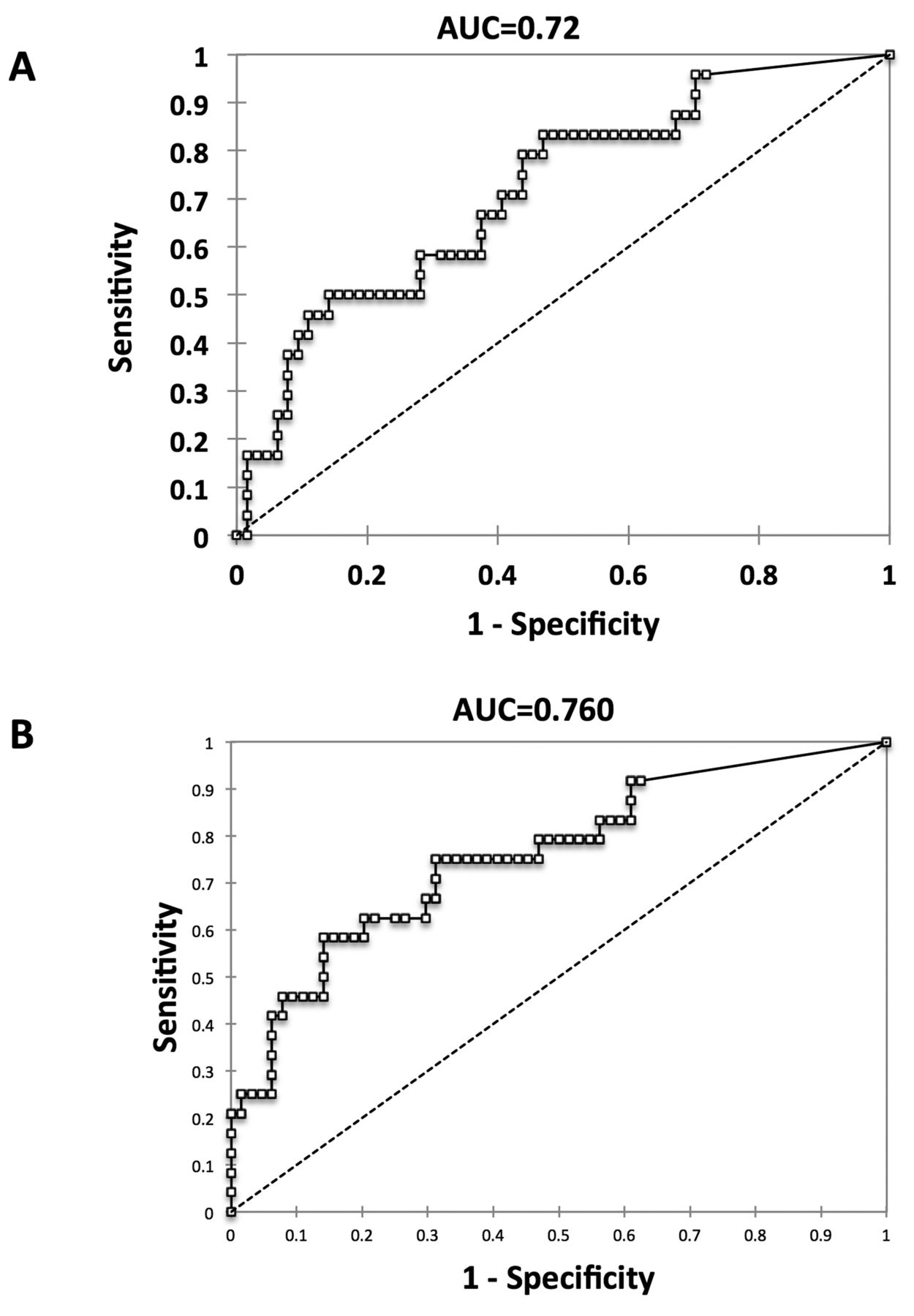
Univariate Cox analysis revealed that concentrations above the median value of anti-AT1R and anti-ETAR antibodies were predictive of the occurrence of ischemic DU (HR 2.85, 95% CI 1.19–6.84, p = 0.02 and 3.39, 95% CI 1.35–8.50, p = 0.009, respectively). Kaplan-Meier analyses of freedom from the occurrence of new DU for these 2 autoantibodies confirmed the results observed with Cox analyses and are shown in Figure 2A–B. In addition, the diagnostic value of anti-AT1R and anti-ETAR antibodies for detecting patients with ischemic DU was reflected by an area under the curve of 0.72 and 0.76, respectively (Figure 3A–B).
