

Abstract
Objective. To investigate the relationship between antiestrogen therapy in women with breast cancer and risk of autoimmune disease.
Methods. We used a national database to assess the incidence of systemic lupus erythematosus (SLE) and rheumatoid arthritis (RA) following treatment with selective estrogen receptor modulators (SERM) or aromatase inhibitors (AI) in women with breast cancer. The total number of patients in our study was 190,620.
Results. We observed highly significant, cumulative dose-dependent increased OR of incidence of both SLE and RA following treatment with SERM (p < 0.0001). The odds of developing RA were also increased following AI therapy (p < 0.001), but there was a trend for reduced odds of SLE, though this trend did not attain statistical significance (p = 0.070 for 2–11 months of treatment and p = 0.254 for 12+ months of treatment).
Conclusion. Antiestrogen agents may have an important effect on risk of autoimmune disease.
- AUTOIMMUNE DISEASES
- SELECTIVE ESTROGEN RECEPTOR MODULATORS
- AROMATASE INHIBITORS
- ESTROGEN RECEPTOR-POSITIVE
- SYSTEMIC LUPUS ERYTHEMATOSUS
- RHEUMATOID ARTHRITIS
Systemic lupus erythematosus (SLE) and rheumatoid arthritis (RA) can lead to severe morbidity and increased mortality, as well as drastically altered quality of life1,2. Women are 7 to 9 times more likely than men to develop SLE, while the female:male sex ratio is 2–3:1 for RA3. Estrogen may play a key role in these sex differences by influencing the immune response4, and numerous reports have established the importance of estrogen in induction of autoantibodies and promotion of disease activity in SLE3.
Estrogen is produced from androgenic precursors through the enzymatic activity of aromatase and exerts its myriad effects by binding to receptors present on many tissues throughout the body. Both variations in estrogen receptor (ER) type5,6 and aromatase activity7,8 have been implicated in the mechanism of autoimmune disease. Thus, these elements have become the object of studies aimed at decreasing the expression and severity of autoimmune disorders. Drugs that target these factors, including selective ER modulators (SERM) such as tamoxifen, and aromatase inhibitors (AI) such as anastrazole, have long been available for treatment of ER–positive patients with breast cancer9. The purpose of our study was to investigate any relationship between the use of these therapies and the incidence of RA and SLE.
Current data on the use of AI and SERM in patients with autoimmune disorders are equivocal or lacking in humans. A few studies exist on the effects of SERM on RA10 or SLE11, but they show no conclusive results. The effect of AI on these disorders has not been studied, to our knowledge. Further, the potential relationship between AI and SERM use and subsequent incidence of autoimmune disorders has not been studied.
Our study explores the relationship between the use of SERM and AI and the subsequent diagnosis of SLE and RA using a retrospective cohort study of a large, de-identified patient database (Explore; Explorys Inc.)12.
MATERIALS AND METHODS
De-identified patient data were collected from a database containing records from patients seen in multiple healthcare systems across the United States from 1999 to 2013 (Explore; Explorys Inc.). The database standardizes patient data by mapping diagnoses into the Systematized Nomenclature for Medicine – Clinical Terms (SNOMED-CT). Drug prescriptions were categorized by class with SNOMED or by individual drug with RxNorm12. This database permits searching by demographics, diagnosis, and medicines prescribed, and months of treatment. Explorys searches result in output in terms of numbers of patients but do not yield average baseline statistics for cohorts such as age.
The overall patient cohort was composed of all women over the age of 18 years who did not have a diagnosis of SLE or RA at the time of the breast cancer diagnosis. Among these patients, our control cohort comprised those who did not receive any SERM or AI treatment, and our experimental cohorts comprised those receiving 2–11 or 12+ months of either SERM or AI. The OR of developing SLE or RA was set equal to 1.0 in the control group (patients without SERM or AI treatment). We chose to exclude patients who received only a single month of these agents (n = 3250 for the AI cohort and n = 2780 for the SERM cohort) to eliminate spurious results caused by isolated use. We also excluded the small number of patients who received both SERM and AI (n = 5340) because we found too few patients who went on to develop RA or SLE in this category to warrant appropriate statistical analysis. We chose to analyze the data at 12 months to review the effects of using the drug for a full year. Further categorization beyond this number (e.g., 18 or 24 mos) was precluded in this study owing to a lack of sufficient data.
