

Abstract
Objective. Our study reports the results of the MIRA (MabThera In Rheumatoid Arthritis) registry, set up to collect data about clinical usage, patient profile, and retention of rituximab (RTX) treatment in daily clinical practice in Belgium.
Methods. Patients with active rheumatoid arthritis (RA) who failed at least 1 anti-tumor necrosis factor (anti-TNF) treatment were included in our study between November 2006 and October 2011. At baseline, demographics, medication, disease history, disease activity, rheumatoid factor (RF), and anticyclic citrullinated peptide antibodies (anti-CCP) status were recorded. Evolution of the 28-joint Disease Activity Score (DAS28)-erythrocyte sedimentation rate, retreatments, and reasons for therapy stop were followed prospectively.
Results. The MIRA registry included 649 patients, with mean disease duration of 12.8 ± 0.4 years and DAS28 values at inclusion of 5.85 ± 0.48. Patients received on average 2.82 ± 0.07 (range 1–9) RTX treatments, over a mean followup period of 93.1 ± 2.6 weeks. At database lock, 433 patients (66.7%) were still under RTX treatment, 182 (28.0%) had stopped treatment, and 34 (5.2%) were lost to followup. Ineffectiveness (n = 108, 59%) and safety concerns (n = 39, 22%) were the most frequent reasons for discontinuing RTX therapy. From 2006 to 2011, RTX practice patterns clearly evolved toward RTX being started in patients with a lower number of previously failed anti-TNF drugs and lower baseline DAS28 values. A lower number of previous anti-TNF drugs, and positivity for RF and anti-CCP, predicted more successful longterm treatment. RTX treatment provided adequate longterm disease control.
Conclusion. In our daily practice study, RTX provided good longterm disease control and treatment retention in refractory patients with RA. Over the years, rheumatologists tended to start this treatment in patients with fewer previous anti-TNF treatments and lower disease activity.
Rituximab (RTX) is a genetically engineered monoclonal anti-CD20 antibody, indicated for treating rheumatoid arthritis (RA) after prior failure of antitumor necrosis factor (anti-TNF) drugs. It has been shown to be safe, effective, and prevent progression of radiological lesions in this indication1,2,3,4.
RTX effectively suppresses disease activity over a relatively long period, but because response decreases over time, retreatment is often necessary. Five-year followup data from the Randomized Evaluation of Long-Term Efficacy of Rituximab in RA (REFLEX) study show that RTX retains its effectiveness over multiple treatment courses5.
The MIRA (MabThera In Rheumatoid Arthritis) registry was set up to collect data about clinical usage, treatment retention, and reasons for stopping treatment in daily clinical practice. Setup and interim results were reported previously6. Our study reports longterm RTX treatment practice, and analyzes predictors of successful longterm treatment.
MATERIALS AND METHODS
Study population
All patients in Belgium and Luxembourg starting RTX treatment between November 2006 and October 2011 were eligible for inclusion in the Belgian MIRA registry. In Belgium, RTX treatment is available and reimbursed for patients receiving methotrexate with baseline 28-joint count Disease Activity Score (DAS28) > 3.7 after failure of at least 1 anti-TNF.
At least 6 months after the previous treatment, patients are eligible for retreatment if the first treatment elicited moderate to good response at Week 16 and their current DAS28 is ≥ 3.2. No specific exclusion criteria were defined.
Our study was approved by the ethical committees of all participating centers. All patients provided written informed consent prior to inclusion in our study.
Study design and data collection
The design and data collection of the MIRA registry study were described previously6. Briefly, baseline data included demographics, medication and disease history, rheumatoid factor (RF), and anticyclic citrullinated peptide antibodies (anti-CCP) status. RTX treatment was administered as two 1000-mg infusions given 2 weeks apart, with administration of 1 g of paracetamol, 100 mg of methylprednisolone, and an antihistaminic prior to RTX infusion. European League Against Rheumatism (EULAR) response was evaluated at Week 16, and followup data (treatment status, patient global visual analog scale, DAS28) were collected every 8–12 weeks and before retreatment, for as long as patients continued RTX treatment. Data were collected until October 2012.
When RTX treatment was stopped, the date and reason for discontinuation were recorded. Patients were considered lost to followup if no data were collected for at least 1 year.
