

Abstract
Objective. To evaluate the effects of golimumab therapy on achieving inactive disease or major improvement, as assessed by the Ankylosing Spondylitis Disease Activity Score (ASDAS), and improvements in health-related quality of life (HRQOL) and productivity through 2 years in patients with AS.
Methods. In the phase III GO-RAISE trial, 356 patients were randomized to placebo with crossover to golimumab 50 mg at Week 24 (n = 78), golimumab 50 mg (n = 138), or golimumab 100 mg (n = 140) at baseline and every 4 weeks. The proportions of patients with ASDAS major improvement (improvement ≥ 2.0) or inactive disease (score < 1.3) were determined. HRQOL was assessed using the 36-item Medical Outcomes Study Short Form-36 physical/mental component summary (SF-36 PCS/MCS) scores (normal score ≥ 50). The effect of disease on productivity was assessed by visual analog scale (0–10). Regression analyses on the association of disease activity and HRQOL were performed. The final assessment was at Week 104.
Results. Significantly greater proportions of golimumab-treated patients achieved ASDAS major improvement or inactive disease at weeks 14 and 24 versus placebo. Through Week 104, patients who achieved ASDAS inactive disease or major improvement had significantly greater improvements in SF-36 PCS and MCS scores and productivity than did patients not meeting these targets. Among all patients, achieving ASDAS inactive disease at weeks 52 and 104 was associated with normalized SF-36 PCS/MCS scores and significant improvements in work productivity.
Conclusion. Greater proportions of golimumab-treated patients achieved ASDAS major improvement or inactive disease and improved HRQOL versus placebo. Achieving an inactive disease state by ASDAS criteria (< 1.3) was associated with normalized HRQOL through 2 years.
Ankylosing spondylitis (AS) is a chronic inflammatory disease, primarily affecting the spine and sacroiliac joints. Uncontrolled systemic inflammation in patients with AS is thought to precipitate extraarticular manifestations, including eye, skin, bone, and bowel disease1. AS typically presents in the third decade of life, thus disrupting patients’ work productivity2,3,4,5 and quality of life6,7,8 during their prime working years. Treatment with therapies targeting tumor necrosis factor (TNF) has been shown to improve health-related quality of life (HRQOL) in patients with AS9,10,11.
Disease activity in patients with AS has typically been evaluated with a variety of assessments that separately measure the patient’s assessment of disease, the physician’s assessment of disease, acute-phase reactants, and joint changes visible by MRI12. The composite Bath AS Disease Activity Index13 is a commonly used activity measure in clinical trials; however, it is limited to only patient-reported outcomes. The Bath AS Functional Index is a validated measure for assessing physical function in patients with AS. A 20% improvement in the Assessment of SpondyloArthritis international Society (ASAS)14 criteria is also a commonly used endpoint in clinical trials, but it relies on measuring a change from a reference baseline status and cannot be used to determine disease state at a given timepoint. The ASAS 5/6 improvement criteria includes C-reactive protein (CRP) and performs well in anti-TNF trials, but like the ASAS20 response15, it is limited to measuring improvements over time. Recently, ASAS has developed a well-balanced AS Disease Activity Score (ASDAS) that incorporates both patient-reported outcomes and either CRP or erythrocyte sedimentation rate (ESR)16. The validated ASDAS can be used to assess disease activity as a continuous measure or as discrete levels as well as measuring improvement following treatment17.
In the GO-RAISE trial, the safety and efficacy of golimumab, a human monoclonal anti-TNF antibody, was evaluated in adult patients with active AS. Patients treated with golimumab 50 mg or 100 mg had significantly greater improvements in the signs and symptoms of AS and HRQOL compared with those who received placebo18, and response to golimumab treatment was maintained for up to 2 years as reported19. In a limited posthoc analysis using the ASDAS, significantly greater proportions of patients treated with golimumab 50 mg or 100 mg had an ASDAS < 1.1 or < 2.1 at Week 24 when compared with those who received placebo; response rates were generally similar among treatment groups at weeks 52 and 104, after placebo patients had been receiving golimumab for several months19. We now report the findings of additional posthoc analyses of the GO-RAISE trial evaluating ASDAS inactive disease and major clinical response and the association of these outcomes with changes in HRQOL and the effect of disease on productivity.
