

Abstract
Objective. To identify biomarkers for bone metabolism in patients with ankylosing spondylitis (AS) and to determine the relationship between these biomarkers and disease activity, back mobility, osteoproliferation, and bone mineral density (BMD).
Methods. Serum levels of Wingless protein (Wnt-3a), Dickkopf-1 (DKK-1), sclerostin, soluble receptor activator of nuclear factor-κB ligand (sRANKL), and osteoprotegerin were assessed using ELISA. Ankylosing Spondylitis Disease Activity Score-C reactive protein, Bath Ankylosing Spondylitis Disease Activity Index, Bath Ankylosing Spondylitis patient global score, and C-reactive protein (CRP) were used as disease activity measures, and Bath Ankylosing Spondylitis Metrology Index (BASMI) as a measure of spinal mobility. Lateral spine radiographs were scored for chronic AS-related changes (mSASSS). BMD was measured with dual-energy x-ray absorptiometry.
Results. Two hundred four patients with AS (NY criteria; 57% men), with a mean age of 50 ± 13 years and disease duration 15 ± 11 years, and 80 age and sex-matched controls were included. The patients with AS had significantly higher serum levels of Wnt-3a (p < 0.001) and lower levels of sclerostin (p = 0.014) and sRANKL (p = 0.047) compared with the controls. High CRP was associated with low sclerostin (rS = −0.21, p = 0.003) and DKK-1 (rS = −0.14, p = 0.045). In multiple linear regression analyses, increasing BASMI and mSASSS were independently associated with older age, male sex, high CRP, and elevated serum levels of Wnt-3a. In addition, mSASSS remained associated with a high number of smoking pack-years after adjusting for age. Low BMD of femoral neck was associated with high mSASSS after adjusting for age.
Conclusion. Serum levels of Wnt-3a are elevated in AS and associated with increased BASMI and mSASSS, independent of age, indicating that Wnt-3a could be a biomarker for the osteoproliferative process.
Ankylosing spondylitis (AS) is a chronic rheumatic disease characterized by sacroiliac and spinal inflammation and the growth of bony spurs (syndesmophytes) between the vertebrae. Syndesmophyte formation is associated with restriction of spinal mobility. Pathologic new bone is mainly formed by endochondral ossification, but membranous ossification also contributes1,2. Inflammation and osteoproliferation are at least partially uncoupled events in AS, because osteoproliferation can occur even if the inflammatory activity is low. Although inflammation can be treated successfully with blockers of tumor necrosis factor (TNF-α), several 2-year followup studies have shown a lack of effect on syndesmophyte formation3,4,5. In one observational study, however, patients with AS taking TNF inhibitors were followed for up to 5 years, and TNF inhibition appeared to reduce radiographic progression6. Daily or high use of nonsteroidal antiinflammatory drugs (NSAID) has been associated with less radiographic progression, but a truly effective treatment against new bone formation in AS has yet to be found7,8,9.
Parallel to the osteoproliferation, patients with AS also have an increased loss of trabecular bone, resulting in an elevated risk for vertebral fractures, sometimes complicated by neurological injuries10,11. Prevalences of osteoporosis of 19% to 62% and vertebral fractures of 9% to 42% have been reported from different AS cohorts10,12,13,14. These 2 enhanced but opposite bone processes create diagnostic and therapeutic problems. Osteoproliferative changes cause an artifactual increase in lumbar bone mineral density (BMD). Levels of bone biomarkers can be difficult to interpret if they mirror both processes. Treating and preventing osteoproliferation could potentially worsen osteoporosis and vice versa, and the knowledge is missing about which time window to use to treat these 2 conditions. There is a need for biomarkers for both the osteoproliferation and the osteoporosis to guide physicians in the decision of who to treat, when to treat, and how to follow up.
The bone morphogenic proteins, hedgehogs, and wingless proteins (Wnt) are important regulators of bone formation by intracellular signaling pathways that affect gene transcription. Wnt can signal by at least 4 different pathways, of which the “canonical” Wnt/β-catenin pathway is best described. Wnt/β-catenin signaling stimulates osteoblast differentiation, proliferation, and survival resulting in increased bone mass, whereas suppressed signaling leads to bone loss15,16,17. Wnt signaling also triggers the formation of osteophytes18. The Wnt signaling is regulated by several secreted receptor antagonists. Dickkopf-1 (DKK-1), expressed mainly by osteoblasts and osteocytes, and sclerostin, expressed exclusively by osteocytes, are negative regulators of bone formation by binding to Wnt coreceptors19,20. The expression of sclerostin in the osteocytes is reduced by mechanical loading21,22. Insufficient or excess activity of DKK-1 or sclerostin in bone results in increased or decreased bone density, respectively16,23.
