

Abstract
Objective. To evaluate the safety and efficacy of once-weekly subcutaneous rilonacept 160 mg for prevention of gout flares in patients initiating or continuing urate-lowering therapy (ULT).
Methods. This phase III study was conducted in the United States, South Africa, Europe, and Asia. Adults (n = 1315, 18–80 yrs) with gout, who were initiating or continuing ULT, were randomized to treatment with weekly subcutaneous injections of rilonacept 160 mg or placebo for 16 weeks followed by a 4-week safety followup. The primary endpoint was safety, assessed by adverse events (AE) and laboratory values. Efficacy was a secondary endpoint.
Results. Demographic and clinical characteristics were similar between treatments; predominantly male (87.8%), mean age 52.7 ± 11.3 years. Patients with ≥ 1 AE were 66.6% with rilonacept versus 59.1% placebo, with slightly more AE-related withdrawals with rilonacept (4.7% vs 3.0%) because of the greater incidence of injection site reactions (15.2% rilonacept, 3.3% placebo). Serious AE were similar in both groups, as were serious infections (0.9% placebo, 0.5% rilonacept); no tuberculosis or opportunistic infections occurred. Most common AE were headache, arthralgia, injection site erythema, accidental overdose, and pain in extremity. Of the 6 deaths, only 1 in the placebo group was considered treatment-related. At Week 16, rilonacept resulted in 70.3% fewer gout flares per patient (p < 0.0001), fewer patients with ≥ 1 and ≥ 2 gout flares (p < 0.0001), and 64.9% fewer gout flare days (p < 0.0001) relative to placebo.
Conclusion. Weekly subcutaneous administration of rilonacept 160 mg showed no new safety signals. The safety profile was consistent with previous studies. Rilonacept also significantly reduced the risk of gout flares. Clinicaltrials.gov identifier NCT00856206; EudraCT No. 2008-007784-16.
Gout, the most common form of inflammatory arthritis among men, is associated with substantial medical and economic burdens resulting from reduced quality of life, high healthcare resource use, and reduced work productivity1,2,3. Studies have further suggested that these burdens are greater among patients with more frequent gout flares and those with tophi4,5.
The primary goal of gout management is to reduce serum urate to target levels < 6 mg/dl through lifestyle modification and use of pharmacologic urate-lowering therapies (ULT), including allopurinol, probenecid, febuxostat, and pegloticase6. Unfortunately, ULT may increase the risk of gout flares, and gout management guidelines recommend concomitant use of colchicine or nonsteroidal antiinflammatory drugs (NSAID) for prophylaxis of ULT-associated gout flares7. However, these prophylactic agents are associated with well-recognized side effects, and the presence of specific comorbid conditions, especially in an older population, may pose barriers to their use8,9. An inability to use conventional gout flare prophylaxis may contribute to the reported low rate of patient adherence to ULT10,11,12,13. Further, hyperuricemia itself is clinically relevant in the context of other renal and cardiometabolic disorders14,15,16,17, with an apparent reciprocal relationship between these comorbidities and gout, because their presence may increase the risk of gout flares18. These interactions between gout and comorbid conditions increase the complexity of disease management, and suggest the need for flare prophylaxis agents that have a more favorable safety and tolerability profile in selected patients.
Interleukin 1 (IL-1) is a cytokine that drives a number of inflammatory pathways, including those involved in gouty arthritis that are initiated by crystal-induced activation of the multiprotein NLR family, pyrin domain containing 3 inflammasome19,20,21. The utility of inhibiting IL-1 in gout was demonstrated in case reports22,23,24 and clinical studies of rilonacept and other IL-1 inhibitors25,26,27,28. Recent studies with rilonacept further support the rationale for IL-1 as an appropriate therapeutic target for prevention of gout flares in patients initiating ULT27,28,29.
Rilonacept is a fully human, soluble decoy receptor that binds IL-1α and IL-1β, preventing their activation of cell surface receptors30. It is approved for treatment of the IL-1 mediated cryopyrin-associated periodic syndromes, specifically familial cold autoinflammatory syndrome and Muckle-Wells syndrome31,32. Although the efficacy of rilonacept to reduce gout flares in patients initiating ULT was confirmed in phase II and III trials27,28,29, it was important to demonstrate the safety of rilonacept, as well as its efficacy, in a large population that may be more representative of the clinical gout population than has been evaluated in previous trials. A more representative population would include patients who are continuing ULT as well as those initiating ULT, and patients with relevant comorbid conditions. The purpose of this international study was to evaluate the safety and tolerability of 160 mg subcutaneous rilonacept once weekly for gout flare prevention in a large population with these clinically relevant characteristics; efficacy was evaluated as a secondary endpoint.
