

Abstract
Objective. Primary gout has been associated with single-nucleotide polymorphisms (SNP) in several tubular urate transporter genes. No study has assessed the association of reabsorption and secretion urate transporter gene SNP with gout in a single cohort of documented primary patients with gout carefully subclassified as normoexcretors or underexcretors.
Methods. Three reabsorption SNP (SLC22A12/URAT1, SLC2A9/GLUT9, and SLC22A11/OAT4) and 2 secretion transporter SNP (SLC17A1/NPT1 and ABCG2/BRCP) were studied in 104 patients with primary gout and in 300 control subjects. The patients were subclassified into normoexcretors and underexcretors according to their serum and 24-h urinary uric acid levels under strict conditions of dietary control.
Results. Compared with control subjects, patients with gout showed different allele distributions of the 5 SNP analyzed. However, the diagnosis of underexcretor was only positively associated with the presence of the T allele of URAT1 rs11231825, the G allele of GLUT9 rs16890979, and the A allele of ABCG2 rs2231142. The association of the A allele of ABCG2 rs2231142 in normoexcretors was 10 times higher than in underexcretors. The C allele of NPT1 rs1165196 was only significantly associated with gout in patients with normal uric acid excretion.
Conclusion. Gout with uric acid underexcretion is associated with transporter gene SNP related mainly to tubular reabsorption, whereas uric acid normoexcretion is associated only with tubular secretion SNP. This finding supports the concept of distinctive mechanisms to account for hyperuricemia in patients with gout with reduced or normal uric acid excretion.
Increased serum urate levels in gout may be the result of enhanced purine synthesis, decreased uric acid excretion, or both1. In most patients with primary gout, hyperuricemia has been related to a reduced renal uric acid excretion (underexcretors)2,3. In contrast, increased uric acid synthesis is suspected in normoexcretors with gout in whom the renal handling of uric acid is presumed to be normal.