Osteoclast maturation requires macrophage colony stimulating factor (M-CSF) and receptor activator of nuclear factor-κB ligand (RANKL)24,25. RANKL binds to RANK on osteoclast precursors, inducing their transformation into mature osteoclasts and thus has a resorptive effect on bone. The RANKL expression is enhanced by proinflammatory cytokines. The RANK-RANKL interaction is inhibited by osteoprotegerin (OPG), a decoy receptor for RANKL that has an antiresorptive effect on bone.
The goal of our study was to identify biomarkers of importance for both osteoporosis and osteoproliferation in AS. The specific aims of the study were to compare the serum concentrations of a panel of biomarkers reflecting bone metabolism in patients with AS versus in healthy controls and to analyze the relationship between these biomarkers and disease activity, back mobility, osteoproliferation, and BMD. The biomarkers studied were Wnt-3a, DKK-1, sclerostin, soluble RANKL (sRANKL), and OPG.
MATERIALS AND METHODS
Patients
All patients with AS (modified New York criteria) who were registered at the departments of rheumatology at the Sahlgrenska University Hospital and Hospitals of Alingsås and Borås were invited to participate. Exclusion criteria were psoriasis, inflammatory bowel disease, dementia, other concomitant rheumatic disease, and difficulties in understanding Swedish. The inclusion of the patients has been described10,26. The patients all gave written informed consent according to the Declaration of Helsinki and the study was approved by the Regional Ethics committee in Gothenburg.
The patients answered questionnaires regarding medical history and medication including use of NSAID (daily or on-demand) and TNF-α blockers. Disease activity was assessed using the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), the Ankylosing Spondylitis Disease Activity Score with C-reactive protein (ASDAS-CRP), and the Bath Ankylosing Spondylitis patient global score (BAS-G). Spinal mobility was measured for calculation of the Bath Ankylosing Spondylitis Metrology Index (BASMI)27,28.
The patients were asked about current and previous smoking, age at onset and disruption of smoking, and average daily cigarette consumption. Smoking pack-years were subsequently calculated.
Healthy controls
Blood samples from healthy sex and age-matched blood donors were collected to use as controls to the AS patients. The blood donors were recruited while giving blood at Sahlgrenska University Hospital. The blood donors all gave their written informed consent and answered questionnaires stating that they were in full health.
Blood samples
Blood samples were drawn in a non-fasting state. Levels of hemoglobin, erythrocyte sedimentation rate (ESR), and CRP were analyzed using standard laboratory techniques at the hospitals. Serum was stored at −20ºC until needed for analysis.
Biomarkers of bone metabolism
Serum samples were assayed for markers of bone metabolism using specific ELISA kits according to manufacturers’ instructions. The biomarkers measured were Wnt-3a (Uscn Life Science Inc.), total DKK-1 (R&D Systems), sclerostin (Biomedica Gruppe), sRANKL (Biovendor), and OPG (Immunodiagnostic Systems). The following values of sensitivity were reported by the manufacturers: Wnt-3a lower limits of detection (LLD) = 0.055 ng/ml; DKK-1 LLD = 4.2 pg/ml; sclerostin LLD = 2.6 pmol/l; sRANKL LLD = 0.4 pmol/l; OPG LLD = 14 pmol/l.
Absorbance was read at 450 nm in SpectraMax 340PC384 spectrophotometer (Molecular Devices). The software SoftMax Pro 5.2 was used to calculate the biomarker concentrations.
Radiography and dual-energy x-ray absorptiometry (DEXA)
Lateral radiographs of the cervical and lumbar spine were scored for chronic AS-related changes using the modified Stoke Ankylosing Spondylitis Spine Score (mSASSS)29. The mSASSS scoring was done by an experienced radiologist, specialized in rheumatology and AS in particular. BMD was measured with DEXA (Hologic Discovery A, Hologic Inc.) in the femoral neck.