The incidence of autoimmune disorders was defined as the number of patients who received a diagnosis of SLE or RA at any time after cancer diagnosis for the control cohort and after initiating drug treatment for the experimental cohorts. For comparison, SLE and RA prevalence rates were calculated for the general female population over the age of 18, as well as the entire population of patients with breast cancer, regardless of drug treatment. For this study, the SERM chosen were tamoxifen, raloxifene, and toremifene; the AI were anastrazole, exemestane, formestane, letrozole, and aminoglutethimide.
OR and logistic regression calculations were used to determine incidence rates and CI. Chi-squared analyses with a null hypothesis of p1 = p2 were performed to determine the statistical difference in disease incidence with various doses of AI or SERM therapy when compared to no treatment. These analyses were performed with R 3.0.2.
Our study was approved by the Institutional Review Board of the MetroHealth Medical Center, Cleveland, Ohio, USA (approval number IRB13-00305).
RESULTS
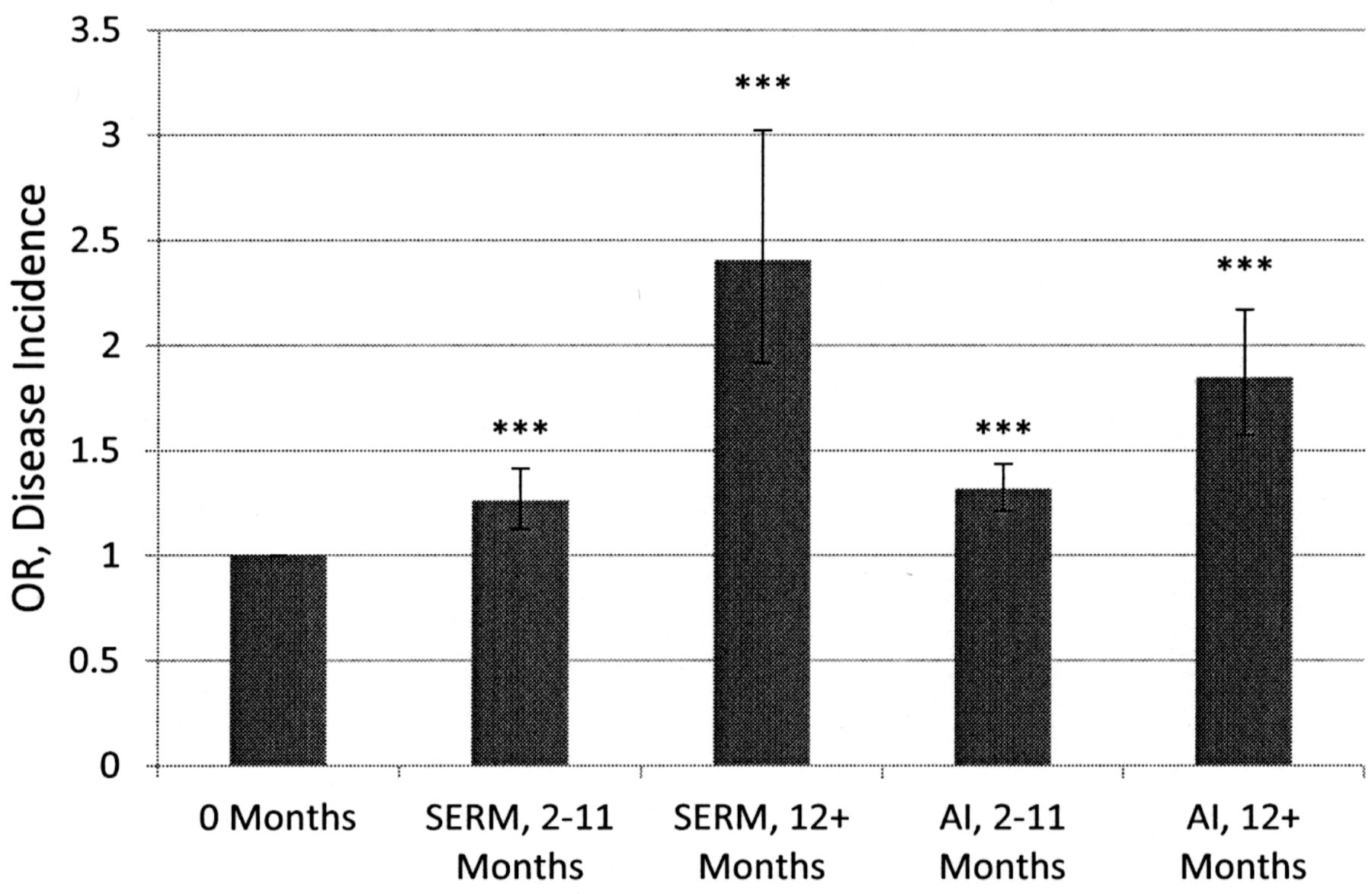
Over 12 million patients fit our initial search criteria, with 238,880 diagnoses of breast cancer of any type. We studied the OR of incidence of SLE and RA in patients diagnosed with breast cancer who received antiestrogen agents, compared with our control cohort of 190,620 patients with breast cancer who did not receive antiestrogen therapy. Our results are shown in Table 1. Patients receiving any SERM had a cumulative dose-dependent increased OR of developing both RA [1.26 for 2–11 months (95% CI 1.13–1.41; p = 3.61 × 10−5); 2.41 for 12+ months (95% CI 1.92–3.02; p = 3.95 × 10−16)] and SLE [1.41 for 2–11 months (95% CI 1.16–1.71; p = 4.76 × 10−4); 2.02 for 12+ months (95% CI 1.29–3.15; p = 1.41 × 10−3)]. This relationship was also observed for the use of AI and the risk of developing RA [1.32 for 2–11 months (95% CI 1.21–1.44; p = 4.14 × 10−11); 1.85 for 12+ months (95% CI 1.57–2.17; p = 4.23 × 10−15)]. When taking into account Bonferroni’s correction for multiple comparisons, the p value for significance (with 4 group comparisons) between any 2 groups is p = 0.0125. The calculated p values show that even after this correction, the data are still highly statistically significant.
Antiestrogen use and incidence of RA and SLE in patients with breast cancer.
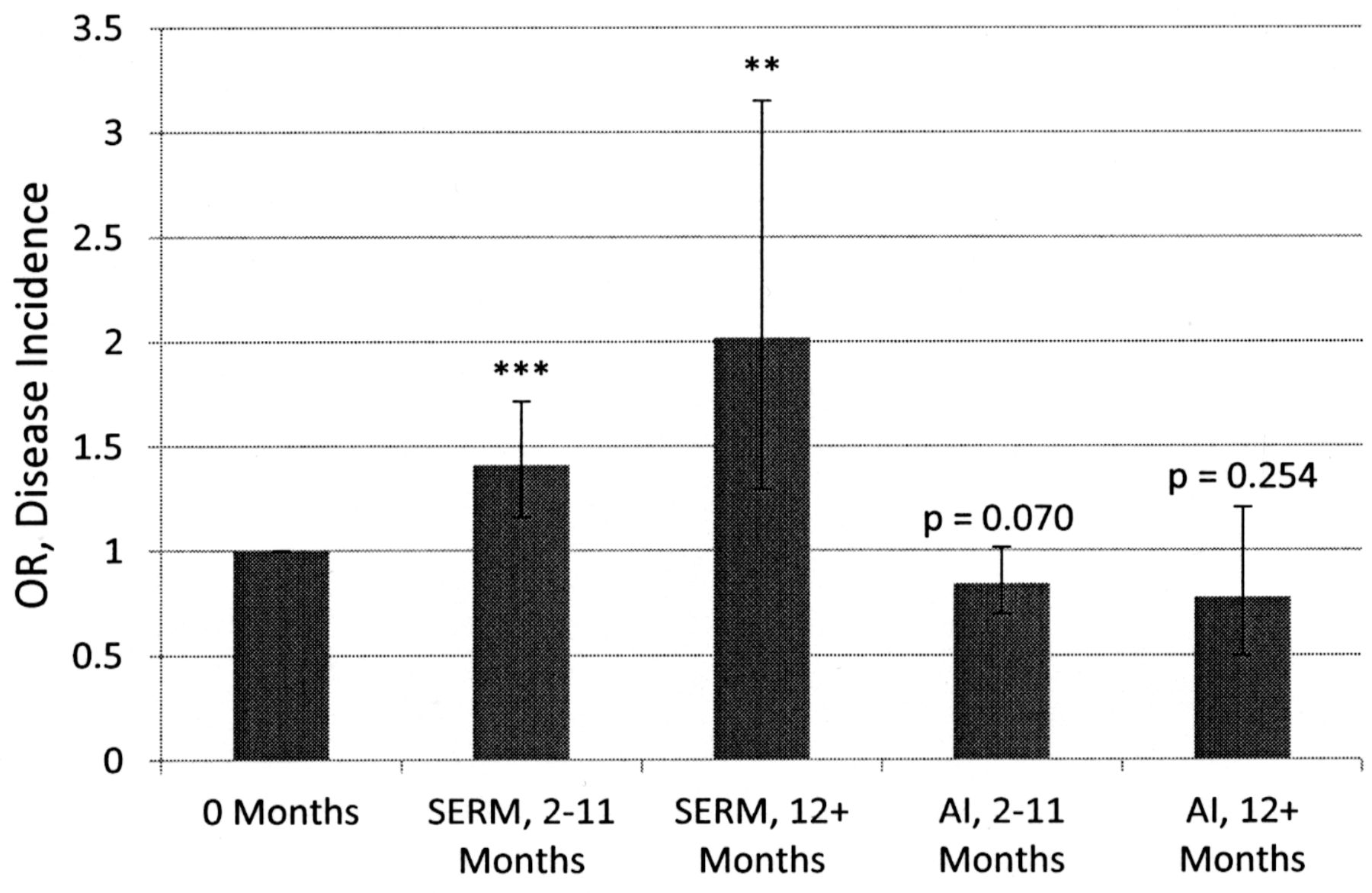
In contrast, patients receiving any AI had a decreased OR of developing SLE (0.84 for 2–11 months; 0.77 for 12+ months); however, these results were not statistically significant (95% CI 0.70–1.02; p = 0.070; and 95% CI 0.50–1.21; p = 0.254, respectively).
Because of the recent availability of the database used for this study, we intended to validate our approach. We used the database to assess the prevalence of SLE and RA in the general population (all females over the age of 18) as well as in all patients with breast cancer, regardless of treatment received (Table 2). The prevalence rates we observed for the general female population were consistent with those reported in large epidemiological studies1,2. Further, the database estimate of breast cancer prevalence in females, 2.0%, roughly corresponds with the value derived from literature, 1.8%13.
SLE and RA prevalence in women 18+ years and all patients with breast cancer.
DISCUSSION