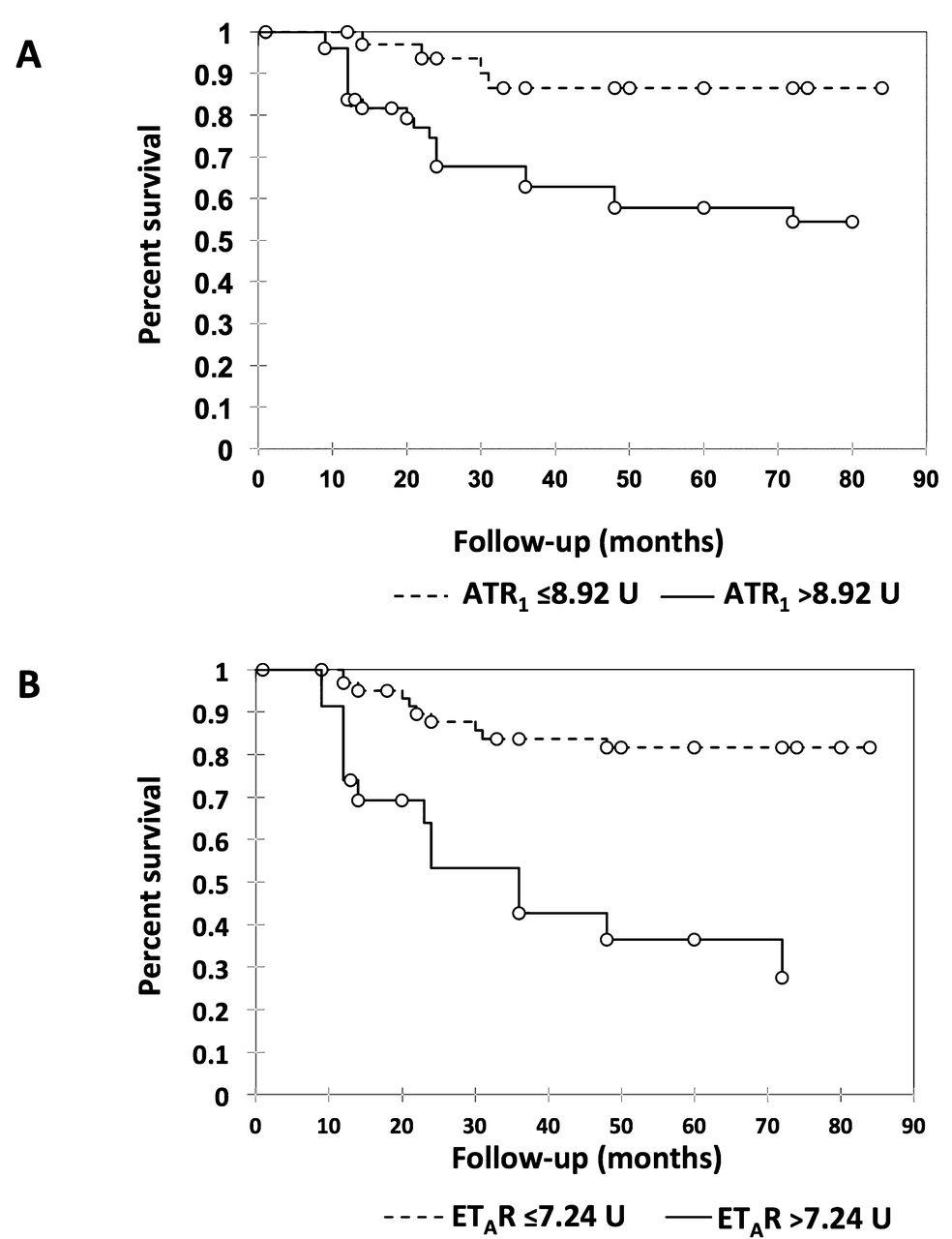
Kaplan-Meier analyses of freedom from ischemic digital ulcers in 90 patients with SSc. Curves are shown for patients with SSc who had (A) anti-AT1R antibodies ≤ 8.92 and > 8.92 units at study entry (p = 0.003) or in those who had (B) anti-ETAR antibodies ≤ 7.24 or > 7.24 units at study entry (p < 0.001). SSc: systemic sclerosis; anti-AT1R: antiangiotensin II Type 1 receptor; anti-ETAR: antiendothelin 1 Type A receptor.

Receiver-operating characteristic curve for the (A) anti-AT1R and (B) anti-ETAR autoantibody prediction of ischemic DU. AUC were 0.72 and 0.76 for anti-AT1R and anti-ETAR autoantibodies, respectively. Anti-AT1R: antiangiotensin II Type 1 receptor; anti-ETAR: antiendothelin 1 Type A receptor; DU: digital ulcers; AUC: area under the curve.
In patients who developed ischemic DU during the followup period, no correlation was observed between the speed of DU development and the serum levels of AT1R (r −0.13, p = 0.537) or anti-ETAR (r −0.06, p = 0.791) antibodies.