Statistical analyses
Statistical analyses were performed using PASW Statistics 18.0 (SPSS Inc.). Descriptive statistics are presented as median and range and/or mean and SD. Mann-Whitney U test or chi-square tests were used for comparisons between groups (patients/controls, men/women, ever-smokers/never-smokers, anti-TNF treated/non-treated). All correlations were calculated using Spearman’s correlation (rs). All tests were 2-tailed and p < 0.05 was considered statistically significant. Multiple linear regressions were run using a stepwise method with BASMI, mSASSS, and BMD of femoral neck as outcome. The linear regressions with mSASSS as outcome was run in 2 models. In the first model, conventional mSASSS score was used. In the second model, mSASSS was log-transformed and patients with only sacroiliitis (mSASSS = 0) were excluded, leaving data from 148 patients ready to analyze. This was done to make mSASSS normally distributed. Covariates in all multiple linear regressions were age, sex, smoking pack-years, CRP, and the biomarkers of bone metabolism, which were significantly associated with the outcome in the univariate analyses. In the model where BMD of femoral neck was the outcome, mSASSS was also included as a covariate. Age, sex, smoking, and CRP were chosen as covariates because they are known risk factors for osteoproliferation and osteoporosis.
RESULTS
Patients and healthy controls
In total, 204 patients with AS (87 women and 117 men) with a median age of 49 years (range 17–78), symptom duration of 24 years (2–55), BASDAI 3.5 (0–9.6), and ASDAS-CRP 2.3 (0.8–5.9) were included (Table 1).
Characteristics of 204 patients with ankylosing spondylitis in western Sweden.
The healthy control group consisted of 80 blood donors (26 women and 54 men) with a median age of 48 years (19–71). The age- and sex-distributions were not significantly different between the patients and the controls (Table 2).
Demographics and serum levels of biomarkers in patients with ankylosing spondylitis (AS) and in the controls.
Levels of biomarkers in AS compared with healthy controls
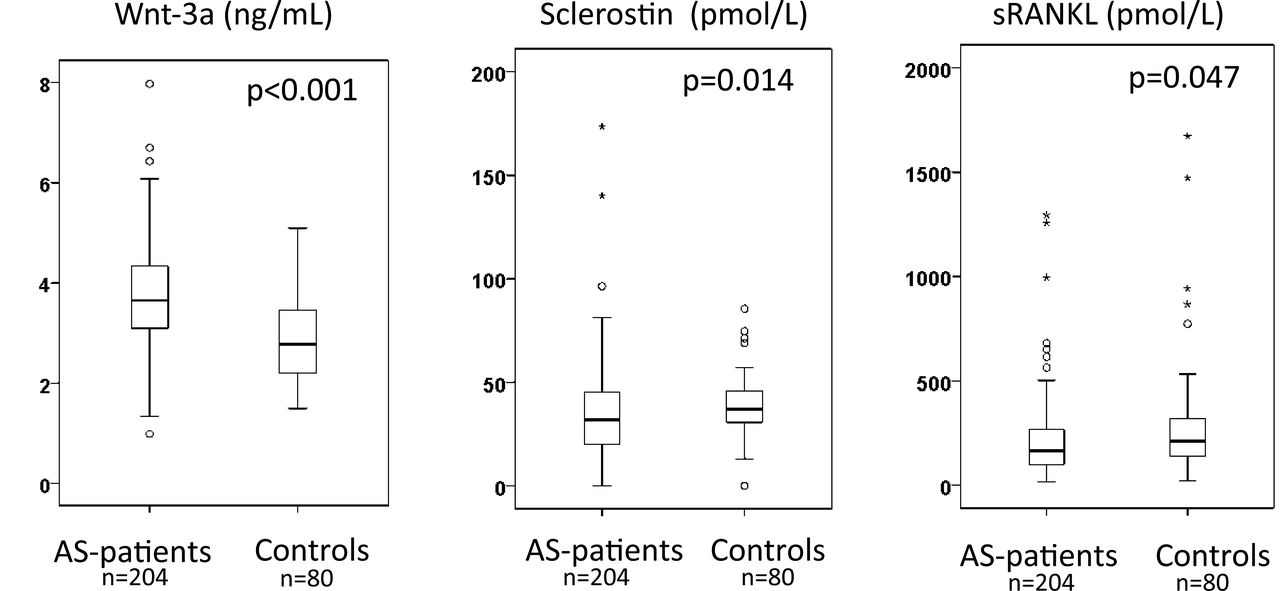
The patients with AS had significantly higher serum levels of Wnt-3a (p < 0.001), lower serum levels of sclerostin (p = 0.014), lower serum levels of sRANKL (p = 0.047), and lower sRANKL/OPG ratio (p = 0.022) compared with the healthy controls (Table 2 and Figure 1). The serum levels of DKK-1 showed a tendency to be higher in the patients with AS (p = 0.058).