MATERIALS AND METHODS
Study design and population
RESURGE (REview of Safety Using Rilonacept in preventing Gout Exacerbations) was a phase III, randomized, double-blind, placebo-controlled trial that enrolled patients with intercritical gout from study sites in Germany, India, Indonesia, South Africa, Taiwan, the United Kingdom, and the United States. This study was approved by local ethics committees or institutional review boards, and was performed in accordance with the current revision of the Declaration of Helsinki; all patients provided written informed consent prior to participation. Clinicaltrials.gov identifier NCT00856206; EudraCT No. 2008-007784-16.
For enrollment, patients were required to be 18–80 years of age with a history of gout (presence of either ≥ 6 of the 13 American College of Rheumatology 1977 preliminary criteria for the classification of acute arthritis of primary gout33 or monosodium urate microcrystals in joint fluid), who were initiating or recently initiated ULT (allopurinol, probenecid, sulfinpyrazone, or febuxostat) and were at risk for a gout flare. For patients already taking ULT, those treated for more than 2 months were required at screening/baseline to have either serum uric acid ≥ 7.0 mg/dl (416 μmol/l) or visible tophi. Exclusion criteria included an acute gout flare within 2 weeks before screening; intolerance to allopurinol or inadequate urate-lowering response to allopurinol; use of glucocorticoids within 4 weeks, or use of NSAID or colchicine within 2 weeks of screening; estimated glomerular filtration rate < 30 ml/min; chronic or active infections, or recent treatment with antiinfective agents; evidence of current or previous history of tuberculosis; and use of systemic immunosuppressants within 6 months prior to baseline. Pregnant or lactating women were also excluded, as were both men and women of reproductive potential unwilling to use adequate contraception throughout the study.
Randomization and treatment
Using an interactive voice response system, patients were randomly allocated in a 3:1 ratio to receive weekly subcutaneous rilonacept or placebo for 16 weeks. The study sample size was chosen to result in at least 900 rilonacept-treated patients to provide a sufficient rilonacept safety dataset when combined with other studies.
A loading dose of rilonacept 320 mg or placebo was administered in 2 equal volumes on Day 1 of treatment, followed by 15 weekly doses of rilonacept 160 mg or placebo with a safety followup performed 5 weeks after the last study drug injection. To maintain blinding, rilonacept and placebo were both supplied as a lyophilized powder in sterile, single-use vials. Each vial contained an extractable volume of 2 ml of rilonacept (for a 160 mg dose) or placebo after reconstitution with sterile water for injection. Alternatively, a subset of patients were treated with rilonacept or placebo presented as a sterile liquid formulation in a prefilled syringe.
For patients initiating allopurinol, the starting dose was 300 mg with subsequent titration every 2 weeks in 100 mg increments up to 800 mg/day to attain serum uric acid < 6 mg/dl (about 357 μmol/l). The initial allopurinol dose was adjusted for renal impairment based on baseline creatinine clearance estimated using the Cockroft-Gault equation34, with subsequent titration increments of 50 mg for those with estimated renal clearance < 60 ml/min. For patients initiating other ULT, initial dose and titration was as appropriate to achieve serum uric acid < 6 mg/dl. All ULT were continued during the 4-week safety followup. NSAID and/or oral glucocorticoids were permitted as rescue medication for acute gout flares at the investigators’ discretion while study treatments were continued.
Outcomes
Followup during treatment was performed by telephone contact at weeks 4, 12, and 20 (safety followup), and clinic visits at weeks 8 and 16. Patients also completed a daily diary beginning at onset of gout flare pain until resolution of all flare symptoms.
The primary endpoint of RESURGE was safety, based on incidence and types of treatment-emergent adverse events (AE), including serious AE (SAE) and clinically significant abnormal clinical laboratory variables over the 20-week study period. AE were graded by severity and assessed for causality by the investigator.