Data analysis and statistics
Data are presented as mean ± standard error or percentages. Statistical tests used were t test or ANOVA for normally distributed variables, Mann-Whitney U test for variables not distributed normally, chi-square for categorical variables, and Kaplan-Meier analysis for treatment survival (SPSS 20, IBM Corporation). A p < 0.05 was considered statistically significant.
RESULTS
Population characteristics
The MIRA registry enrolled 649 patients with RA treated by 80 rheumatologists in 52 centers. At inclusion, patients were 57.4 ± 0.5 years old, with disease duration of 12.8 ± 0.4 years, and DAS28 values of 5.85 ± 0.48. Medication history included 1 previous biologic in 54.2%, 2 biologics in 32.4%, and more than 2 biologics in 12.5% of patients. Before starting RTX, 29.2% of patients used prednisolone and 28.1% methylprednisolone.
Evolution of baseline characteristics over time
Over the 5-year inclusion period, the number of failed anti-TNF drugs used before starting RTX treatment decreased significantly (chi-square, p < 0.001; Table 1). In parallel, the DAS28 values of patients starting RTX treatment also decreased significantly over time (ANOVA, p < 0.001).
Evolution of the baseline characteristics of patients starting rituximab (RTX) treatment over time. Over the period 2006–2011, patients starting RTX treatment evolved toward lower DAS28 values (p < 0.001, ANOVA) and fewer previously failed anti-TNF treatments (p < 0.001, chi-square).
Therapy retention and reasons for discontinuation
At database lock, 433 patients (66.7%) were still under RTX treatment, 182 patients (28.0%) had stopped, and 34 patients (5.2%) were lost to followup. Mean overall followup time was 93.1 ± 2.6 weeks (range 8–252) and mean RTX treatment time was 168.7 ± 4.5 weeks (Figure 1). At Week 16, 78.2% of patients had at least moderate EULAR response. Patients with MIRA received on average 2.82 ± 0.07 (range 1–9) RTX courses with a mean interval of 262.0 ± 3.8 days. Ineffectiveness (n = 108, 59.3%) and safety concerns (n = 39, 21.4%) were the most frequent reasons for discontinuation. Thirteen patients (7.1%, 2.0% of total) died during followup. Causes of death were pneumonia (n = 2); metastatic bronchus carcinoma, myeloma, and suicide (n = 1 each); and unknown (n = 8).