We found a cumulative, dose-dependent, positive correlation between the use of SERM and subsequent diagnoses of RA and SLE, as shown in Figures 1 and 2. Given the statistical significance of this association and the temporal precedence of treatment prior to disease diagnosis of RA or SLE, our findings suggest a possible causative influence of these drugs on the incidence of these autoimmune diseases. It is possible that some type of selection bias related to more extensive diagnostic testing in women with breast cancer (including possibly rheumatoid factor and antinuclear antibody tests) than in “healthy women” could influence the diagnosis of these autoimmune disorders. Such a possibility might partly explain the slightly increased prevalence of SLE and RA among all patients with breast cancer, compared with healthy women (Table 2). However, we would not expect such a situation to apply between patients with breast cancer who did and those who did not receive antiestrogen therapy (our control cohort). With regard to use of AI, we also observed a statistically significant cumulative dose-dependent increased OR of RA (Figure 1). This finding should be considered speculative, in view of the knowledge that up to 50% of patients treated with AI experience polyarthralgias14, a tendency that could conceivably contribute to an increased diagnosis of RA. In contrast, we found a cumulative dose-dependent, inverse correlation between the use of AI and SLE incidence OR, as shown in Figure 2; however, these results did not achieve statistical significance.

Relationship between months of treatment with SERM and AI and OR of RA incidence. Statistically significant at *** p < 0.001. SERM: selective estrogen receptor modulator; AI: aromatase inhibitor; RA: rheumatoid arthritis.