All efficacy endpoints were secondary and were assessed from Day 1 through Week 16 (end of the double-blind period). These endpoints included the mean number of gout flares per patient; the proportion of patients with ≥ 1 and ≥ 2 flares, the number of flare days, and time to first flare. A gout flare was defined as subject-reported acute articular pain typical of a gout attack that is deemed (by the subject and/or the investigator) to require treatment with an antiinflammatory medication. This definition was previously used as a primary outcome in phase II27, and as a secondary outcome in phase III trials of rilonacept in gout flare prophylaxis. This definition of gout flare was used in the absence of a validated definition35, although a provisional definition has been proposed since initiation of this trial36.
Statistical analysis
The full analysis set was the primary analysis population, and consisted of all randomized subjects who received any study medication. No formal statistical testing was performed for the primary endpoint of safety; AE are reported by number and proportions of patients with the event. For secondary endpoints, the number of gout flares and number of flare days were analyzed using the Wilcoxon rank sum test with exact method using Monte Carlo estimation. Fisher’s exact test was used for variables that were proportions, and time to first flare was analyzed using Kaplan-Meier plots; for statistical analyses, a 2-sided α < 0.05 was taken to indicate significance.
RESULTS
Demographics and disposition
A total of 1315 patients were randomized to rilonacept 160 mg (n = 985) or placebo (n = 330). Overall, 83.7% of patients completed the study through Week 16; a similar proportion of patients discontinued in each treatment group (Figure 1), 16.4% (n = 54) and 16.3% (n = 161) on placebo and rilonacept, respectively. A Kaplan-Meier survival curve showing discontinuations through the end of the study is presented in Appendix 1. There were 3 withdrawals due to lack of efficacy, 1 (0.3%) with placebo and 2 (0.2%) with rilonacept, and withdrawals due to AE were 3.0% with placebo and 4.7% with rilonacept. Data from all patients were available for the safety analysis.

Patient disposition.
Demographic and clinical characteristics were generally similar between the treatment groups (Table 1). Although the population was racially mixed, patients were predominantly men (87.8%) with a mean ± SD age of 52.7 ± 11.3 years, and a mean body mass index of 32.1 kg/m2 ± 6.7. Duration of gout was 10.7 ± 9.3 years and 29.0% of patients had tophi. The proportion of patients initiating ULT was similar in both groups, as was the proportion currently using ULT (Table 1). Allopurinol was the most commonly used ULT (98.6%), and 39% of patients were naive to allopurinol. Additionally, patients were characterized by a substantial comorbidity burden that included not only a variety of musculoskeletal conditions (48.9%), but also hypertension (52.9%), hypercholesterolemia (16.8%), renal and urinary disorders (14.1%), and cardiac disorders (11.5%).
Baseline demographic and clinical characteristics.
Exposure and adherence
Adherence to study drug injections was high in both treatment groups; 91.8% and 91.4% of rilonacept and placebo patients, respectively, had 80%–100% adherence. Among the 209 placebo and 614 rilonacept patients who initiated allopurinol, the mean ± SD final daily allopurinol dose was 342.4 ± 123.6 mg/day for placebo and 325.4 ± 115.6 mg/day for rilonacept. Among the 114 placebo and 363 rilonacept patients continuing on allopurinol, the final allopurinol dose was 251.3 ± 90.1 mg/day for placebo and 247.5 ± 100.5 mg/day for rilonacept.
At endpoint, the mean ± SD serum urate levels were reduced similarly between treatments, from 8.2 ± 2.0 to 5.8 ± 1.5 mg/dl in the placebo group, and from 8.0 ± 1.9 to 5.7 ± 1.4 mg/dl in the rilonacept group. At baseline, 16.4% of placebo patients and 14.4% of rilonacept patients had uric acid concentration < 6 mg/dl. At the end of the double-blind period, these proportions were 63.3% and 65.2% for the 275 placebo patients and 823 rilonacept patients who had these values available, respectively.
Safety
About 66% of patients treated with rilonacept reported an AE compared with 59% of patients in the placebo group. In addition, there were slightly more withdrawals due to AE in the rilonacept group (4.7% vs 3.0%; Table 2). The higher rate of withdrawals with rilonacept was primarily due to the greater incidence of injection site reactions (15.2% vs 3.3%) that were also the primary reason for AE-related withdrawals in this treatment group. AE were generally mild (nonsignificant interference with normal functioning) to moderate (some impairment with normal functioning) in severity. Serious AE occurred with a similar frequency in both treatment groups (Table 2), and only 3 of 44 were deemed to be related to study medication: 2 in the placebo group (1 death and 1 case of cellulitis) and 1 with rilonacept (drug eruption).