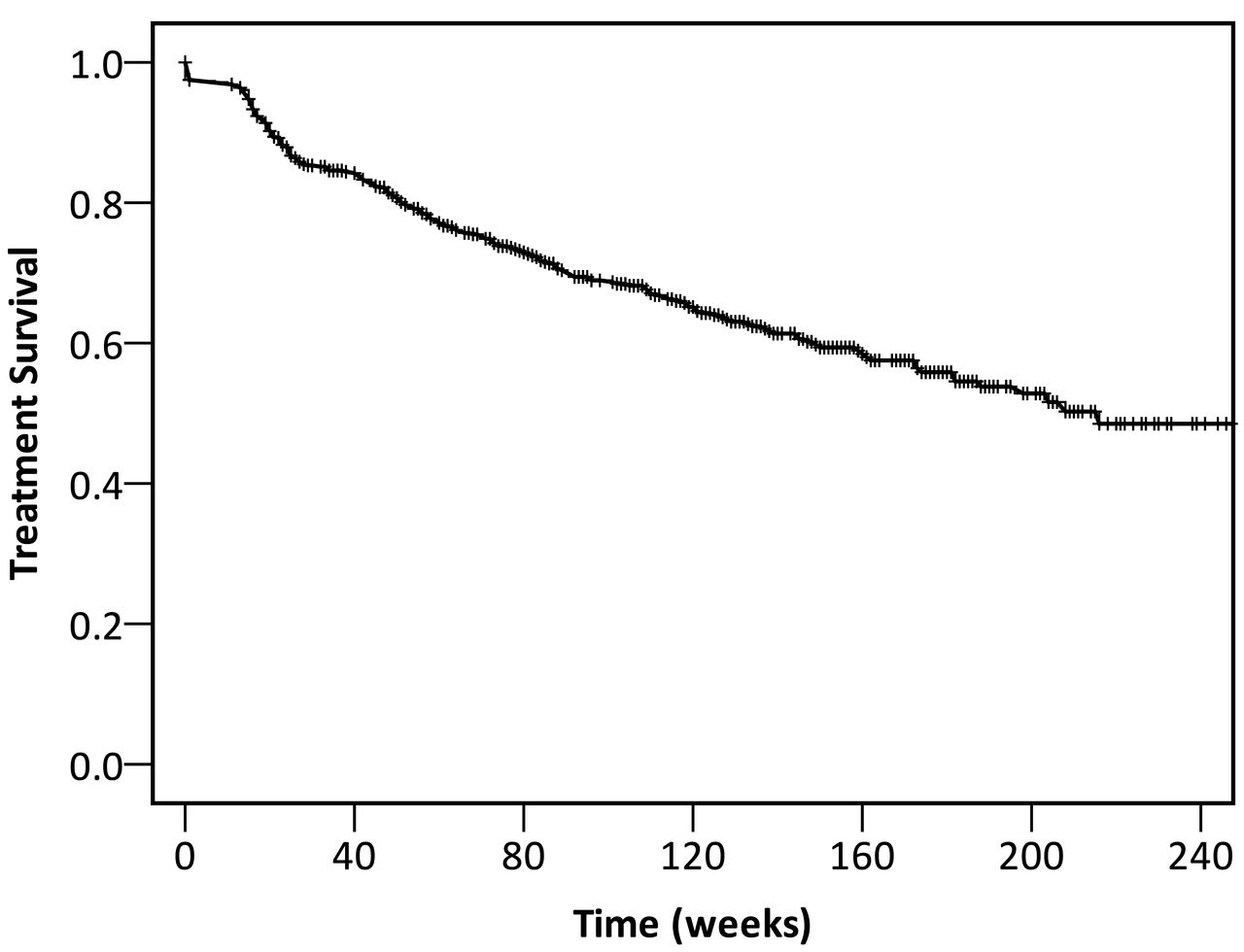
Kaplan-Meier curve for rituximab treatment survival. In the overall MIRA population, maximum followup duration was 254 weeks and mean treatment time was 168.7 ± 4.5 weeks. Vertical tick marks on the survival curve represent patients censored at the end of followup. The followup period was variable because patients were included between November 2006 and October 2011, and the study ended in October 2012. MIRA: MabThera In Rheumatoid Arthritis.
Safety concerns included infusion reaction (n = 13, 2.0%); infection (n = 6, 0.9%); malignancy (n = 5, 0.8%); cytopenia and adenopathy (n = 2 each); abnormal liver enzymes, hallucinations, hypertension, atrial fibrillation, fatigue, and unexplained pain (n = 1 each). In 5 patients, the safety reason was not further specified.
Additional reasons for discontinuation were personal decision of the patient (13/16), diarrhea, pregnancy wish, and participation in a clinical trial (n = 1).
The reasons for RTX discontinuation significantly shifted with age: while ineffectiveness was the most frequent reason for discontinuation in younger patients and decreased with age, safety concerns occurred more frequently in older patients.
Longterm disease control with RTX treatment
Patients with longer drug retention had a significantly lower number of previous anti-TNF, and higher prevalence of RF and anti-CCP positivity in comparison with patients who stopped (Table 2). Age, sex, disease duration, and baseline DAS28 did not differ significantly between patients who continued and discontinued RTX.
Factors predicting longterm treatment success with rituximab (RTX). Patients who continued RTX treatment were previously treated with a significantly lower number of anti-TNF agents in comparison with those who discontinued RTX during the study. Additionally, prevalence of RF and anti-CCP positivity was significantly higher in the group that continued treatment. DAS28, age, sex, and disease duration did not differ significantly between the groups who continued and discontinued RTX treatment.
DAS28 values (Figure 2) declined sharply over the first year of RTX treatment and stabilized afterward.