MATERIALS AND METHODS
Patients and study design
The detailed patient eligibility criteria and study design of the GO-RAISE trial have been reported18. Briefly, adult patients with active AS were randomly assigned to receive subcutaneous injections of placebo (Group 1), golimumab 50 mg (Group 2), or golimumab 100 mg (Group 3) at baseline and every 4 weeks. At Week 16, patients who had < 20% improvement in total back pain and morning stiffness entered blinded early escape, such that patients in Group 1 switched to golimumab 50 mg injections, and patients in Group 2 had their golimumab dose increased from 50 mg to 100 mg. No treatment adjustments were permitted for patients in Group 3 regardless of their early escape status. At Week 24, all patients who were still receiving placebo crossed over to golimumab 50 mg. No additional changes in treatment were permitted after Week 24, and all golimumab injections continued to be administered every 4 weeks through Week 100; the final visit included in our analysis was at Week 104.
The protocol was approved by the institutional review board or ethics committee at each site. All patients gave written informed consent before any study-related procedures were performed.
Assessments
In this posthoc analysis, disease activity was evaluated using the composite ASDAS, which was developed after the GO-RAISE trial was initiated. The ASDAS incorporates measures of back pain, duration of morning stiffness, patient global assessment, peripheral pain/swelling, and CRP17,20. There is no upper limit to the ASDAS, and a higher score indicates more severe disease17, with the following cutpoints indicating different levels of disease activity: < 1.3 = inactive disease, 1.3 to < 2.1 = moderate disease, 2.1 to 3.5 = high disease activity, and > 3.5 = very active disease20. ASDAS major improvement was defined as an improvement ≥ 2.0 from baseline20.
Patient HRQOL was assessed using the physical component summary (PCS) and mental component summary (MCS) scores of the 36-item Medical Outcomes Study Short Form-36 (SF-36)21. The effect of disease on productivity at work, school, or home was evaluated using a visual analog scale (VAS, 0–10 cm). Employability was self-reported and defined as currently working or able to work if a job is available.
Statistical analysis
Descriptive statistics are reported by randomized treatment group. ASDAS scores were assessed at weeks 0, 14, 24, 52, and 104; the proportions of patients in each treatment group achieving ASDAS major improvement or inactive disease were also determined through Week 104. Mean changes from baseline in SF-36 PCS and MCS scores, and the proportions of patients with normal PCS and MCS scores (≥ 50) or a minimal clinically important difference (MCID; improvement ≥ 5 units) were determined at weeks 14, 24, 52, and 104. Improvements from baseline in the effect of disease on productivity were determined at weeks 16, 24, 52, and 104; employment status for patients who were unemployable at baseline because of AS was assessed at weeks 24, 52, and 104. Through Week 24, differences between Group 1 and Groups 2 and 3 were evaluated using an ANOVA on the van der Waerden normal scores for continuous variables and chi-square test for dichotomous variables. Statistical comparisons among the treatment groups were not performed beyond Week 24 because all patients were receiving golimumab.
For patients in Group 1 and Group 2 who met the early escape criteria at Week 16, Week 16 values were carried forward to Week 24; however, if the Week 16 value was missing, the values at Week 24 were set to missing. Mean improvements in SF-36 PCS and MCS scores and the proportions of patients with normal PCS and MCS scores were compared between patients with ASDAS major improvement or inactive disease and those who were nonresponders. Relative risks (RR) for achieving normal SF-36 PCS and MCS scores among patients who achieved ASDAS inactive disease were estimated using log-binomial regression models that adjusted for treatment group and age (both PCS and MCS analyses), as well as baseline SF-36 MCS score (MCS analysis only).
