

Abstract
Objective. To perform a systematic review of the benefits and harms of folic acid and folinic acid in reducing the mucosal, gastrointestinal, hepatic, and hematologic side effects of methotrexate (MTX); and to assess whether folic or folinic acid supplementation has any effect on MTX benefit.
Methods. We searched the Cochrane Library, MEDLINE, EMBASE, and US National Institutes of Health clinical trials registry from inception to March 2012. We selected all double-blind, randomized, placebo-controlled clinical trials in which adult patients with rheumatoid arthritis (RA) were treated with MTX (dose ≤ 25 mg/week) concurrently with folate supplementation. We included only trials using low-dose folic or folinic acid (a starting dose of ≤ 7 mg weekly) because the high dose is no longer recommended or used. Data were extracted from the trials, and the trials were independently assessed for risk of bias using a predetermined set of criteria.
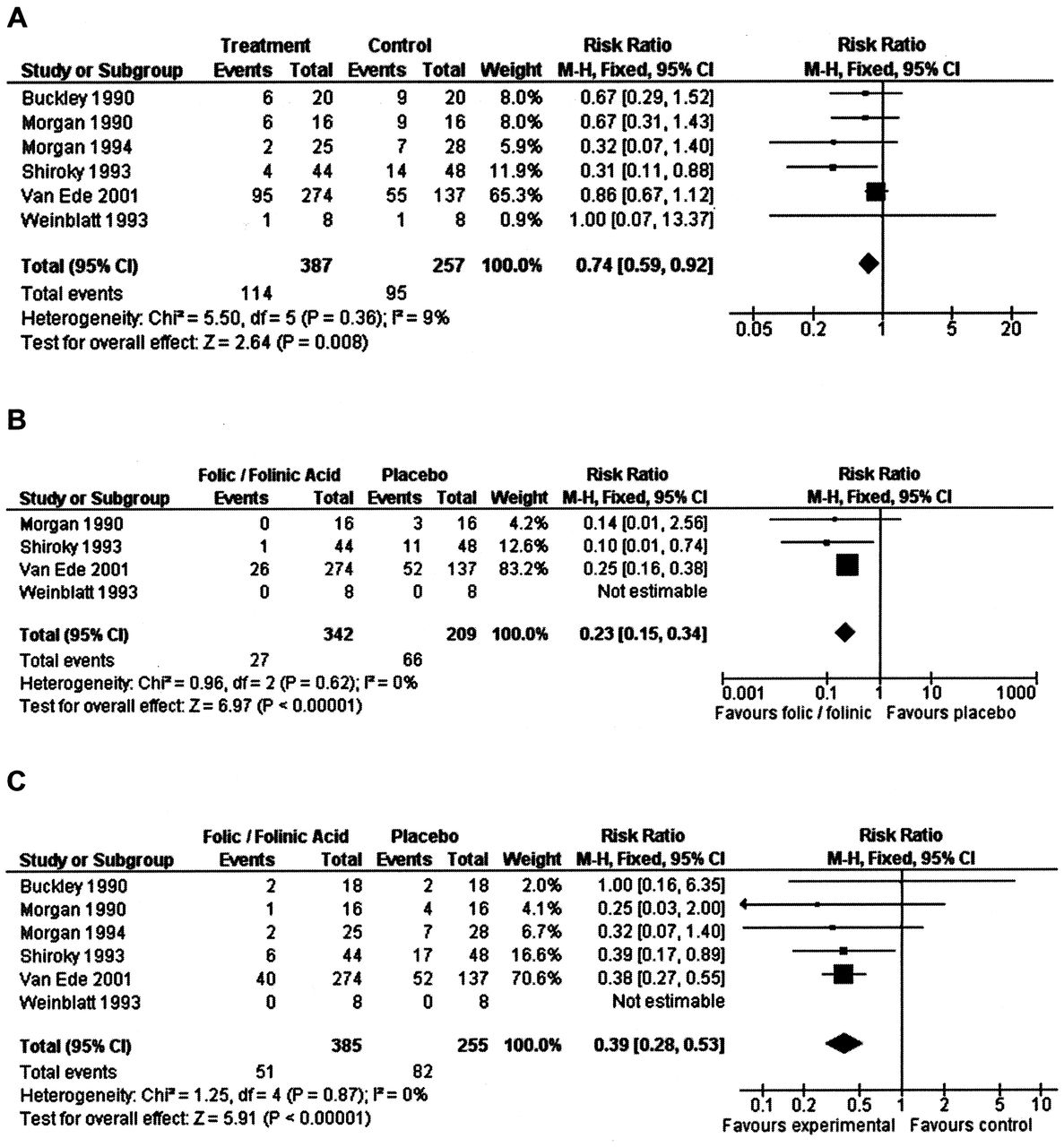
Results. Six trials with 624 patients were eligible for inclusion. Most studies had low or unclear risk of bias for key domains. The quality of the evidence was rated as “moderate” for each outcome as assessed by the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) working group, with the exception of hematologic side effects, which were rated as “low.” There was no significant heterogeneity between trials, including where folic acid and folinic acid studies were pooled. For patients supplemented with any form of exogenous folate (either folic or folinic acid) while receiving MTX therapy for RA, a 26% relative (9% absolute) risk reduction was seen for the incidence of gastrointestinal side effects such as nausea, vomiting, or abdominal pain (RR 0.74, 95% CI 0.59 to 0.92; p = 0.008). Folic and folinic acid also appear to be protective against abnormal serum transaminase elevation caused by MTX, with a 76.9% relative (16% absolute) risk reduction (RR 0.23, 95% CI 0.15 to 0.34; p < 0.00001), as well as reducing patient withdrawal from MTX for any reason [60.8% relative (15.2% absolute) risk reduction, RR 0.39, 95% CI 0.28 to 0.53; p < 0.00001].
Conclusion. The results support a protective effect of supplementation with either folic or folinic acid for patients with RA during treatment with MTX. There was a clinically important significant reduction shown in the incidence of GI side effects and hepatic dysfunction (as measured by elevated serum transaminase levels), as well as a clinically important significant reduction in discontinuation of MTX treatment for any reason.