Box plot showing serum levels of Wnt-3a, sclerostin, and sRANKL in the patients with AS in comparison with the healthy controls. Values are the medians (horizontal line), interquartile ranges (box), and ranges of values (whiskers). O (outliers) shows cases with values between 1.5–3.0 box lengths and stars (extremes) values more than 3 box lengths from the upper or lower edge of the box. Wnt: wingless proteins; AS: ankylosing spondylitis; sRANKL: soluble receptor activator of nuclear factor-κB ligand.
Correlation between the different biomarkers in the patients with AS
Sclerostin was positively correlated with DKK-1 and OPG. No significant correlation was found between Wnt-3a and the other biomarkers (Table 3).
Univariate analyses. Correlation matrix showing significant correlations (Spearman’s rho) between the biomarkers.
Age and biomarkers
Age was positively correlated with sclerostin and OPG, but negatively correlated with sRANKL in the patients with AS (Table 4).
Univariate analyses. Significant correlations (Spearman’s rho) between the biomarkers of bone metabolism and measures of disease activity, back mobility, chronic ankylosing spondylitis (AS)-related changes in the spine and bone mineral density (BMD). Data are rs: Spearman’s correlation coefficient, and p value.
Disease activity and back mobility and biomarkers
CRP was negatively correlated with both sclerostin and DKK-1. BASMI was positively correlated with Wnt-3a, sclerostin, and OPG (Table 4). No significant correlations were found between the biomarkers analyzed and BASDAI, ASDAS-CRP, BAS-G, ESR, or hemoglobin.
In multiple linear regression, increasing BASMI was independently associated with older age, male sex, high CRP, and elevated serum levels of Wnt-3a (Table 5).
Multivariate analyses. The results of the stepwise multiple linear regressions with BASMI, mSASSS, Log10 mSASSS, and femoral neck BMD as outcome.
Chronic AS-related changes in the spine, smoking, and biomarkers
mSASSS was significantly higher in the male patients compared with the female (20 ± 22 vs 6 ± 9; p < 0.001). mSASSS was positively correlated with Wnt-3a, sclerostin, CRP, age, and smoking pack-years (Table 4). Comparing the first (mSASSS = 0) and fourth (mSASSS ≥ 20) quartiles of mSASSS we found significantly higher Wnt-3a (3.98 ± 1.00 vs 3.49 ± 1.02 ng/ml, p = 0.005) and sclerostin (40.90 ± 23.07 vs 31.4 ± 17.65 pmol/l, p = 0.01), but lower DKK-1 (2.78 ± 0.94 vs 3.27 ± 1.58 ng/ml, p = 0.003) in the fourth quartile.
The smoking habits of the patients are displayed in Table 1. Smoking pack-years were positively correlated with mSASSS, BASMI, and age (Table 4). In comparison with never-smokers, the patients who smoked for at least 6 months of their lives (ever-smokers) had significantly higher mSASSS (mean 20 ± 22 vs 9 ± 15; p < 0.001), BASMI (mean 3.6 ± 1.6 vs 2.6 ± 1.4; p < 0.001), and age (mean 53 ± 12 vs 47 ± 13; p = 0.001). The distributions of sex, CRP, and the biomarkers of bone metabolism were equal between current smokers, ever-smokers, and never-smokers.
In multiple linear regression, high mSASSS was independently associated with age, male sex, smoking pack-years, and elevated levels of serum Wnt-3a. High log10 mSASSS was associated with age, male sex, high CRP, and elevated levels of serum Wnt-3a (Table 5).