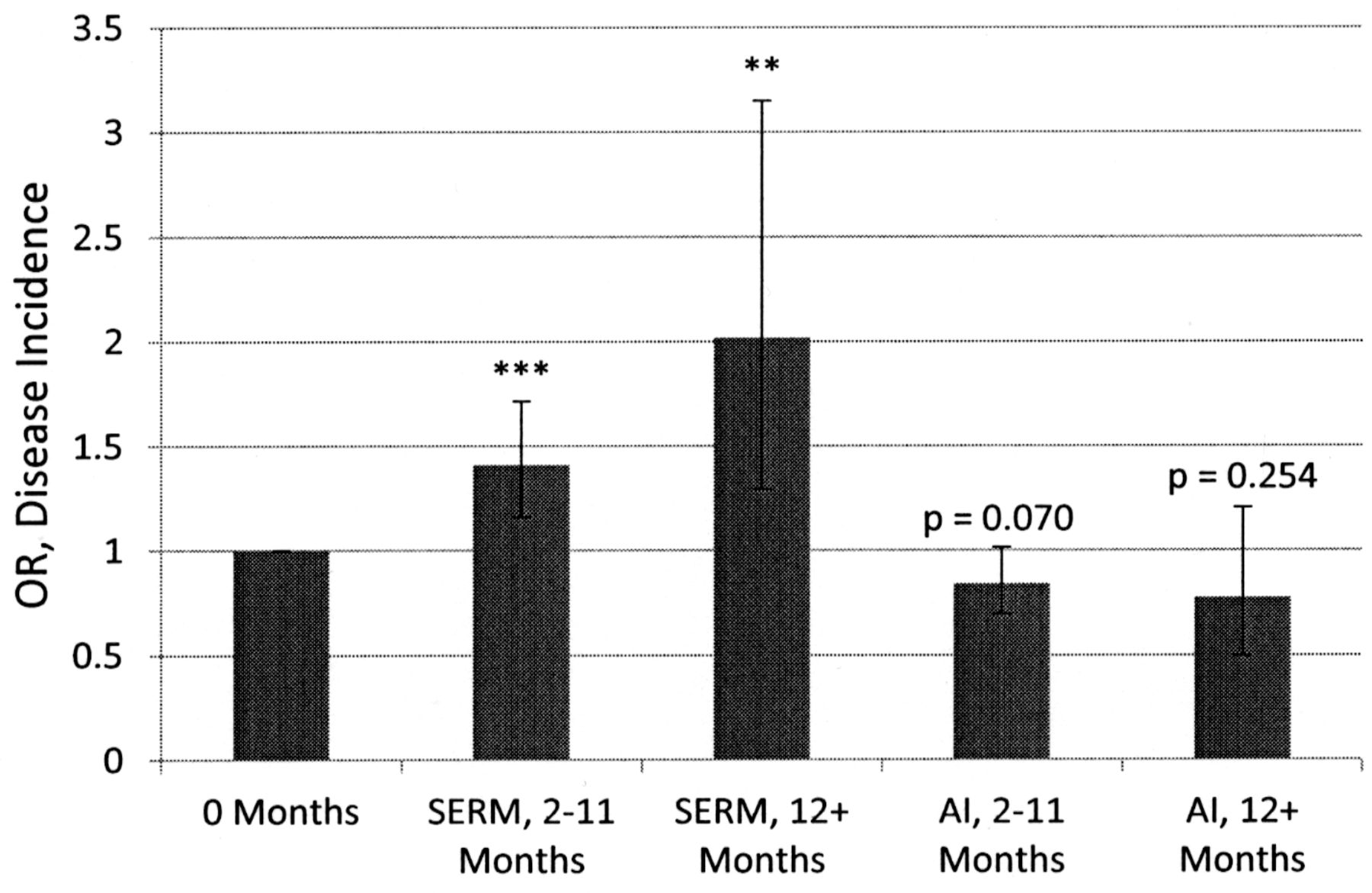
Relationship between months of treatment with SERM and AI and OR of SLE incidence. Statistically significant at ** p < 0.01, *** p < 0.001. SERM: selective estrogen receptor modulator; AI: aromatase inhibitor; SLE: systemic lupus erythematosus.