Methotrexate (MTX) is an antimetabolite with an antagonistic effect on folic acid metabolism. Although its exact mechanism of action in rheumatoid arthritis (RA) is uncertain, it has become the first-line drug of choice1.
Three metaanalyses2,3,4 estimate that a third of the patients show major improvement. However, toxicity does prevent many patients from obtaining benefit from the drug. It has been reported that mild toxicity occurs in about 60% of patients, and roughly 7% to 30% of patients discontinue MTX therapy within the first year of treatment because of toxicity1,5.
Folic acid (also known as vitamin B9) has demonstrated health benefits in a variety of areas. Folinic acid (5-formyl tetrahydrofolate) is one active form in the group of vitamins known as folates. In contrast to folic acid (which is a synthetic form of folate), folinic acid is found naturally in foods. In the body, folinic acid can be converted into any of the other active forms of folate.
Folate deficiency occurs frequently in patients with RA, and folate stores are further decreased in patients with RA who receive MTX6. Gastrointestinal (GI) and hematologic side effects have been related to folate deficiency. There has been concern that high doses of folate supplementation may reduce the efficacy of, and therefore benefit seen with, MTX if the antirheumatic effects are also mediated through folate antagonism7,8,9. The aim of this systematic review was to determine the effect of low doses of folic acid and folinic acid in reducing GI symptoms, hepatic (liver) toxicity, and hematologic side effects of low-dose MTX in patients with RA, and to determine whether folate supplementation with folic acid or folinic acid reduces the anti-arthritis benefit of MTX therapy.
MATERIALS AND METHODS
Types of studies, participants, and interventions
We included all double-blind, randomized, placebo-controlled clinical trials comparing low doses of MTX (≤ 25 mg/week) concurrently with low-dose folate supplementation (either folic or folinic acid), with a starting dose ≤ 7 mg/week in patients older than 18 years, fulfilling the American College of Rheumatology criteria for RA10.
Outcome measures
Major outcomes included GI symptoms (such as nausea, vomiting, or abdominal pain), mouth ulcers (stomatitis), liver toxicity (as measured by raised serum transaminases), hematologic side effects (anemia or cytopenia), and discontinuation of MTX therapy. Minor outcomes included alteration of the beneficial effect of MTX (loss of efficacy) as measured by any of the following: swollen joint count (SJC), tender joint count (TJC), pain, disability score, grip strength, patient global assessment, and physician global assessment.