RESULTS
Baseline characteristics
A total of 356 patients were randomly assigned to Group 1 (placebo, n = 78), Group 2 (golimumab 50 mg, n = 138), or Group 3 (golimumab 100 mg, n = 140). Demographic and baseline disease characteristics were generally well-balanced among the treatment groups and have been detailed previously18. The population was predominantly male and exhibited significant disease activity at baseline (Table 1). The physical effect of AS on patients’ HRQOL was evident in the SF-36 PCS scores (means: 29.2–30.7 across treatment groups).
Baseline demographic and disease characteristics. Data are presented as mean (SD) unless otherwise noted.
Clinical response
Mean ASDAS scores were similar across the treatment groups at baseline (Table 1). During the 24-week placebo-controlled period, improvements in ASDAS were significantly greater in Groups 2 and 3 than in Group 1 at both weeks 14 and 24 (Table 2). Significantly greater proportions of patients in Groups 2 and 3 achieved ASDAS major improvement when compared with Group 1 at both Week 14 (37.0% and 38.5% vs 5.1%; p < 0.001) and Week 24 (39.4% and 39.0% vs 4.2%; p < 0.001; Figure 1). Likewise, significantly greater proportions of patients in Groups 2 and 3 had ASDAS inactive disease at weeks 14 and 24 (Figure 1). Following placebo crossover to golimumab 50 mg at Week 16 (early escape) or 24 (crossover), mean improvements from baseline in ASDAS scores at weeks 52 and 104 were similar across all 3 treatment groups (Table 2).

Proportions of patients with ASDAS major improvement (A) or inactive disease (B) at weeks 14 and 24. *p < 0.001. ASDAS: Ankylosing Spondylitis Disease Activity Score.
Improvements in ASDAS, health-related quality of life, and productivity through Week 104a. Data presented as n (%) or mean ± SD.
HRQOL and productivity
Previously, median improvements in SF-36 PCS and MCS scores in the randomized treatment groups through Week 24 and mean improvements at weeks 52, 76, and 104 with patients classified according to early escape status were reported18,19. Here we report mean improvements in SF-36 PCS and MCS scores by randomized treatment group (Table 2). Consistent with earlier reports, patients in Groups 2 and 3 had greater mean improvements in SF-36 PCS and MCS scores at weeks 14 and 24 than did patients in Group 1, and mean improvements at weeks 52 and 104 were similar among the treatment groups (Table 2). Additionally, the proportions of patients who achieved a normal SF-36 PCS score (≥ 50) or an MCID in SF-36 PCS were significantly greater in Groups 2 and 3 than in Group 1 at weeks 14 and 24 (Table 2). The proportions of patients with a normal MCS score at weeks 14 and 24 were not significantly different among the treatment groups, ranging from 46.2% to 48.9% and from 49.3% to 52.6%, respectively. At weeks 52 and 104, when all patients had been receiving golimumab for several months, the proportions of patients with normal SF-36 PCS or MCS scores or with an MCID in score were similar among all treatment groups (Table 2).
Mean improvements in the effect of disease on productivity were significantly greater in Groups 2 and 3 than in Group 1 at weeks 16 and 24 (Table 2). Improvements in productivity were similar among the treatment groups at weeks 52 and 104 and ranged from 3.4 to 3.7 and from 3.8 to 4.1, respectively. Among patients who reported that they were unemployable at baseline and had not retired before Week 24, 34.3% (12/35) of those in Groups 2 and 3 combined and 20.0% (2/10) in Group 1 regained employability at Week 24; however, this numerical difference was not statistically significant. At weeks 52 and 104, 17/36 (47.2%) and 19/28 (67.9%) of patients, respectively, who were unemployable at baseline because of AS had regained employability.