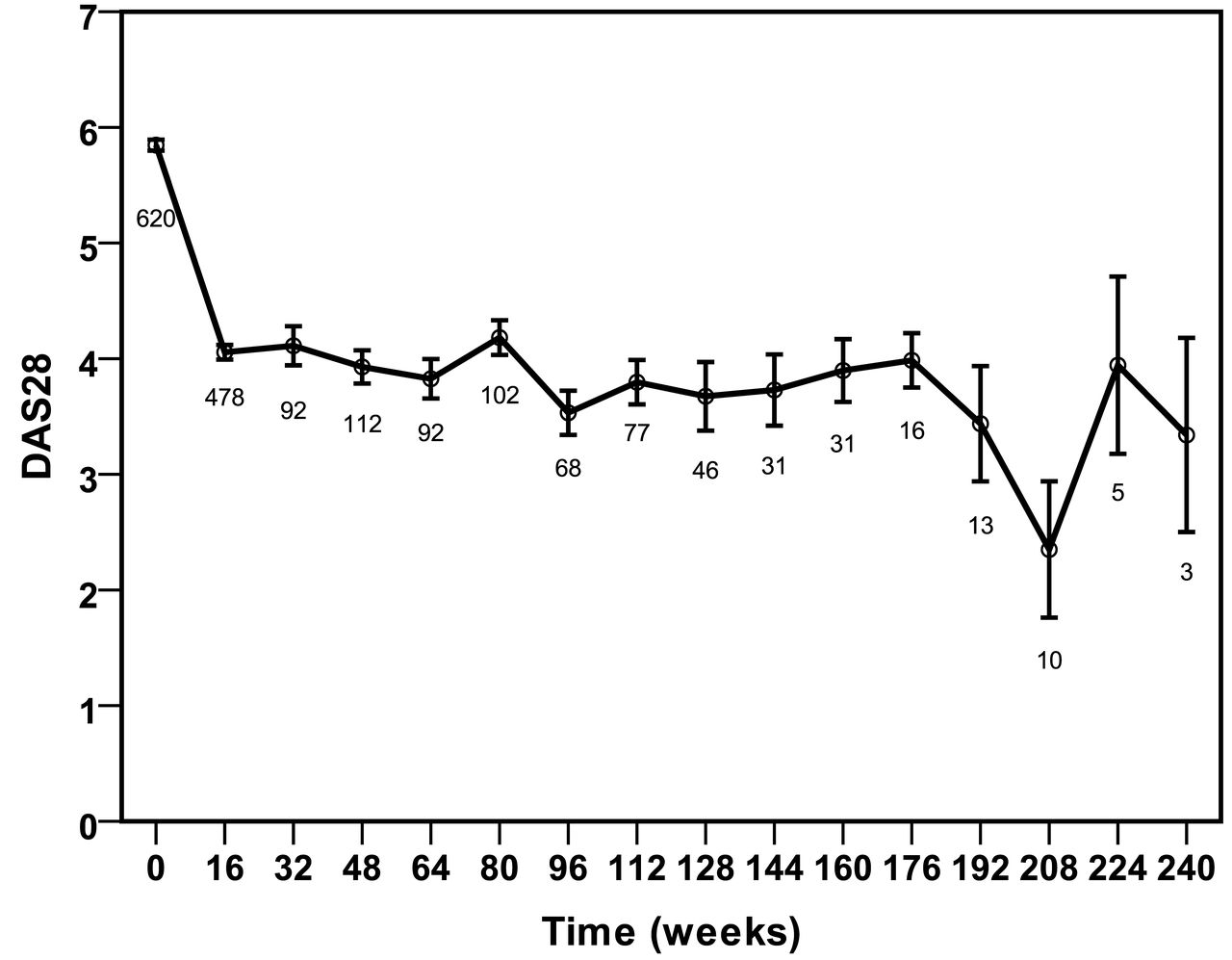
DAS28 values over time. Data are presented as mean ± SE; numbers below the graph represent the number of DAS28 measurements per timepoint, which was lower than the number of patients followed at that timepoint, especially for patients with longer followup duration. DAS28: 28-joint Disease Activity Score.
DISCUSSION
The MIRA registry prospectively collected data on a population of 649 patients with longstanding active RA treated with RTX after failure of at least 1 anti-TNF agent.
In this daily clinical practice setting, RTX retention was relatively high: treatment was discontinued in 28.0% of patients after a mean followup of 93.1 ± 2.6 weeks. Ineffectiveness was the most frequently reported reason for discontinuation, followed by safety concerns. Although age did not predict treatment success in our study, the relative number of treatment discontinuations for safety reasons tended to be higher for older patients.
Longterm disease control under RTX, analyzed in a subpopulation of patients treated for at least 3 years, was good, with DAS28 declining sharply over the first year and remaining stable for the remainder of our study.