Our results are interesting given the mechanism of estrogen in promoting autoimmune disease. Estrogen has numerous effects on the immune system, including inhibition of apoptosis of mononuclear cells, stimulation of autoreactive B cells and autoantibody production, enhancement of inflammatory cytokine production [e.g., interleukin 1 (IL-1), IL-4, IL-10, and transforming growth factor-β], suppression of IL-2 production, and promotion of calcineurin-induced T cell activation4. In aggregate, these effects can contribute to an autoimmune diathesis. The major estrogen in humans, 17-β-estradiol, binds to one of 2 receptors (α and β) that are both expressed on numerous immune cells, including T lymphocytes and B lymphocytes and dendritic cells4. Experimental studies using mouse models of SLE have suggested that ER-α activity is most important in promotion of clinical autoimmune disease7. Though SERM are typically thought of as estrogen antagonists, their effects on ER-α and ER-β are variable. For example, SERM as a class have an antagonist effect on cell growth in ER+ breast cancer cells, while tamoxifen in particular is associated with the growth of endometrial cancer cells15. Further, both tamoxifen and raloxifene are agonists at the ER-α16, thus providing a possible explanation for the increased incidence of SLE and RA in patients receiving those therapies.
Because AI inhibit the direct enzymatic conversion of androgens such as testosterone and dehydroepiandrosterone to estrogenic compounds, it might be assumed that they would have a more straightforward effect on autoimmune disorders. The well-established importance of estrogen in the disease process of SLE is consistent with our data, showing a cumulative dose-dependent trend of decreased incidence in patients receiving AI. This trend was not found to be statistically significant, perhaps related to the small numbers of patients even in this very large population. In RA, however, our findings should be viewed with caution. The statistically significant increased disease incidence that we observed may be clouded because a common side effect of AI use is polyarthralgia, which may confound a precise diagnosis of RA. Finally, the discrepancy between risk of SLE and RA in patients taking AI provides further support for the likely greater role of estrogen in the pathogenesis of SLE.
One limitation of our study is that a large, anonymous cross-sectional database cannot retrieve certain data relative to individual patients. Characteristics that may affect the incidence of autoimmune diseases, such as menopausal status, change over time and are thus not well recorded. Thus, we are unable to provide baseline information or regression models comparing the control and treatment groups. Further, we are unable to determine an appropriate denominator for our incidence results (e.g., patient-yrs). Thus, the incidence rates we report are relative to our control and treatment groups within this study and cannot be compared to those in the literature. The OR findings, however, between patients with breast cancer treated and untreated with antiestrogen are valid and are the main focus of our study. An additional concern is whether use of chemotherapy agents in antiestrogen untreated patients could have influenced the risk of SLE or RA. We were unable to obtain consistent data relative to such agents in view of the multitude of agents (often used in variable combinations), differing doses, and variable time periods of administration. However, we know of no data suggesting that chemotherapeutic regimens used for treatment of cancer reduce the subsequent occurrence of autoimmune diseases.
Further studies are needed to more clearly elucidate the influence of antiestrogen agents on autoimmune disorders. A better understanding of the mechanistic action of SERM in various tissues would help clarify their roles in these diseases. The effect of individual drugs on the different ER should also be firmly established. Future work may be conducted on individual patients to investigate any possible relationship between use of these drugs and markers of disease activity and progression in both SLE and RA. An analysis of individual patients might allow better insight into the role of chemotherapy and age, if any, in influencing the development of autoimmune disorders as well. Finally, the relationship between antiestrogen agents and other autoimmune disorders, such as autoimmune thyroiditis or Sjögren syndrome, should be addressed.
Our study provides evidence that the use of selective ER modulating agents may increase the risk of developing autoimmune disorders such as SLE and RA. AI have a more speculative but intriguing influence on the risk of these disorders. These risks are of importance to clinicians who use antiestrogen agents for treatment of breast cancer or osteoporosis, as is the possibility that these agents could influence disease activity in these autoimmune disorders.
Acknowledgment
We thank Dr. David Kaelber and Todd Sarbach for providing access and instruction in using the Explorys database for this study. We also thank Dr. Doug Einstadter and Joseph Lee for their assistance with statistical analysis. We also thank Emma Barnboym for assisting in submitting the Institutional Review Board approval application.
- Accepted for publication August 26, 2014.








{kind=link}
{kind=link}