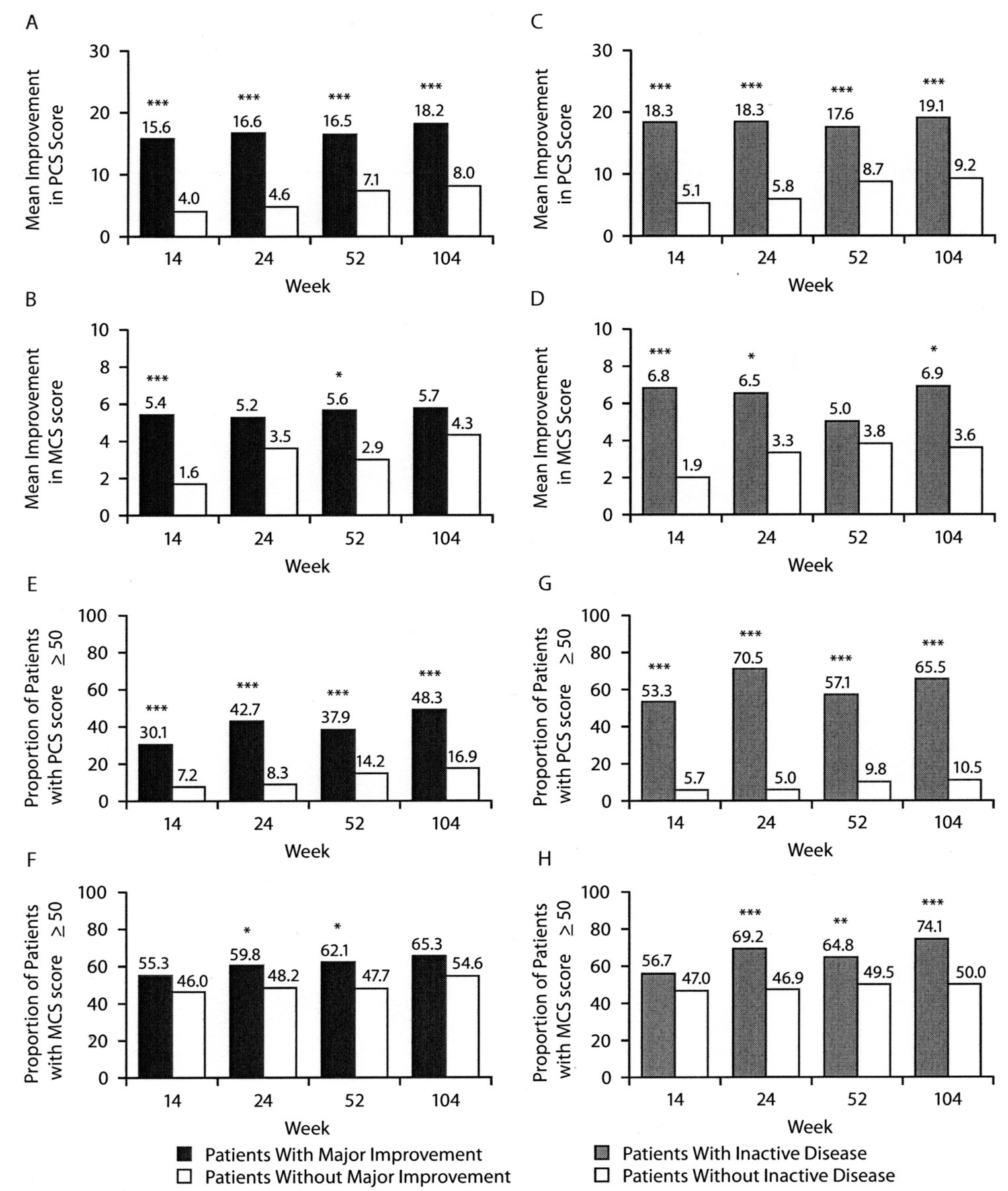
Among all patients, those who had ASDAS major improvement or inactive disease at weeks 14, 24, 52, and 104 had significantly greater mean improvements in SF-36 PCS scores than did patients who were nonresponders (Figure 2A–D). ASDAS responders also had greater improvements in SF-36 MCS scores, although these differences were not always statistically significant (Figure 2A–D). In addition, greater proportions of patients with ASDAS major improvement or inactive disease had normal SF-36 PCS scores (≥ 50) when compared with nonresponders (Figure 2E–H). Overall, greater proportions of ASDAS responders versus nonresponders had normal SF-36 MCS scores (≥ 50); however, this difference was not always statistically significant (Figure 2E–H). Regression analyses showed that achieving ASDAS inactive disease at weeks 52 and 104 was significantly associated with having a normal SF-36 PCS score at weeks 52 and 104 and a normal SF-36 MCS score at Week 104 (Table 3).