Treatment-emergent adverse events (AE) through Week 20 reported in ≥ 5% of patients in either treatment group.
The types and incidences of AE by system organ class were similar between treatment groups, except for general disorders and administration site conditions, which was driven primarily by a higher frequency of injection site reactions with rilonacept (Table 2). The most common AE, reported in ≥ 5% of patients in either group by preferred term, were headache, arthralgia, injection site erythema, accidental overdose, and pain in extremity. Among these AE, the incidence was similar between treatments except for injection site erythema (6.2% rilonacept, 0.3% placebo). The incidence of serious infections was similar between the treatment groups, 0.5% with rilonacept and 0.9% with placebo. There were no cases of tuberculosis or opportunistic infections.
Administration of a study drug injection in excess of the scheduled weekly dose was identified as an accidental overdose (Table 2), and included doses following the last scheduled injection (the majority) as well as doses during the treatment period taken fewer than 7 days after the previous dose. Both treatment groups experienced a similar incidence of accidental overdose, and none of the events included new signs or symptoms of an AE.
There were 6 deaths during the study (3 each in the placebo and rilonacept groups), of which 3 (2 placebo and 1 rilonacept) occurred post-treatment. In the placebo group, 1 death was of unknown cause and was considered by the investigator to be related to study treatment. Other causes of death, not assessed as treatment-related, included 2 myocardial infarctions (rilonacept), 1 cerebrovascular event (rilonacept), 1 sudden cardiac death (placebo), and 1 collapsed lung (placebo).
Treatment with rilonacept was associated with small mean increases in alanine aminotransferase (ALT), aspartate aminotransferase (AST), triglycerides, and creatine phosphokinase (CPK). Mean values at 16 weeks were 38.8 ± 24.0 IU/l for ALT, 30.4 ± 16.4 IU/l for AST, 265.5 ± 250.8 mg/dl for triglycerides, and 182.6 ± 255.5 IU/l for CPK, relative to baseline values of 31.3 ± 16.5 IU/l, 25.6 ± 9.3 IU/l, 225.6 ± 186.0 mg/dl, and 154.8 ± 136.7 IU/l, respectively. Similarly, there were small mean decreases with rilonacept in neutrophil and platelet counts, mean values of 3.6 ± 1.5 and 217.9 ± 56.1 × 103/μl, respectively, but few of these changes were clinically significant and most cases resolved by the post-treatment observation period. Among the hematologic changes of potential significance, neutrophil values were < 1500 cells/μl in 3 (1.0%) placebo patients and 30 (3.3%) rilonacept patients during the treatment period, in which AE during the low neutrophil count were reported in 1 placebo patient (bacteruria) and 2 rilonacept patients (rhinitis and influenza). Neutrophil counts < 1000 cells/μl were observed in 5 rilonacept patients (0.5%); no AE were associated with these events. The 4 events of neutropenia led to dose suspension or termination in the rilonacept group, but they did not lead to withdrawal from the study and these patients remained in the study for safety observation. Few hematologic or laboratory test abnormalities were reported as AE. Hematologic AE included 2 patients (0.2%) with decreased neutrophils in the rilonacept group, and 1 case each of increased eosinophils and decreased white blood cells in the placebo group. Laboratory test abnormalities reported as AE included increases in ALT in 2 (0.6%) placebo patients and 11 rilonacept (1.1%) patients; increased AST, abnormal liver function tests, and increased transaminases in 6 (0.6%), 3 (0.3%), and 2 (0.2%) patients in the rilonacept group, respectively, with no occurrences in the placebo group; increased blood triglycerides in 2 (0.6%) placebo patients and 12 (1.2%) rilonacept patients; single instances in both treatment groups of increased blood CPK, blood cholesterol, and low-density lipoprotein, with single instances in the rilonacept group of increases in blood bilirubin and blood uric acid hepatic enzyme; and a single case of increased blood calcium (placebo).