Search methods for identification of studies
We searched the following electronic databases, unrestricted by language: Cochrane Library Issue 2 of 12, February 2012 (by Wiley), MEDLINE (through OVID 1946–March 2, 2012), and EMBASE (through OVID 1947–February Week 4, 2012). Reports of ongoing trials were searched in the US National Institutes of Health trial registry, ClinicalTrials.Gov (www.clincaltrials.gov). Reference lists from related publications and abstracts of selected rheumatology meetings were scanned for possible inclusion.
The MEDLINE search strategy combined the subject search with the Cochrane highly sensitive search strategy for identifying reports of randomized controlled trials (RCT)11, and was adapted for the other databases. Full search strategies are available on request.
Following an a priori protocol, at least 2 review authors (BS, ZO, WK, MS, TR) independently screened all titles or abstracts generated by the searches for potentially relevant studies. We assessed the full-length articles of the selected titles or abstracts for eligibility. We resolved disagreements by consensus or third-party adjudication.
Data extraction and management
Data were independently extracted by 4 authors (ZO, BS, WK, MS). Folate supplementation was considered as “the administration of folic or folinic acid at any time with respect to MTX.” The GI effects were combined (where possible). The incidence of stomatitis, as well as the incidence of abnormal serum liver enzymes, was analyzed independently. The following hematologic side effects were included, if reported: cytopenia, macrocytosis, or pancytopenia.
To assess changes in disease activity, the following measurements were considered a priori and ultimately included in the efficacy analysis: SJC, TJC, pain, disability score, grip strength, patient global assessment, and physician global assessment. A starting dose of ≤ 7 mg/wk folic or folinic acid was used as a cutoff value for studies to be included in the analysis. Worldwide guidelines currently support co-administration of folic acid with MTX, and where a dose value is suggested, it usually falls in the range of 0.5 to 2 mg daily12,13,14,15.
Assessment of risk of bias (ROB) in included studies
Assessment of ROB was undertaken for each included study using the Cochrane Collaboration’s ROB tool16. The following 7 key domains were assessed: sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective outcome reporting, and “other issues” (comparability of treatment and control group at entry, and appropriateness of duration of surveillance). Pairs of review authors judged the key domains as either “high risk,” “low risk,” or “unclear” ROB. In cases of disagreement, the decision was made by consensus.
Statistical analysis
For each trial, risk ratio (RR) and the 95% CI were calculated for dichotomous outcomes. Mean differences and 95% CI were calculated for continuous outcomes. If the scale for each assessment varied among the studies, we calculated a standardized mean difference based on end-of-trial results. If the SD of the change scores were not available we used the SD of the baseline score for each group. If we noticed missing data during data extraction, we attempted to contact the original investigators of the study to request the required information.
Heterogeneity between comparable trials was tested using a standard chi-square test and considered statistically significant at p < 0.10; after due consideration of the value of the I2 statistic, a value > 50% may indicate substantial heterogeneity. If there were sufficient studies (at least 10) it was intended to assess the possibility of publication bias with funnel plots.
Data synthesis
Where appropriate, results of comparable groups of trials were pooled using the fixed-effect model, and 95% CI were calculated. If heterogeneity existed between studies, a random-effects model was used. Since folic and folinic acid do not act at the same point on the folate pathway, they were analyzed separately as well as together. Metaanalysis was facilitated by RevMan 5 software.
Grading of evidence and summary of findings tables
Major outcomes (including benefits and adverse events) were presented in summary of findings tables, which provide information on the quality of evidence and the magnitude of the intervention effect, as well as a summary of the main outcome data17. The Grading of Recommendations Assessment, Development, and Evaluation (GRADE) working group approach was used to assess the quality of evidence per outcome (high, moderate, low, and very low) as outlined in the Cochrane Handbook for Systematic Reviews of Interventions18.