The renal handling of uric acid is a complex process involving glomerular filtration and both tubular reabsorption and secretion, all of which determine a normal net uric acid excretion of almost 10% of the filtered load of urate2. In the last decade, several tubular urate transporters have been described that influence either urate reabsorption or secretion4.
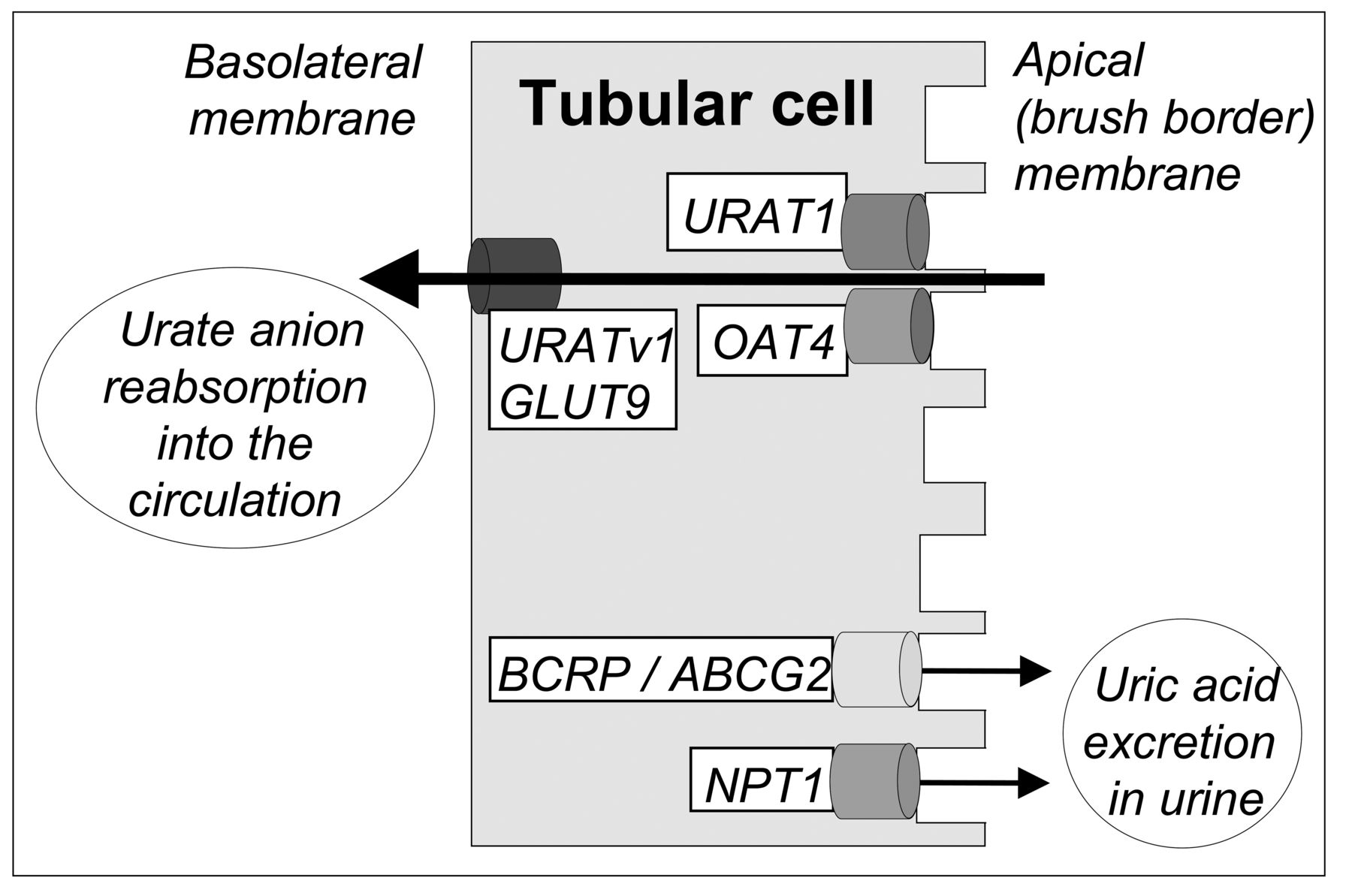
Several studies, including a number of genome-wide association studies, have identified a substantial association between single-nucleotide polymorphisms (SNP) in as many as 28 genetic loci, including 6 urate-transporter-coding genes (URAT1/SLC22A12, GLUT9/SLC2A9, ABCG2/BCRP, SLC22A11/OAT4, SLC17A1/NPT1, and SLC17A3/NPT4), and serum urate concentrations5,6,7,8,9,10,11,12. The essential role of URAT1 and GLUT9 transporters in proximal tubular urate reabsorption has been underscored by their marked functional deficiency in patients with renal hypouricemia (OMIM 220150 and 612076, respectively) attributable to renal urate wasting13,14,15. Data have been published relative to gout association with URAT1, GLUT9, ABCG2, OAT4, and SLC17A1/NPT1 SNP; however, a number of studies have shown certain discrepancies. For instance, among several SNP at 8 genetic loci with a significant association with serum urate levels, Yang, et al9 reported that only 2 loci (GLUT9 and ABCG2) were significantly associated with gout. Several studies11,16 suggested that NPT1 polymorphisms are associated with gout; however, Stark, et al5 did not find such an association. It is remarkable that in a number of these studies, the diagnosis of gout was self-reported5,6,17, and no study, to our knowledge, has yet assessed the association of several SNP in a single cohort of well-characterized patients with gout classified into normoexcretors and underexcretors. In our study, we analyzed 5 previously gout-related SNP, corresponding to 5 different reabsorption and secretion tubular urate transporter-related genes (Figure 1) in normal subjects and in patients with primary gout, diagnosed according to the American College of Rheumatology criteria, and classified into normoexcretors and underexcretors following a protocol that included renal uric acid excretion rates and serum urate concentrations determined under strict dietary control.