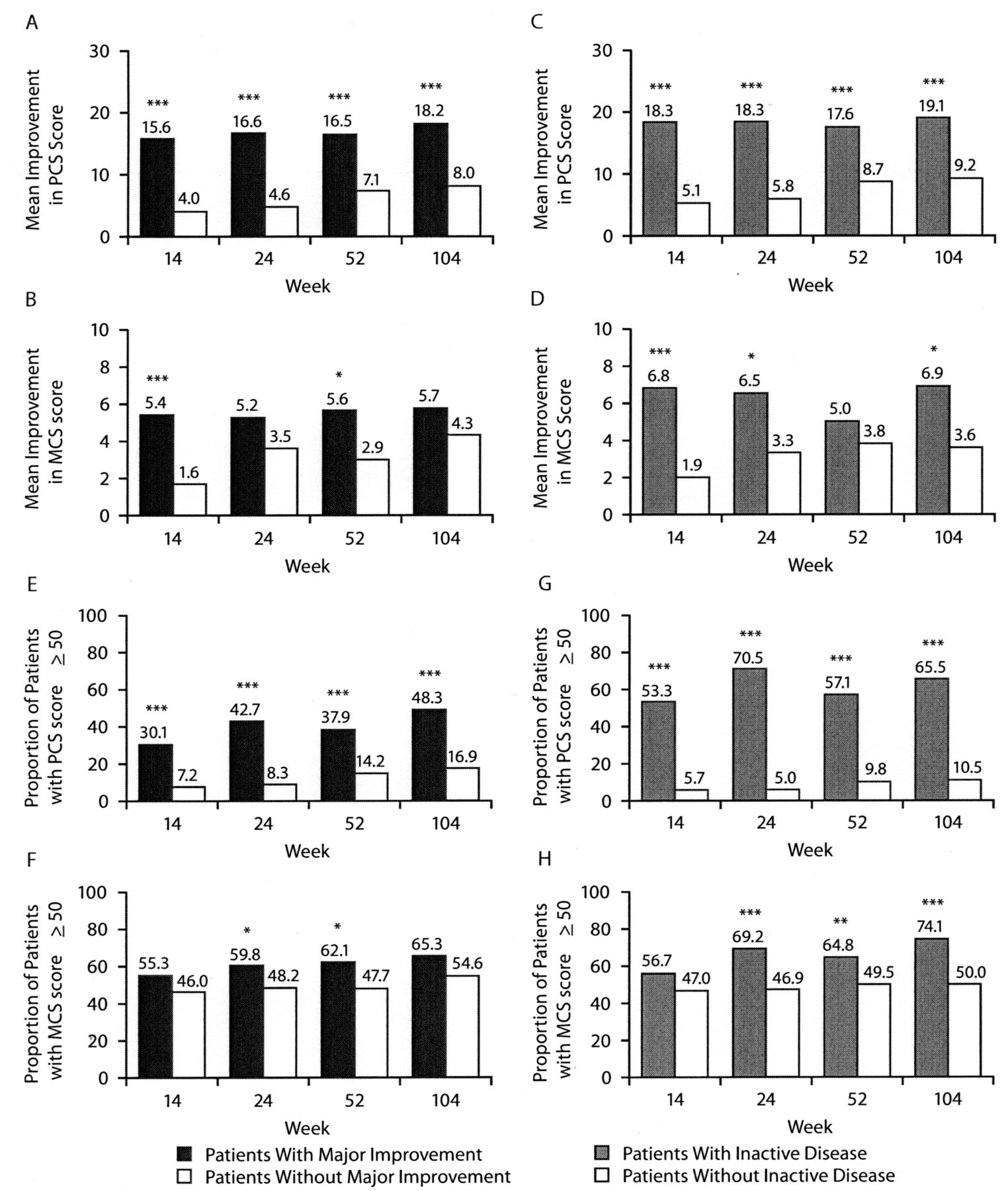
Mean improvements in SF-36 PCS and MCS scores (A–D) and the proportions of patients who achieved a normal SF-36 PCS and MCS score (≥ 50; E–H) among patients who achieved ASDAS major improvement or inactive disease. All patients who were randomized to placebo switched to golimumab at Week 16 (early escape) or Week 24 (prespecified crossover). *p < 0.05, ** p < 0.01, *** p < 0.001. ASDAS: Ankylosing Spondylitis Disease Activity Score; SF-36 PCS/MCS: 36-item Medical Outcomes Study Short Form-36 physical/mental component summary.