RESULTS
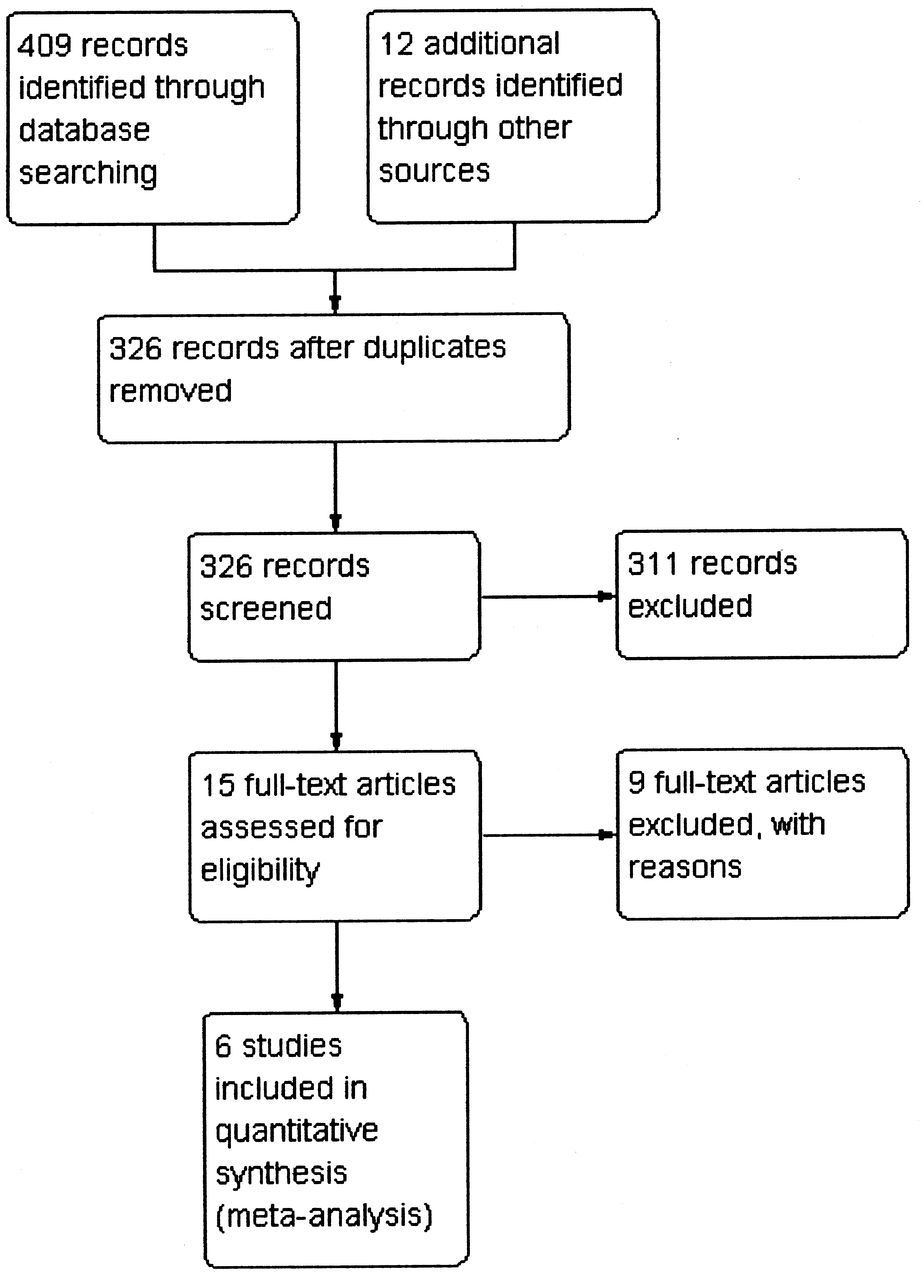
We initially screened 421 references, from which 15 papers in total were selected for full text appraisal. Six RCT19,20,21,22,23,24 met the eligibility criteria (Figure 1). The other 9 (2 abstracts and 7 articles) were excluded. All RCT included in the analysis assessed hematologic side effects with a complete blood count including platelet count. Some trials also measured mean corpuscular volume. Three of 6 included trials did not report number of patients with hematologic side effects, mean values, or measures of variance and could not be included in the analysis. Overall, the included trials reported 624 participants, of whom 385 were treated with either folinic (211 participants) or folic acid (174 participants). The study flow diagram is given in Figure 2 and characteristics of included studies in Table 1.

Methodological quality summary of included studies. +: low risk of bias; –: high risk of bias; ?: unclear risk of bias.