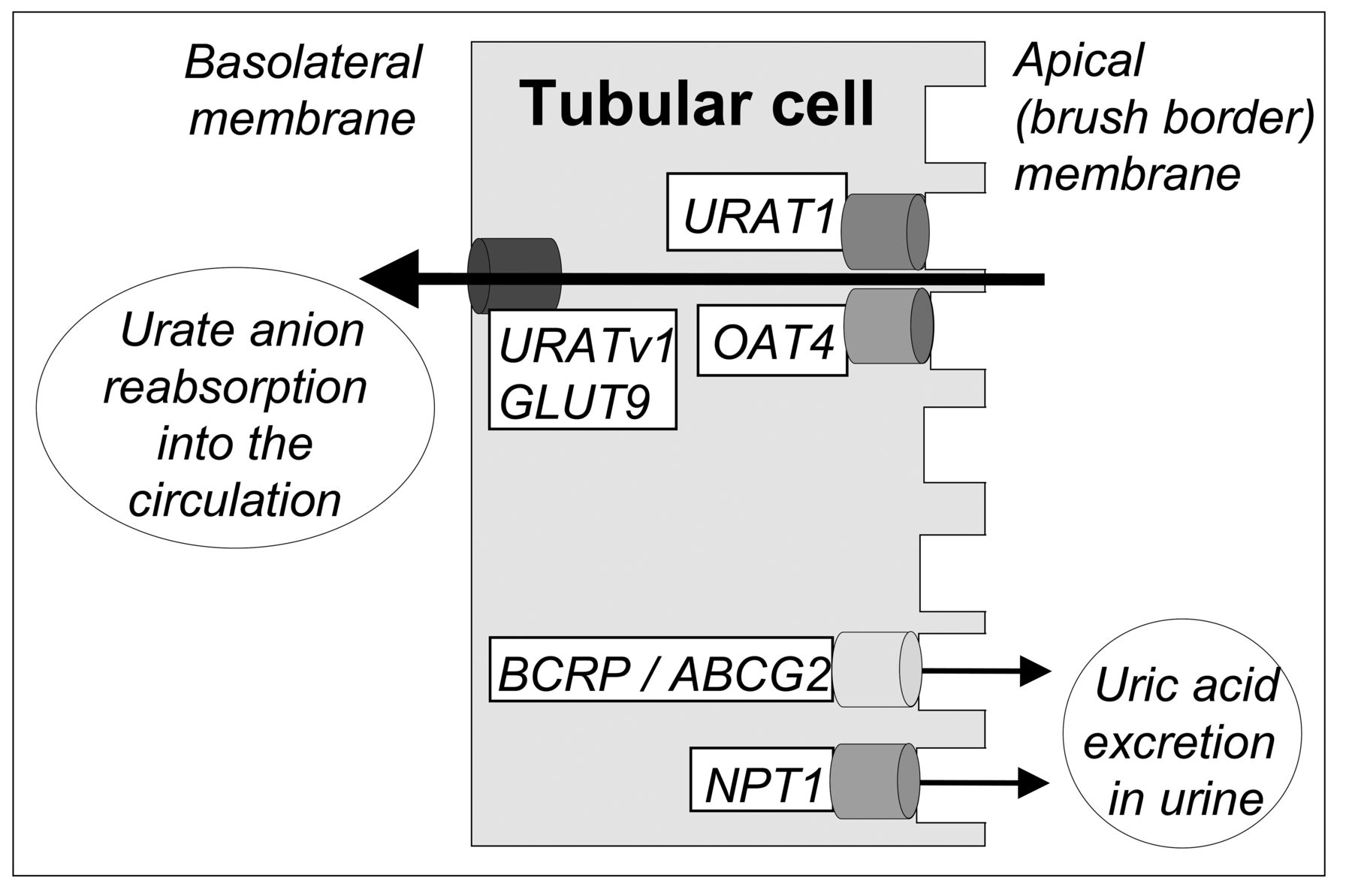
Schematic diagram showing the 5 tubular urate transporter genes studied in the current model of bidirectional urate anion movement in proximal tubule epithelial cells. Urate reabsorption at the apical membrane is critically regulated by SLC22A12/URAT1, which exchanges urate for intracellular organic anions (e.g., lactate, nicotinate) and monocarboxylates (e.g., pyrazinamide metabolites). The organic acid transporter SLC22A11/OAT4 also contributes to urate reabsorption from the tubular lumen. The hexose transport facilitator SLC2A9/GLUT9 (URATv1) performs voltage-dependent urate anion reabsorption into the circulation at the basolateral membrane. The purine nucleoside transporter BCRP/ABCG2 and the voltage-driven transporter SLC17A1/NPT1 mediate urate secretion at the apical membrane.