Over the 5-year inclusion period (2006–2011) of the MIRA study, RTX treatment was increasingly started in patients with less active disease, and as a second biological, after only 1 failed anti-TNF drug. RTX can be considered a good choice for patients who have failed a first or single anti-TNF treatment7,8,9,10,11.
In correspondence with other reports12,13,14,15,16, long-term treatment success in the MIRA population was associated with RF and anti-CCP positivity, whereas age, sex, disease duration, and baseline DAS28 values were not predictive for longer drug retention.
Acknowledgment
We thank the Royal Belgian Society for Rheumatology (KBVR/SRBR) and an unrestricted grant from Roche (Basel, Switzerland). The authors acknowledge the contribution of Veerle Persy, MD, PhD (Hugin Mugin Research) as an independent medical writer.
APPENDIX
List of MIRA Study Group collaborators: De Meulenaere, Leon (Ambroise Paré, Mons); De Keyser, Van den Bosch (AZ Alma, Sijsele); Maertens (AZ Damiaan Campus H. Hart, Oostende), Vandevyvere (AZ Groeningen, Kortrijk); Raeman (AZ Jan Palfijn, Merksem); Ghyselen (AZ Lokeren, Lokeren); Castro, Stappaerts (AZ Middelares, Ghent); Reychler (AZ Oudenaarde, Oudenaarde); Lensen (AZ Seruys, Oostende); De Brabanter, Maeyaert (AZ Sint Lucas, Brugge); Ackerman, Luyten (AZ Sint Lucas, Ghent); De Clercq, Hoffman, Schatteman (AZ St Augustinus, Wilrijk); D’hondt, Peene (AZ St Jan, Brugge); Maenaut (AZ St Jozef, Malle); Daumerie, Docquier (CH Jolimont Lobby, Haine St Paul); Halleux (CH Ste Elisabeth, Heusy); Fontaine (CHC Liege, Liege); Cremer (CHC, Waremme); Mathy (CHD, Dinant); Martin (CHR St Joseph Warquignies, Boussu); Daens, Fernandez Lopez (CHU Brugmann, Brussels), Jeukens, Nizet (CHU Liege, Chenee); Kaiser, Lust, Ribbens (CHU Sart Tilman, Liege); Di Romana (CHU St Pierre, Brussels); Schreiber (CHU Tivoli, La Louviere); Dall’Armelina, Jardinet (Clinique Notre-Dame de Grâce ASBL, Gosselies), Steinfeld (Clinique Saint Jean, Site Botanique, Brussels); Brigode (Clinique St Pierre, Ottignies); Tant (Erasme, Anderlecht); Francois (Europaziekenhuizen - St Michiel, Brussels); Van Bruwaene (H Hartziekenhuis, Roeselare); Van den Bergh (Hopital Sainte Therese, Montignies s/ Sambre); Zangerle (IFAC Marche, Aye); Declerck (Imeldaziekenhuis, Mechelen); Mindlin (Iris Sud, Brussels); Durez (Mont Godine, Yvoir); Ravelingien (OLV Aalst, Aalst); Van Essche (Private practice, Bonheiden), Cheroutre (Private practice, St Niklaas), Van den Bossche (Private practice, St Niklaas); Volders (Reumacentrum, Hasselt); Herman (St Blasius, Dendermonde); Coutellier (St Luc Bouge, Jambes); Vanneuville (SZ Roeselare, Roeselare); Gyselbrecht, Van Den Berghe (SZA, Aalst); Verbruggen (UZ Brussels, Brussels), Aspeslagh, Carron, De Keyser, Elewaut, Malfait, Mielants, Piette, Stubbe, Van den Bosch, Vander Cruyssen, Verbruggen (UZ Ghent, Ghent); Westhovens (UZ Leuven, Leuven); Lechkar (UZA, Edegem); Corluy (Virga Jesse Ziekenhuis, Hasselt); Hirsch (Zitha Kliniek, Luxembourg); Berghs, Geussens, Vanhoof (ZOL St Jan, Genk).
Footnotes
-
Published online before print August 15, 2014
-
The Belgian MIRA cohort was supported by the Royal Belgian Society for Rheumatology (KBVR/SRBR) and an unrestricted grant from Roche (Basel, Switzerland).
- Accepted for publication May 15, 2014.








{kind=link}
{kind=link}