Relative risk for achieving normal SF-36 PCS and MCS scores among patients who achieved ASDAS inactive disease at weeks 52 and 104a.
Patients with ASDAS major improvement or inactive disease had a significantly greater median percent improvement in productivity than did nonresponders at weeks 16, 24, 52, and 104 (Figure 3). Among patients who were unemployable at baseline owing to AS and had ASDAS data available, 15 achieved ASDAS major improvement at Week 52, and 11 of these patients (73.3%) regained employability. In addition, 7 patients who were unemployable at baseline achieved ASDAS inactive disease at Week 52, and 6 of these patients (85.7%) regained employability. At Week 104, 13 of the 14 (92.9%) patients who had major improvement regained employability, and all 7 patients who achieved inactive disease regained employability.
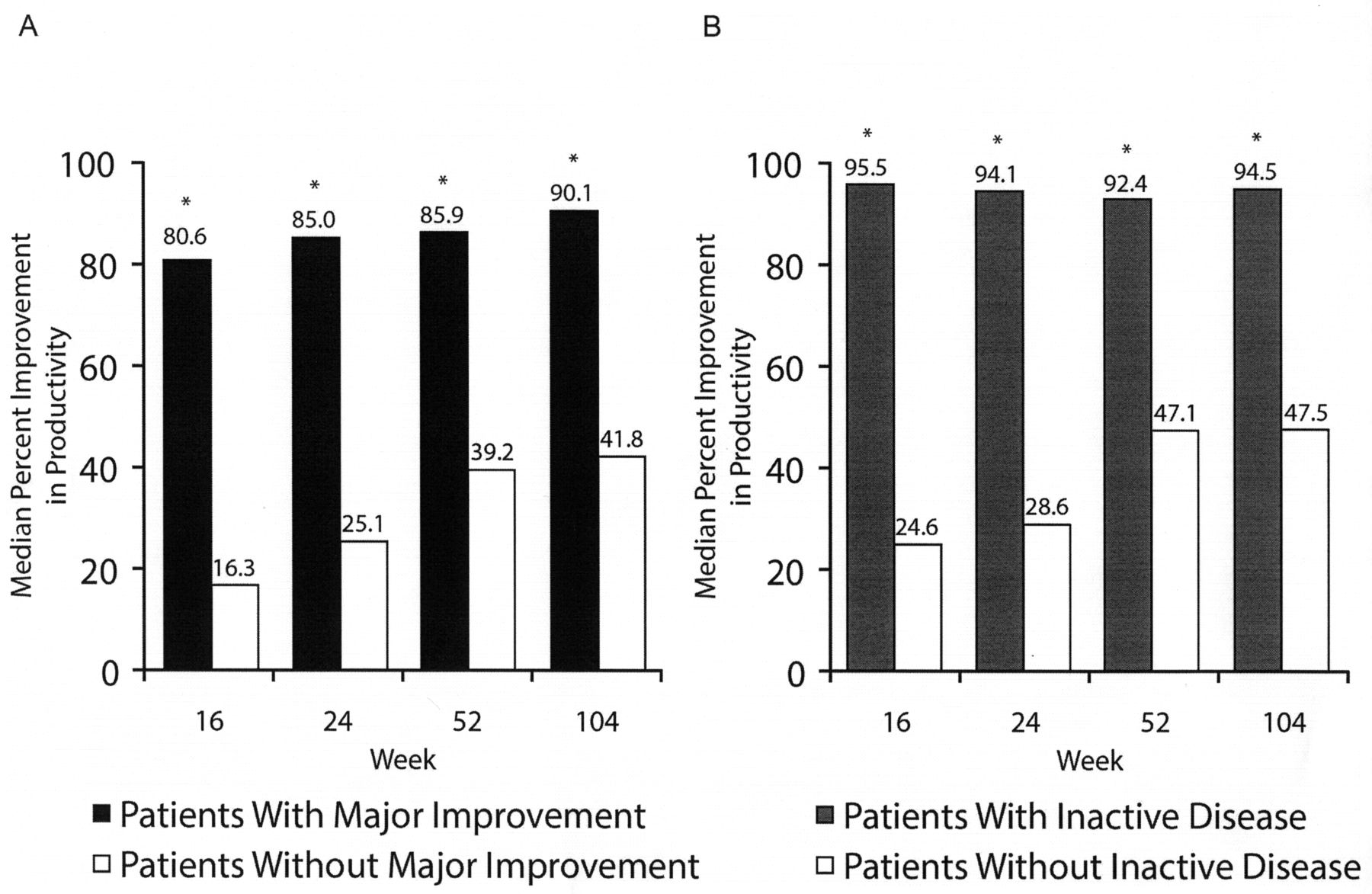
Median percent improvement in productivity among patients who achieved ASDAS major improvement (A) or inactive disease (B). All patients who were randomized to placebo switched to golimumab at Week 16 (early escape) or Week 24 (prespecified crossover). * p < 0.001. ASDAS: Ankylosing Spondylitis Disease Activity Score.
DISCUSSION
Historically, disease activity in AS has been measured using a combination of tools that separately evaluated the patient’s assessment of disease, the physician’s assessment of disease, and acute-phase reactants. Many of these tools are limited to 1 aspect of disease activity or allow for only the physician’s or the patient’s assessment. The ASAS20 response, a commonly used study endpoint, is useful in determining improvement from baseline in signs and symptoms, but cannot measure absolute disease activity at a given timepoint and does not include an objective measure of disease activity14,15.