MATERIALS AND METHODS
Patients
Patients with primary gout were recruited from the outpatient clinic of the Metabolic-Vascular Unit, Division of Internal Medicine at La Paz University Hospital, Madrid. Primary gout was diagnosed according to the American College of Rheumatology criteria18. Only patients with 2 or more acute arthritis episodes documented by a physician were selected for our study (n = 141). Secondary gout attributable to enzymopathies was discarded by determination of phosphoribosyl pyrophosphate synthetase and hypoxanthine-guanine phosphoribosyltransferase activities in erythrocyte lysates by high-performance liquid chromatography, as previously described19,20. The main exclusion criteria were secondary gout (i.e., psoriasis, n = 4), marked organ insufficiency that precluded participation on an ambulatory basis (n = 10), and unwillingness to participate (n = 9). All studies were conducted according to the Declaration of Helsinki and were approved by the institutional research and ethics review committees of La Paz University Hospital. Medications that might affect uric acid metabolism were discontinued for a 3-month period prior to the start of our study. Colchicine (0.5 to 1.0 mg/day) was prescribed as a prophylaxis against acute gouty arthritis. All patients signed informed consent forms.
A specialized nurse provided all subjects with detailed instructions on following a weight-maintenance, isocaloric, purine-restricted diet (< 75 mg/24 h of purines, with a protein content of 10%–15%) for 5 days before the 24-h urine sample collection. At the end of the 24-h urine collection and following an overnight fast and rest, venous blood was obtained between 7 AM and 10 AM for uric acid and creatinine determination and DNA extraction. Patients with serum urate levels < 6.5 mg/dl following the 5-day purine-restricted diet were excluded from our study (n = 6). Subjects who did not collect urine appropriately were scheduled for a second visit the following day and instructed to continue the same purine-free diet. None of the subjects had lost ≥ 1 kg by the end of the purine-free diet period. Patients with a 24-h creatinine clearance < 45 ml/min/1.73 m2 were excluded from our study (n = 8). According to a constructed nomogram21, patients with gout were classified into 2 groups: normoexcretors and underexcretors. This nomogram takes into account the individual body surface area and serum urate concentration, the main variable determining urinary uric acid excretion.
Comorbidities were assessed following the definition proposed by the European Society of Hypertension22. The control group included DNA and plasma from 300 healthy subjects from the Spanish National DNA Bank. The Spanish National DNA Bank receives, processes, and stores DNA, plasma, and cell samples from donors along with relevant information on health and lifestyle habits related to the samples.
Methods
Uric acid and creatinine levels were determined by means of the uricase enzymatic and Jaffé methods, respectively. The RNA-free genomic DNA samples from 101 patients with gout were isolated from whole blood using a DNA Purification Kit (Puragene, Gentra systems). DNA samples from 300 control subjects were isolated with the same DNA Purification Kit.
Five SNP (rs11231825, rs16890979, rs17300741, rs1165196, and rs2231142) corresponding to 5 different tubular urate transporter-related genes (URAT1, GLUT9, OAT4, NPT1, and ABCG2, respectively), were analyzed in all subjects. These 5 SNP have previously been associated with serum uric acid levels6,7 and primary gout5,6–8,9,10,11,12,23. Four SNP are in the coding region and 1 SNP is intronic (rs17300741; Table 1). SNP rs16890979, rs1165196, and rs2231142 are nonsynonymous and cause the V253I, T269I, and Q141L amino acid change, respectively, in their corresponding proteins (GLUT9, NPT1, and ABCG2).
Primer sequences (5′–3′) and probes used for amplification of SNP regions in 5 human genes that encode tubular urate transporters.
Genotyping was performed on each 50-ng genomic DNA sample using the LightCycler 480 System (Roche), with the LightCycler 480 Genotyping Master. For each SNP, a set of primers and HybProbe probes was designed and obtained from TIB MOLBIOMOL (Table 1). The specificity of the amplified PCR product was assessed by performing a melting curve analysis to discriminate between the homozygote for the major frequency allele, the homozygote for the minor frequency allele, and the heterozygote products.
Statistical analysis
The analysis plan for our study specified a minor allele frequency of 25%24, a significance level of 5% (α), and a 3:1 ratio (control/case) to provide about 95% power to detect a difference of ± 20%. Thus, a sample size of 400 subjects (300 controls and 100 cases) was estimated (Query Advisor program, version 5.0). Mean values with SD and percentages were used to describe the patient characteristics. The differences between groups were evaluated with t tests for continuous variables and a logistic-regression model for dichotomous variables.