Efficacy
Significant divergence from placebo in the number of gout flares per patient was observed in patients receiving rilonacept as early as 4 weeks after initiating treatment, the earliest prespecified analysis timepoint (p < 0.0001; Figure 2). This difference was maintained over the double-blind treatment period, such that at Week 16, the rilonacept group was characterized by a 70.3% reduction in the mean number of gout flares per patient relative to placebo, from 1.73 (95% CI 1.44, 2.02) to 0.51 (95% CI 0.44, 0.59; p < 0.0001; Figure 2). Reductions in gout flares at Week 16 in each treatment group among patients who initiated allopurinol were similar to reductions among those who continued allopurinol, and were consistent with that observed for the overall population (data not shown). When stratified by the presence of tophi, more flares occurred in patients with tophi during the 16 weeks. At Week 16, flares per patient with tophi were 2.07 ± 2.90 and 0.87 ± 1.56 for placebo and rilonacept, respectively, and for those without tophi, 1.58 ± 2.60 for placebo and 0.37 ± 0.94 for rilonacept.
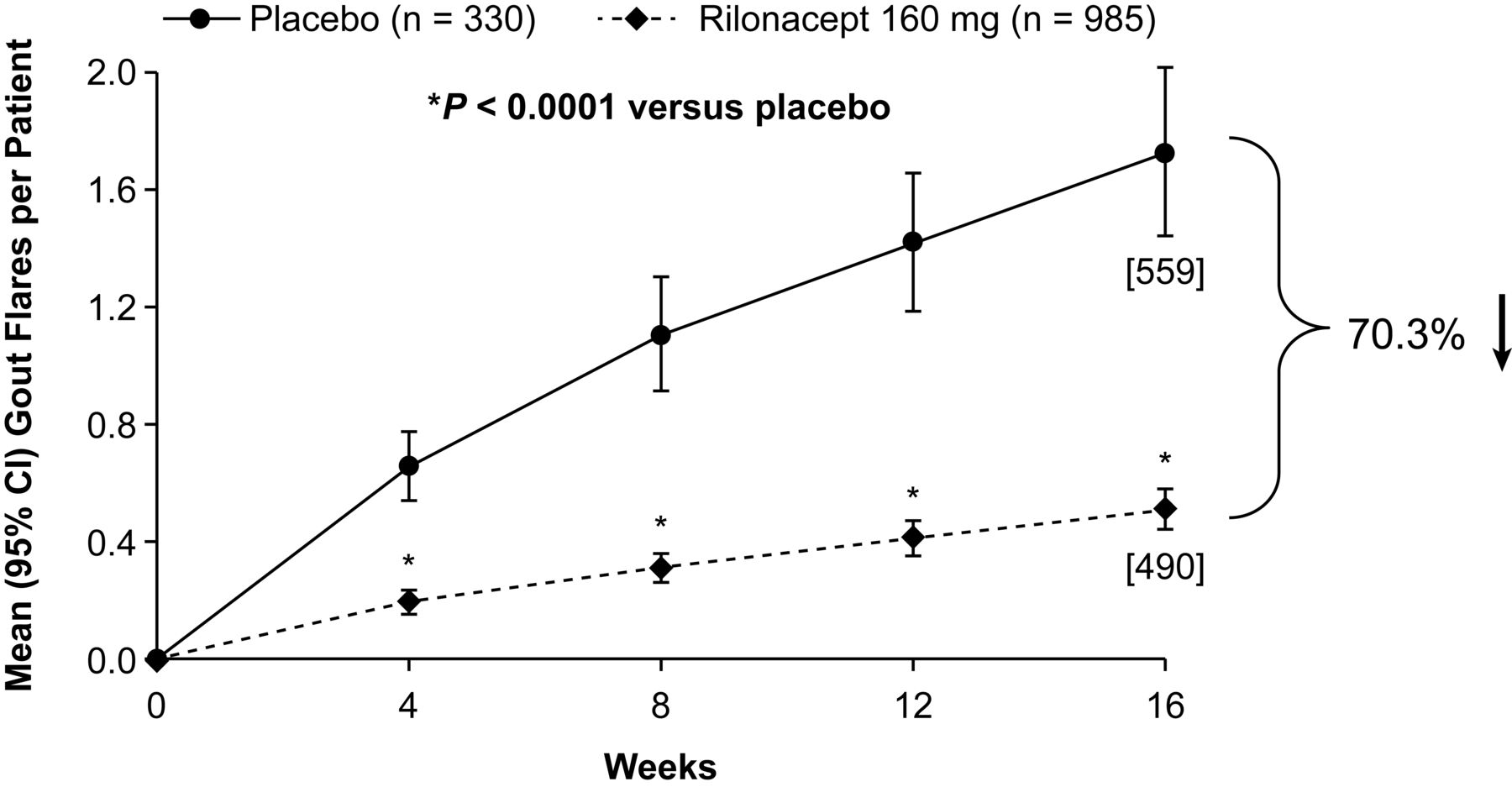
Gout flares per patient through Week 16. Numbers in brackets represent cumulative number of flares at Week 16.