The ASDAS is the first disease activity index for AS that includes both patient-reported outcomes and acute-phase reactants, which physicians may emphasize over subjective measures22. It has been shown to correlate well with both the patient and physician global assessments17. The burden to patients and physicians is low in that it is easy to administer and calculate23. While the ASDAS is the newest disease activity measure for AS, analyses have shown that this index reliably discriminates between disease states and is sensitive to changes in disease activity following treatment17.
In a previous report of the primary 2-year findings of the GO-RAISE trial, golimumab was shown to be effective in reducing the signs and symptoms of AS in adult patients through 2 years of treatment19. Limited ASDAS results (proportions of patients with ASDAS < 1.1 or < 2.1) were reported in the previous analysis19 and are consistent with the findings of the more detailed ASDAS analysis presented here. In the current analysis, patients treated with golimumab 50 mg and 100 mg had significantly greater improvements in ASDAS scores than did patients who received placebo, and significantly greater proportions of golimumab-treated patients achieved ASDAS major improvement (improvement ≥ 2.0) or inactive disease (score < 1.3) at weeks 14 and 24 when compared with those who received placebo.
Improvements in HRQOL and health economic measures were similar for the 2 golimumab doses studied (50 mg and 100 mg) and were consistent with improvements seen with other anti-TNF agents24,25,26. Consistent with earlier reports of the GO-RAISE trial18,19, golimumab-treated patients had significantly greater mean improvements in SF-36 PCS scores through Week 24; mean improvements in SF-36 MCS scores were not as pronounced, likely owing to the near-normal mean MCS scores at baseline. Greater proportions of golimumab-treated patients achieved normal HRQOL (SF-36 PCS/MCS scores) or a clinically significant improvement in HRQOL when compared with those who received placebo. Through Week 24, golimumab-treated patients had significantly greater improvements in productivity versus placebo. In addition, a trend toward greater employability at Week 24 was observed.