The Hardy-Weinberg equilibrium25 for genotypic frequencies for the 5 study SNP in the control subjects was calculated using the chi-squared test. The association of the 5 different SNP genotypes and serum urate levels was performed by 1-way ANOVA with a posthoc Bonferroni test. We used a Bonferroni correction of p < 0.00625, equivalent to p < 0.05 significance, to correct for multiple testing, assuming independent tests for the 5 SNP.
OR and 95% CI were calculated to assess the relationship between SNP and the diagnosis of primary gout and gout subgroups (normoexcretors and underexcretors). A multivariate logistic regression analysis was used to compare allele distribution of the 5 SNP in the different subject groups.
A genetic risk score was generated for every individual by counting the number of alleles of those genes that were associated with serum urate levels in our population (rs11231825 T of URAT1, rs16890979 G of GLUT9, and rs2231142 A of ABCG2; range 0 to 6 points) in control subjects and patients with primary gout6,9,26. The correlation between the risk score and serum urate concentrations was performed using a logistic regression model by means of the chi-squared test. A risk score comparison between controls and patients with gout was conducted using the Mann-Whitney U test.
All p values are 2-sided, and p values of < 0.05 were considered to indicate statistical significance (Statview SAS version 9.2).
RESULTS
Participant characteristics
A total of 104 patients with primary gout completed our study. According to the uric acid nomogram21, 16 patients were classified as normoexcretors (15.4%) and 88 as underexcretors (84.6%; Table 2). The mean daily uric acid excretion was 344 mg/day/1.73 m2 (95% CI, 310–378 mg/day/1.73 m2) higher in normoexcretors with gout than in underexcretors, despite a mean serum urate level 1.0 mg/dl lower in the former than in the latter (Table 2). The fractional excretion of uric acid (Cur/Ccr × 100) in normoexcretors was a mean of 46% higher than in underexcretors (p < 0.001). Clinical characteristics were not significantly different between the 2 groups with gout except for age and renal function. Patients with uric acid underexcretion were on average 6.4 years older than normoexcretors, although the duration of the disease evolution was similar for the 2 groups (slightly above 12 yrs). The glomerular filtration rate was on average 10 ml/min/1.73 m2 lower in underexcretors than in normoexcretors (Table 2), with 20 patients in the former group showing a 24-h creatinine clearance below 60 ml/min/1.73 m2 (range 45–59 ml/min/1.73 m2). Mean serum urate levels and 24-h urinary uric acid excretion were not significantly different in patients with creatinine clearance levels below or above 60 ml/min/1.73 m2 (8.5 mg/dl and 402 mg/day/1.73 m2 vs 8.0 mg/dl and 542 mg/day/1.73 m2, respectively).
Clinical characteristics of patients with primary gout stratified into normal (normoexcretors) and diminished (underexcretors) urinary uric acid excretion related to their serum urate level. Data are mean ± SD unless otherwise indicated.
SNP distribution in control subjects and patients with gout
All of the genotypic frequencies for the 5 study SNP complied with the Hardy-Weinberg equilibrium (p > 0.05) in control subjects25. A strong association was found in all study subjects between the presence of allele T of rs11231825 (URAT1), allele G of rs16890979 (GLUT9), and allele A of rs2231142 (ABCG2) and serum urate concentrations (Table 3). In contrast, no significant association was found between the presences of allele A of rs17300741 (OAT4) and allele C of rs1165196 (NPT1) and serum urate levels.
Associations of serum urate concentrations (mean ± SD) with SNP in the study population [healthy controls (n = 300) and patients with primary gout (n = 101)]. The number of study participants is provided in parentheses. p = Bonferroni test. Numbers in bold face are significant data.
The allele distributions of all the SNP analyzed were significantly different when comparing the controls with all patients with gout as a group (Table 4). Two reabsorption transporter genetic loci, URAT1 rs11231825 and GLUT9 rs16890979, were positively associated with underexcretors with gout (OR 1.62, 95% CI 1.00–2.63, p = 0.04 and OR 3.78, 95% CI 1.09–13.12, p = 0.005, respectively). However, no reabsorption transporter genetic loci were associated with normoexcretors with gout. One secretion transporter SNP (rs2231142 of ABCG2) showed a positive association with gout both in underexcretors (OR 2.91, 95% CI 1.40–6.08, p = 0.005) and in normoexcretors (OR 28.95, 95% CI 5.96–140.6, p = 0.0002), although the OR for normoexcretors was 10 times higher. The other studied secretion transporter SNP, rs1165196 NPT1, showed a negative association only in normoexcretors (OR 0.16, 95% CI 0.05–0.49, p = 0.003).