BMD and biomarkers
In total, 5% of the patients had osteoporosis in the femoral neck and 10% osteoporosis in the lumbar spine. BMD results for this AS cohort are presented in more detail in a previous publication26. BMD of the femoral neck is not affected by the lumbar osteoproliferation in AS and was thus selected as the BMD measure to be compared with the levels of the biomarkers. BMD of the femoral neck was positively correlated with sRANKL, but negatively correlated with OPG and Wnt-3a (Table 4).
In multiple linear regression, low BMD of the femoral neck was independently associated with older age, female sex, and high mSASSS (Table 5).
Medication and biomarkers
A total of 20.6% (42/204) of the patients were treated with TNF-α blockers (n = 30 infliximab, n = 8 etanercept, n = 4 adalimumab). The patients treated with TNF-α blockers had significantly higher serum levels of Wnt-3a (4.02 ± 1.20 ng/ml vs 3.64 ± 0.92; p = 0.049) and sRANKL (410.54 ± 473.89 pmol/l vs 175.61 ± 112.88; p < 0.001), but lower serum levels of OPG (3.25 ± 0.87 pmol/l vs 3.84 ± 1.14; p = 0.002) compared with patients without a TNF-α blocker. There was no significant difference in age, BASMI, mSASSS, femoral neck BMD, or CRP between users and non-users of TNF-α blockers. The correlations between the biomarkers and BASMI, mSASSS, and BMD of femoral neck did not change in any significant way when the patients taking TNF-α blockers were excluded from the analysis. No significant difference in serum levels of the biomarkers was found between users (daily or on-demand) and nonusers of NSAID.
DISCUSSION
In our study the serum levels of Wnt-3a were significantly elevated in the patients with AS and associated with higher BASMI and mSASSS, but not with age. In addition, serum Wnt-3a remained independently associated with BASMI and mSASSS after adjusting for age, sex, smoking, and CRP in multiple linear regressions. The results indicate that serum Wnt-3a may be a marker for the osteoproliferative process in AS.
Wnt-3a was the first of the Wnt to be isolated from cell cultures in its active form and characterized30. It is reasonable to assume that Wnt-3a has osteoproliferative effects because it has been shown to activate both canonical and noncanonical Wnt pathways in mesenchymal stem cells and to promote osteoblast differentiation, proliferation, and survival31,32,33. Total knockout (KO) of Wnt-3a causes embryonic lethality in mice, but heterozygote KO mice display bone loss and low BMD and trabecular number34. Animal models give support to the importance of Wnt signaling in the osteoproliferative process of spondyloarthritides. Increased Wnt signaling caused by DKK-1-blocking antibodies has been shown to induce fusion of sacroiliac joints in mice transgenic for TNF35. In 1 mouse model, the DKK-1 blockage reversed the RA-like bone-destructive pattern to a more osteoarthritis (OA)-like bone-forming pattern with growth of osteophytes in the inflamed joints18.
Extensive syndesmophyte formation is a risk factor for osteoporosis and these conditions often coexist. Low BMD of the femoral neck was also correlated with higher Wnt-3a, but only in the univariate analysis.
In our study, high CRP levels were correlated with lower levels of both sclerostin and DKK-1, suggesting a possible connection between inflammation and reduced inhibition of Wnt signaling. Elevated CRP has been associated with increased syndesmophyte formation in AS and in early axial spondyloarthritis (SpA) in previous studies8,36. A recent study on patients with AS treated with TNF blockers also reported an association between persistently elevated CRP and low sclerostin37.
We found that DKK-1 was positively correlated with sclerostin, which is supported by a 2-year followup study on early AS that also reported significantly lower levels of DKK-1 measured with functional ELISA in patients with syndesmophyte growth compared with patients without syndesmophyte growth38. We found significantly lower DKK-1 in the patients with the highest mSASSS score. In our study, however, we measured total DKK-1 with sandwich ELISA.
Also supporting the role of Wnt signaling, we found significantly lower serum sclerostin in the patients with AS compared with healthy controls, a finding consistent with those of 2 previous studies37,39. We found that increasing levels of sclerostin were associated with increasing BASMI and mSASSS, which may be explained by sclerostin being positively correlated with age in both the patients with AS and the controls. In an earlier prospective study over 2 years, low serum sclerostin was associated with radiologic progression39. Decreased expression of sclerostin was also found in osteocytes in immunohistochemical analyses of zygapophyseal joints from patients with AS and in OA40.