In general, patients who achieved ASDAS major improvement or inactive disease had significantly greater improvements in HRQOL through Week 104 than did ASDAS nonresponders. Further, achievement of ASDAS inactive disease was significantly associated with normal HRQOL. It should be noted that instead of using OR, we calculated RR, which are more appropriate in this situation but often yield lower values27. ASDAS responders (major improvement or inactive disease) also experienced greater improvements in the effect of disease on productivity and were more likely to have an improvement in their employability status compared with nonresponders.
Recently, efforts have been made to define treatment targets for patients with spondyloarthritis, including AS, with the recommendation that, whenever possible, inactive disease should be a major treatment target for patients with AS28. In our analysis of the GO-RAISE trial, patients who achieved ASDAS inactive disease appeared to have greater improvements in HRQOL outcomes than did patients who achieved ASDAS major improvement, although statistical comparisons were not performed. These results together with the association of inactive disease with normalized HRQOL support the recommendation of inactive disease as a treatment target in AS28.
It should be noted that the ASDAS can be calculated using either CRP or ESR; however, the ASDAS using CRP is the preferred method given that CRP measurements can be accurately performed with stored serum samples and using standardized assays in a central laboratory17. ESR can be used as an alternative when CRP levels are not available, but it is not recommended to use the resulting scores interchangeably in the same analysis or for the same patient17. ESR measurements were not collected during the GO-RAISE study; therefore, we could not evaluate the performance of ASDAS using ESR with regards to HRQOL and employment outcomes.
This analysis of the GO-RAISE trial is primarily limited by the posthoc nature of our study. The determination of ASDAS results was not prespecified in the protocol because the ASDAS did not exist when the trial began, and the GO-RAISE trial was not specifically designed to evaluate the relationship between HRQOL and health economic outcomes with changes in ASDAS scores.
Previous analyses have demonstrated that the ASDAS can discriminate between AS disease activity states as well as or better than existing measures17. In the current analysis, patients who achieved ASDAS major improvement or inactive disease consistently had greater improvements in SF-36 PCS and MCS scores and productivity when compared with those who did not achieve major improvement or inactive disease. Also, achievement of ASDAS inactive disease was significantly associated with normalized SF-36 PCS and MCS scores, which supports the recent recommendation that achieving inactive disease should be a major treatment goal in patients with AS28. These findings indicate that, in addition to discriminating clinical disease activity, ASDAS response is consistent with improvements in various HRQOL and health economic outcomes.
Acknowledgment
The authors thank Rebecca E. Clemente, PhD, and Mary Whitman, PhD, of Janssen Biotech Services LLC for writing and editorial support.
Footnotes
-
Supported by Janssen Research & Development LLC and Merck/Schering-Plough. Authors MM, BH, TAG, and CH are employees of the study sponsor and own stock in Johnson & Johnson, of which Janssen Research & Development LLC and Janssen Global Services LLC are subsidiaries. DvdH has received consulting fees and/or research grants from AbbVie, Amgen, AstraZeneca, Augurex, BMS, Celgene, Chugai, Covagen, Daiichi, Eli-Lilly, GSK, Janssen Biologics, Merck, Novartis, Novo-Nordisk, Otsuka, Pfizer, Roche, Sanofi-Aventis, Schering-Plough, UCB, and Vertex and is director of imaging at Rheumatology bv. AD has received payments for educational lectures, teleconferences and serving on advisory boards for Janssen, a company that may have a commercial interest in the results of this research. JB has received honoraria for talks, advisory boards, and grants for studies from Janssen Research & Development LLC, Amgen, Abbott, BMS, Celltrion, Novartis, Pfizer (Wyeth), MSD (Schering-Plough), Roche, Sanofi-Aventis, and UCB. RDI has received consulting fees from Merck, Schering-Plough, Abbott, Amgen, and Sanofi-Aventis.
- Accepted for publication February 12, 2014.








{kind=link}
{kind=link}
{kind=link}