At Week 16, significantly fewer patients had gout flares with rilonacept relative to placebo (Figure 3). The proportion of patients who reported ≥ 1 flares by Week 16 was 51.1% with placebo and 25.7% with rilonacept, a reduction of 49.6% (p < 0.0001), and for ≥ 2 gout flares, the proportions were 34.7% and 11.7%, respectively, representing a reduction of 66.4% with rilonacept (p < 0.0001; Figure 3).
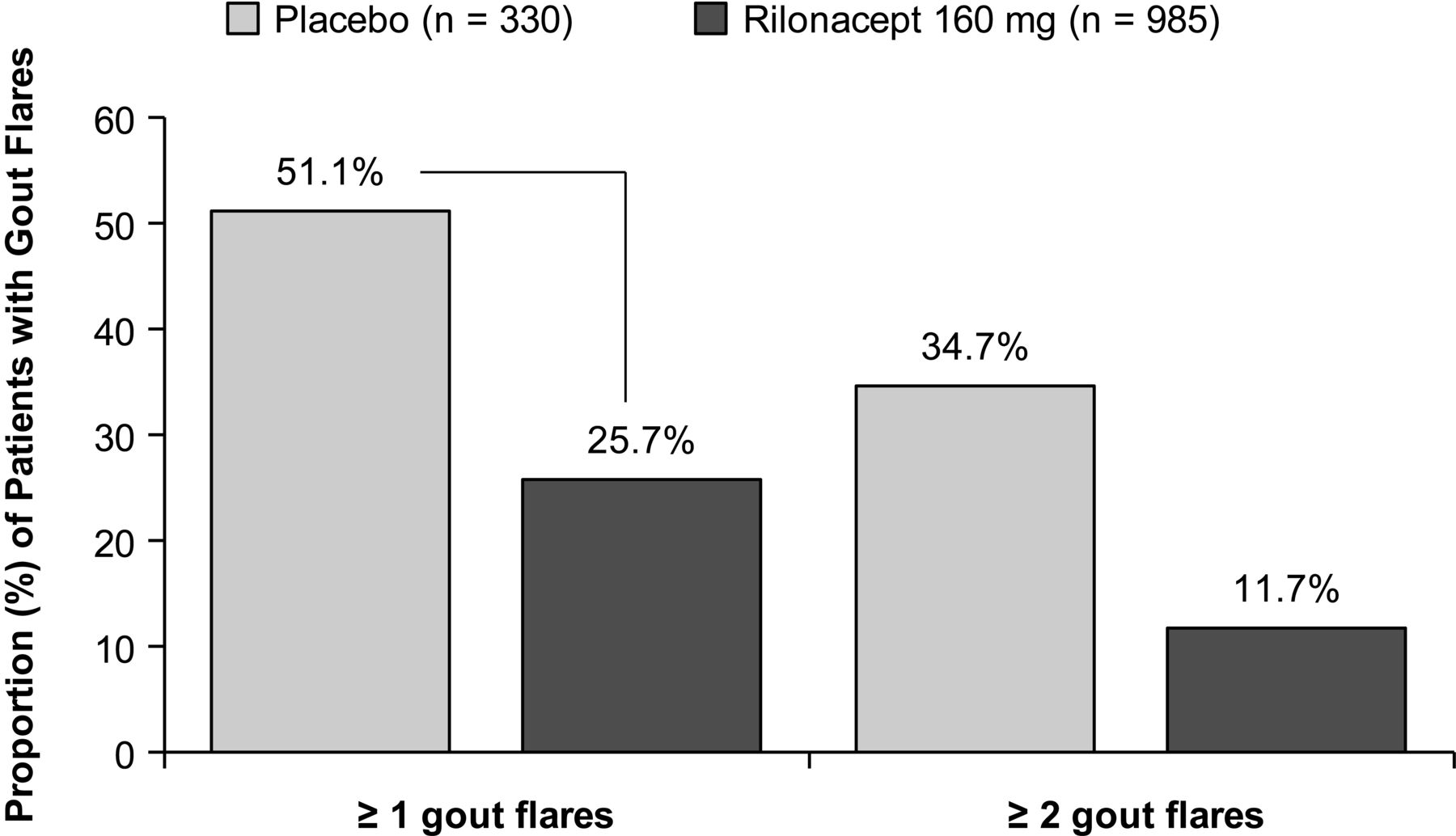
Proportion of patients with gout flares through Week 16.