Allele distribution of the analyzed SNP in the different groups (control, gout, UE and NE patients with gout). Table expresses percentage of the examined allele in heterozygosis and homozygosis; parentheses indicate values in each different group; n = no. subjects with the examined allele in heterozygosis or homozygosis versus the total number of subjects in the group (n/total). OR and 95% CI were calculated to assess the relationship between SNP and the diagnosis of primary gout and gout subgroups (UE and NE). A multivariate logistic regression analysis was used to compare the allele distributions of the risk allele of each SNP in the different subject groups. Numbers in bold face are significant data.
Genetic risk score
An individual genetic risk score was generated by counting the number of alleles of those genes associated with serum urate levels in our population (rs11231825 allele T, rs16890979 allele G, and rs2231142 allele A; range 0 to 6 points according to the number of risk alleles). The proportion of subjects across the genetic risk score showed a markedly different distribution, with control subjects and patients with gout skewed to the lower and upper risk scores, respectively (Figure 2A). Mean serum urate concentrations in the entire population increased linearly with the number of risk alleles (chi-square = 20.035, p = 0.0027; Figure 2B). In addition, the prevalence of gout also increased linearly with the number of risk alleles (Figure 2C). The OR for the diagnosis of primary gout, adjusted for age and sex, increased significantly for those patients with ≥ 3 risk alleles (Figure 2D). For subjects with no risk alleles, the crude prevalence of gout was 0.257 and increased to 52.478 for those with 6 risk alleles (208-fold increase).

Association of a genetic risk score, constructed with the number of hyperuricemia risk alleles, and the prevalence of gout and serum urate concentrations. (A) Proportion of control subjects and patients with primary gout across the genetic risk score. (B) Mean serum urate (mg/dl) levels and their 95% CI for each genetic risk score. (C) Crude prevalence of gout for each genetic risk score. (D) OR of gout for each genetic risk score.
DISCUSSION
Our study shows that patients with primary gout have a significantly increased prevalence of certain alleles for some SNP related to tubular urate transporter genes, which might help explain their uric acid metabolic disorder. Moreover, tubular urate transporter SNP differentiate patients with gout with normal and decreased urinary uric acid excretion. The association found between 3 SNP with serum urate concentrations allowed us to construct an individual hyperuricemia-genetic risk score. We have shown that this additive genetic score had a strong and graded association with primary gout.
To the best of our knowledge, SNP analyses of genes that encode tubular urate transporters have not been reported in patients with gout classified according to their uric acid excretion rate related to their serum uric acid levels. In our study, according to the uric acid nomogram, only 15.4% of patients with gout were classified as normoexcretors. The mean daily uric acid excretion was remarkably higher in normoexcretors with gout than in underexcretors, despite a mean serum urate level 1.0 mg/dl lower in the former than in the latter (Table 2).
Patients with gout showed different allele distributions of the 5 SNP analyzed than did control subjects. However, the diagnosis of underexcretor was only positively associated with the presence of the T allele of URAT1 rs11231825, the G allele of GLUT9 rs16890979, and the A allele of ABCG2 rs2231142, whereas no reabsorption transporter genetic loci were associated with normoexcretors with gout.