Study flow diagram.
Characteristics of included studies of patients with rheumatoid arthritis for more than 18 years.
Effects of interventions
There was no evidence of heterogeneity between included trials. The results from the random-effects model were not substantively different from the fixed-effect model.
Folic acid versus placebo
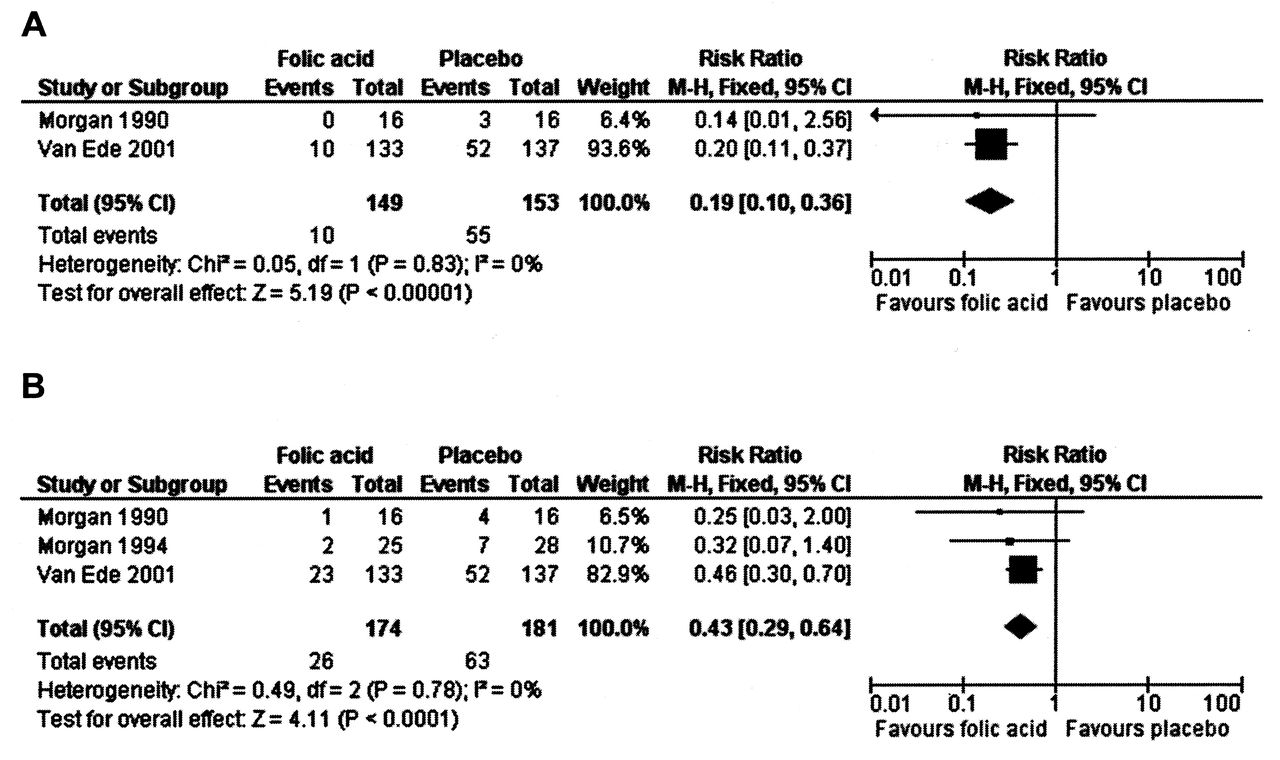
An 81% relative (16.8% absolute) reduction in risk was observed for the incidence of abnormal serum transaminase levels (RR 0.19, 95% CI 0.10 to 0.36; p ≤ 0.00001), and there was a statistically significant decrease in the number of people who dropped out of the studies for any reason while taking folic acid (−14.2% absolute difference; RR 0.43, 95% CI 0.29 to 0.64; p ≤ 0.0001). A 24% relative (8.1% absolute) reduction was seen for the risk of developing GI side effects such as nausea, vomiting, or abdominal pain, although this failed to reach statistical significance. A trend toward a reduction in the incidence of stomatitis (mouth sores) was seen; however, this also failed to reach statistical significance. Table 2 provides a detailed summary of findings, including the quality of evidence. Figures 3A and 3B show the pooled data based on liver toxicity and total withdrawals when taking folic acid as compared to placebo.