Interestingly, we found that patients treated with TNF inhibition had higher serum levels of Wnt-3a, but no difference in serum levels of total DKK-1 was detected between the groups. Resolution of inflammation following anti-TNF treatment has been associated with new bone formation in AS41. It has been hypothesized that this could be caused by increased Wnt signaling and that TNF-α acts as a brake on bone formation by stimulating the expression of the Wnt antagonist DKK-142. Our findings give some support to the theory that anti-TNF treatment is associated with increased Wnt activity, but caution should be taken in the interpretation, because only 21% of the patients were treated with TNF-α blockers and the study was not designed to evaluate the effects of treatment.
Anti-TNF-α treatment has been shown to improve BMD in SpA in earlier studies43,44. In our study, anti-TNF treatment was associated with increased serum levels of sRANKL and lower levels of OPG. Studies on TNF inhibition and levels of sRANKL and OPG in rheumatoid arthritis (RA) have shown both unchanged or lowered levels of sRANKL and unchanged or decreased levels of OPG45.
We found the levels of serum sRANKL and the sRANKL/OPG ratio to be lower in patients with AS compared with the healthy controls. In contrast to our findings, 2 earlier studies with younger cohorts (mean age 32 and 34 yrs) of 60 and 42 patients showed higher levels of sRANKL in AS compared with controls, and in another investigation of 21 patients (mean age 51 yrs), no difference was shown46,47,48. Previous studies on serum RANKL in relation to osteoporosis in men and postmenopausal women have also yielded conflicting results49.
In our study, serum levels of OPG were positively correlated with BASMI and aging. The data are corroborated by an earlier study showing similar association between elevated levels of OPG and poorer spinal mobility and functional outcome47. Serum concentrations of OPG are increased in aging healthy women and men and in patients with osteoporosis50,51. This is viewed as a compensatory mechanism to prevent further bone loss. An earlier study on OPG in AS demonstrated a lack of age-related OPG increase in patients with AS, but this was not confirmed in 2 other studies including the present48,52. We found a negative correlation between OPG and BMD of the femoral neck. Diverging results regarding correlation between OPG and BMD have been reported before48,52.
Cigarette smoking has been identified as a risk factor for radiologic progression, impairment of back mobility, and functional outcome in AS and early axial SpA36,53,54. Our study supports the prior findings. We found that smoking was strongly associated with higher mSASSS, BASMI, age, and lower femoral neck BMD. In addition, high number of smoking pack-years was an independent covariate for mSASSS in the multivariate analyses after adjusting for age.
A limitation of our study was the cross-sectional design. A longitudinal study is needed to show whether the elevated levels of Wnt-3a just reflect presence of chronic AS related changes in the spine or whether Wnt-3a is a predictor for radiologic progression. The validity of the Wnt-3a analysis also needs to be confirmed in other cohorts of patients with AS and in early SpA. It would also be of interest to investigate the levels in other diseases, such as RA and osteoporosis, and to study other members of the Wnt family with respect to disease activity, osteoproliferation, and osteoporosis in AS. A strength of our study was that the biomarkers were studied both in relation to osteoproliferation and BMD, and to the best of our knowledge, was the first to do so.
We analyzed serum levels of biomarkers for bone metabolism in a cohort of 204 well-characterized patients with AS. Most importantly, we found that serum Wnt-3a was significantly higher in the patients with AS and positively correlated with mSASSS and BASMI. After adjusting for sex, age, smoking, and CRP using multiple linear regression, serum Wnt-3a remained independently associated with mSASSS and BASMI, indicating that Wnt-3a could be a marker for the osteoproliferative process in AS.
Acknowledgments
The authors thank all the patients and the blood donors who participated in the study.
Footnotes
-
Supported by grants from The Health and Medical Care Executive Board of the Västra Götaland, Rune and Ulla Amlövs foundation for Rheumatology Research, Göteborg’s Association Against Rheumatism, The Medical Society of Göteborg, the Medical Society of Göteborg and the Region Västra Götaland (agreement concerning research and education of doctors), COMBINE, the Margareta Rheuma research foundation, and the Inger Bendix foundation.
- Accepted for publication March 7, 2014.








{kind=link}