The SNP on secretion transporter ABCG2 showed a positive association with gout both in underexcretors and in normoexcretors, although the OR for normoexcretors was 10 times higher. Given that ABCG2 mediates tubular urate secretion23, it is likely that the dysfunction of this molecule most probably reduces uric acid excretion (Figure 1). The finding of dysfunctional variants of the urate secretion transporter ABCG2 among underexcretors with gout and the increased prevalence of the 2 tubular urate reabsorption transporter SNP studied herein may help explain the long-lasting uric acid underexcretion reported in most patients with primary gout2,3. However, what explains the dysfunction in the urate secretion transporter ABCG2 in patients with normal uric acid excretion rates? Dysfunctional variants of ABCG2 have been reported as major causes of gout and hyperuricemia23,27. Recently, in a study of 644 men with hyperuricemia, the rate of uric acid excretion was found to be inversely related to the ABCG2 function28. ABCG2 is expressed not only in the kidneys29, but also in the apical membrane of several tissues, including the liver and intestines30. In those organs, ABCG2 may contribute to urate secretion31, provided that one-third of urate excretion in humans depends on gut excretion31,32,33. It is conceivable that the dysfunction of ABCG2 affects all organs in which it is expressed. The finding of an increased uric acid excretion rate in ABCG2-knockout mice34 led to the proposition that ABCG2 dysfunction may, by decreasing extrarenal urate excretion (“extrarenal urate underexcretion”), increase the body urate pool, which would enhance urinary uric acid excretion34. This proposal has led to a new classification known as “overproduction” or “renal overload” hyperuricemia34, which may explain the mechanism of urate overproduction in a substantial proportion of patients with gout (15% in our study) who have no evidence of increased uric acid synthesis attributable to an enzyme defect.
The decreased prevalence of allele C of rs1165196 (NPT1) among patients with gout suggests that this allele is a protective, rather than a risk, allele that modulates the secretory expression of NPT1, reducing the likelihood of hyperuricemia and gout. The result of a significantly decreased prevalence of allele C of rs1165196 (NPT1) among normoexcretors with gout, but not among underexcretors with gout, may be interpreted in light of the apparent paradoxical result of ABCG2. SNP rs1165196 is a nonsynonymous polymorphism that causes a threonine 269 to isoleucine amino acid change in NPT1 protein. The NPT1 I269 protein (T allele) has been shown to transport about one-third less than the T269 NPT1 protein (C allele). At least 1 SLC17 member has been found to localize in the intestinal brush border membrane35; thus, it is possible to speculate that similar to ABCG2, NPT1 dysfunction may decrease extrarenal urate excretion. This fact could facilitate a new classification of patients with gout into 2 groups: renal urate underexcretors and extrarenal urate underexcretors (formerly normoexcretors).
The finding of a significant correlation between the genetic risk score and both serum urate concentrations and the prevalence of gout can best be interpreted as an indication that certain SNP markedly determine the kidneys’ handling of urate. This suggests that knowledge of patients’ genotypes could help identify individuals at risk of gout, such as those with metabolic syndrome or cardiovascular diseases36, long before the onset of clinical features, and may help guide clinical decisions, particularly when considering drugs known to increase serum urate levels37. One limitation of our study is that the results are related to 5 genes, among 9 urate transporter genes described to date32. However, to our knowledge, this is the largest study in which 5 urate transporter gene SNP were studied in a well-characterized cohort with gout according to their uric acid excretion rate. The reduced number of normoexcretors with gout (n = 16, 15%) is in agreement with the proportion of those patients reported in most series2,3,4,38. Despite the reduced numbers, we found significant results that were markedly different from those of underexcretors with gout. A study with a similar number of participants from 3 ancestral groups recently concluded that genetic variations in GLUT9 influence uric acid metabolism in European white subjects, but not in Maori and Pacific ethnic groups39. Another limitation of our study is that we assigned the same value in the genetic risk score to each allele. However, this methodology has been previously reported in other studies on gout6,26, and when the association between cholesterol polymorphisms and cardiovascular event risk has been examined40.
Our study shows that patients with primary gout, and normal or decreased uric acid excretion rates, have different prevalence rates for certain SNP related to tubular urate transporters. These results may contribute to a better understanding of the mechanism of hyperuricemia in primary gout.
Acknowledgments
We thank the physicians who participated in the Grupo MAPA-Madrid for referring their patients to the Metabolic Unit. We are indebted to Carolina Velasco García, the research manager of the Metabolic Vascular Unit, and its nursing staff (Inés Narillos and Arantxa Sánchez) for their excellent patient care and followup; to Rosario Madero, PhD, for the statistical analysis; and to Almudena Ligos Díaz for her assistance in preparing the manuscript.
Footnotes
-
Published online before print August 15, 2014
-
Supported by grants from the Fondo de Investigación Sanitaria del Instituto de Salud Carlos III (Healthcare Research Fund of the Carlos III Health Institute; FIS, 08/0009 and 11/0598).
- Accepted for publication May 21, 2014.








{kind=link}
{kind=link}