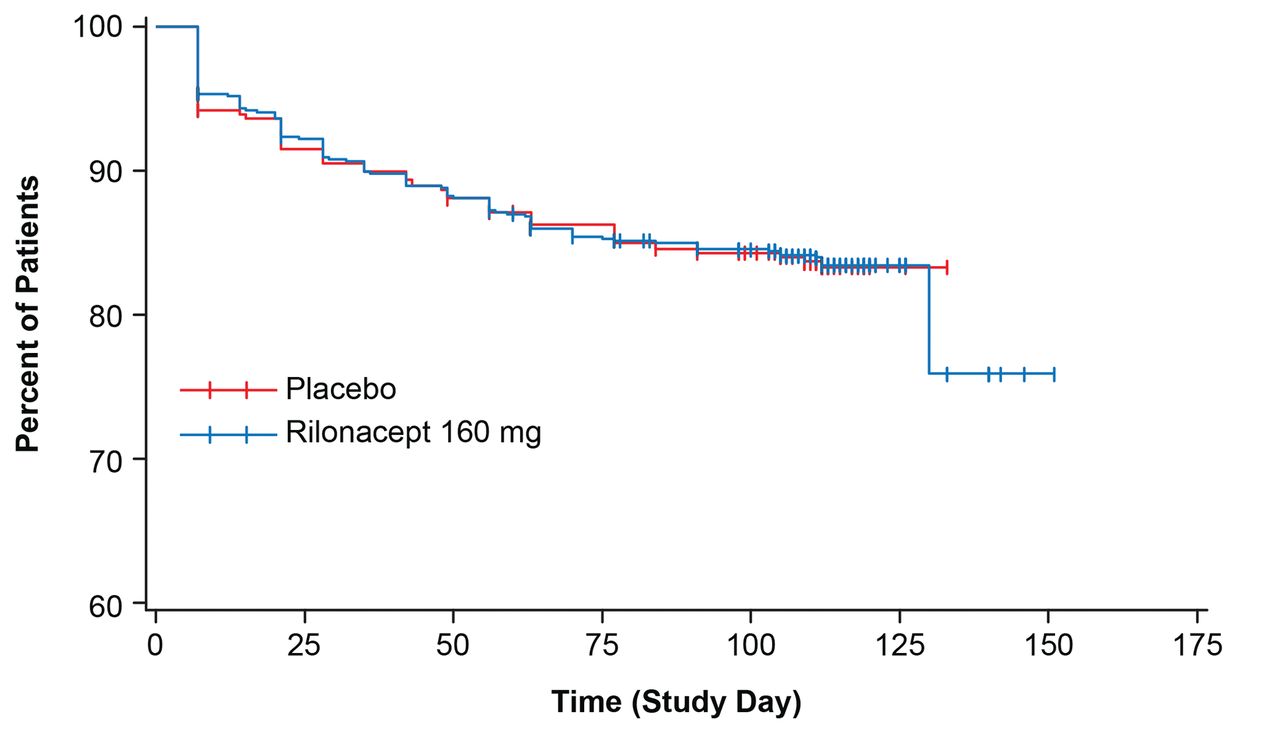
The total number of flare days per patient at Week 16 was 7.7 (95% CI 6.4, 9.0) in the placebo group and 2.7 (95% CI 2.2, 3.2) with rilonacept, a reduction of 64.9% with rilonacept that was statistically significant (p < 0.0001). Based on Kaplan-Meier survival analysis, time to first gout flare was significantly longer with rilonacept relative to placebo (Figure 4; p < 0.0001). While the median time to first gout flare was 87 days in the placebo group, median time to first flare could not be estimated for rilonacept, because less than half the patients (25.7%) reported flares.

Kaplan-Meier estimates of time to first gout flare from Day 1 through Week 16.