Multivariate analysis
Because anti-AT1R and anti-ETAR autoantibodies were correlated, and because Cramer V resulted in a coefficient of association between these 2 variables of 0.71 (suggesting a strong association), each functional antibody was entered as an independent covariate in 2 different multivariate models.
A first multivariate Cox analysis included functional autoantibodies and clinical predictors of new DU identified in univariate analysis by a p value < 0.2 (Supplementary Table 2 available from the authors on request). This analysis confirmed only anti-ETAR autoantibodies as independent predictors of the occurrence of new ischemic DU (HR 3.15, 95% CI 1.22–8.13, p = 0.02) together with the presence at baseline of active DU or history of DU (Table 2).
Evaluation of functional autoantibodies against vascular receptors as predictors of ischemic DU. Results of univariate and multivariate analyses.
A second multivariate analysis implemented with angiogenic markers identified as univariate predictors of new DU was then performed (Table 3; Supplementary Table 3 available from the authors on request) and confirmed anti-ETAR autoantibodies as an independent predictor of the development of new DU (HR 9.59, 95% CI 1.75–52.64, p = 0.010) together with the presence at baseline of active DU or history of DU (Table 3).
Results of univariate and multivariate analyses of candidate predictors of ischemic DU by model analyzed.
DISCUSSION
Our prospective study demonstrates that anti-ETAR autoantibodies are independently predictive of the occurrence of new DU together with the presence at baseline of active DU or history of DU, a well-known clinical predictor of this complication. This finding is important because the identification of relevant predictive biomarkers may allow the detection of a subset of patients who might be candidates for specific management including potential preventive therapeutic strategies.
Although DU are a frequent complication in patients with SSc, few data are available regarding the incidence of new ischemic DU4. In our study, the incidence of new DU (0.04 cases for 100 person-yrs) is close to the incidence recently reported in the EUSTAR database (0.05 cases for 100 person-yrs)18.
We have previously shown the merit of high PlGF serum levels and low circulating EPC counts to predict new DU4. The originality of our current study was to confront in multivariate analysis functional antibodies together with clinical variables and selective validated angiogenic markers. Of the most interest, anti-ETAR autoantibodies were found to outperform the different angiogenic markers, which emphasizes their strong ability to predict the occurrence of new DU. Moreover, anti-ETAR antibodies had a higher predictive value for the occurrence of new DU than did anti-AT1R antibodies in all the analyses performed. Thus, using ET blockers in this context sounds attractive, especially as the ET blocker bosentan is available to prevent recurrent DU, although the patients with the highest benefit and precise management remain to be established.
In addition, to be important for the prediction of DU, anti-AT1R and anti-ETAR antibodies may be important for the pathogenesis of DU, and more broadly of SSc. Indeed, these autoantibodies are biologically active and induce proinflammatory and fibrotic events in endothelial cells and healthy donor fibroblasts through angiotensin and endothelin receptor activation11,12. In addition, blocking AT1R and ETAR seems to alleviate some vascular manifestations of SSc beyond inducing vasodilation5,11,19,20. Thus, a therapeutic perspective might be the clearance of these functional autoantibodies, and B cell therapies by example could be an option in the future.
There are several strengths to our study, including its prospective design, the strong power of the study sample, the longterm followup, the exclusion of nonischemic DU, and the quality of data collected in a center with high experience of the care of patients with SSc.
However, the limitations of our study should also be considered when interpreting the findings. The influence of endothelin receptor antagonists and ACE inhibitors on anti-AT1R and anti-ETAR levels has not been assessed in our study, and should be further studied. Anti-AT1R and anti-ETAR autoantibodies have been previously found associated with other cardiovascular complications of the disease, including pulmonary arterial hypertension (PAH) and scleroderma renal crisis. Unfortunately, the number of patients who developed these complications was too low in our study sample to firmly allow the identification of predictors. Of note, a recent study has demonstrated that anti-AT1R and anti-ETAR autoantibodies are predictive and prognostic markers of SSc-PAH21. Finally, the number of patients with critical digital ischemia at baseline was insufficient to study its predictive value, and nailfold videocapillaroscopy was not systematically performed at baseline, preventing the evaluation of capillary rarefaction as a potential predictor of new ischemic DU.
Our results show that functional autoantibodies against vascular receptors, and particularly anti-ETAR autoantibodies, can be used together with the presence of current or past DU to identify patients with SSc who are at risk for the development of DU during a median 60-month followup period. This may have important clinical implications in that noninvasive tests may be used to identify high-risk patients who should undergo more careful evaluation and management. Further studies assessing the use of these markers in therapeutic strategies aimed at selection of patients for early treatment or prevention therapy are warranted.
- Accepted for publication June 22, 2015.








{kind=link}
{kind=link}
{kind=link}