DISCUSSION
Currently recommended pharmacologic strategies for gout management are generally effective and well tolerated. However, impediments to real-world effectiveness include low patient adherence to ULT and tolerability or safety issues related to recommended agents for gout flare prevention in selected patients9,10,11. The results presented in our study support the favorable safety and tolerability profiles of rilonacept that have been reported in previous studies of gout flare prophylaxis27,28,29. Strengths of the current study include the large and diverse population, as well as patient characteristics that likely reflect clinical practice. These characteristics included not only a substantial proportion of patients continuing ULT (35.7%), in contrast to the previous studies in which all patient initiated ULT at the time of rilonacept treatment, but also the presence of clinically relevant comorbidities such as cardiovascular-related and renal conditions. The additional demonstration of a significant gout flare reduction with rilonacept relative to placebo, also consistent with the other studies, supports a potential role for rilonacept as adjunctive therapy to ULT, especially in patients for whom gout flare prevention with colchicine or NSAID is an undesirable option.
Patients in our study had a high rate of adherence to study drug injections and a low rate of study withdrawal (about 16%), with only 3.0% and 4.7% of placebo and rilonacept patients, respectively, discontinuing because of AE.
Although the overall incidence of AE was higher with rilonacept relative to placebo, most AE were mild to moderate in severity, and there were no new safety signals. There was no signal of an increase in SAE with rilonacept. The incidence of AE-related withdrawals with rilonacept was primarily due to injection site reactions, which were the most common treatment-related AE, and accounted for much of the increase in treatment-related AE as has previously been reported27,28,29.
While the occurrence of infections has been a general concern with biologic anticytokine therapies37, there was no evidence of a signal for increased infections, and there were no cases of tuberculosis or other opportunistic infections with rilonacept. The few infections reported as SAE were balanced between treatments (0.9% placebo, 0.5% rilonacept). Observed changes in hematologic and laboratory values that were considered clinically significant occurred more frequently with rilonacept; these were uncommon, and none was associated with a clinical AE or withdrawal from the study.
Of the 6 deaths, the 1 considered related to treatment was in the placebo group. There were 4 deaths related to cardiovascular or cerebrovascular events, and these may not be unexpected considering the substantial presence of cardiovascular comorbidities and evidence suggesting that gout itself may be associated with increased cardiovascular mortality38,39.
Because almost half the patient population (48.9%) had a history of musculoskeletal disorders, it is also not surprising that one of the most frequently reported AE was musculoskeletal pain. While it should also be noted that reported AE were those considered by a diverse set of international investigators, the overall AE profile was consistent with other studies of rilonacept in gout27,28,29.
The efficacy benefits were similar to those reported in previous phase III studies and were observed early after initiation of treatment, with maintenance of the effects over the duration of treatment. These benefits included a 70.3% reduction in mean number of gout flares per patient; reductions of 72.6% and 80.0% with rilonacept 160 mg were reported as the primary endpoints in other phase III studies28,29. Rilonacept demonstrated efficacy regardless of tophi status, and in patients who were initiating as well as continuing allopurinol therapy. Further, about 75% of the rilonacept-treated patients remained flare-free, a proportion that is consistent with the 80%–84% in the other studies.
Unlike prior studies, this trial allowed use of ULT other than allopurinol. However, few patients (1.9%) actually used alternatives to allopurinol. The risk of flares may be attributed to the rate at which serum urate levels decrease during ULT, rather than to specific ULT or their mechanism of action. We expect that the ability of rilonacept to decrease gout flares is not likely to be altered with use of other ULT. It should also be noted that serum urate levels were similarly reduced in both treatment groups, suggesting that there is no apparent interaction between rilonacept and the effectiveness of ULT.
Our study could be criticized for using a broader definition of gout flares than that in proposed recommendations36. However, when this broader definition was used as a sensitivity analysis in a previous study, the results were comparable to one using the more conservative definition29.
Weekly subcutaneous administration of rilonacept 160 mg had an acceptable safety and tolerability profile in patients with gout initiating or continuing ULT and having a substantial prevalence of comorbidities. The type and incidence of AE were consistent with previous trials and there were no new safety signals. The additional demonstration of significantly better efficacy relative to placebo, albeit as a secondary endpoint, was also consistent with previous studies. These results expand the available data on rilonacept and support its utility for gout flare prevention. The observation that rilonacept results in benefits early after initiation of treatment suggests that it might be appropriate both for patients initiating ULT and those already receiving ULT who are at risk of flares.
APPENDIX 1.

Kaplan-Meier estimates of time to study discontinuation.
Footnotes
-
Funding provided by Regeneron Pharmaceuticals, Tarrytown, NY. Editorial support provided by E. Jay Bienen and funded by Regeneron Pharmaceuticals Inc.
- Accepted for publication April 10, 2014.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}