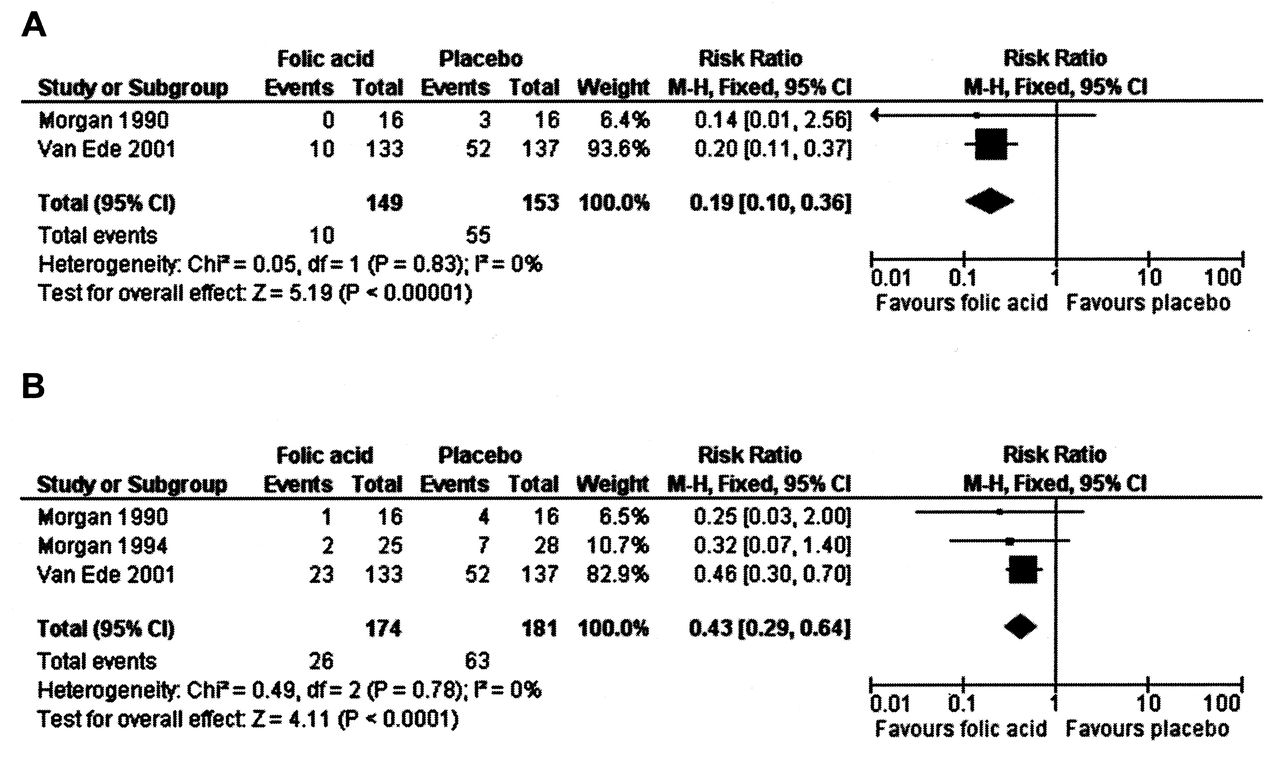
A. Liver toxicity (folic acid vs placebo). B. Total withdrawals (folic acid vs placebo).
Summary of findings: folic acid compared to placebo for reducing side effects in patients receiving methotrexate (MTX) for rheumatoid arthritis.
Folinic acid versus placebo
A 73% relative (15.2% absolute) reduction in risk was observed for the incidence of abnormal serum transaminase levels (RR 0.27, 95% CI 0.16 to 0.44; p ≤ 0.00001), and there was a statistically significant decrease in the number of people who dropped out of the studies for any reason while taking folinic acid (−16.2% absolute difference; RR 0.35, 95% CI 0.23 to 0.53; p ≤ 0.00001). A 22% relative (7.6% absolute) reduction was seen for the risk of developing GI side effects such as nausea, vomiting, or abdominal pain. Similarly, a trend toward a reduction in the incidence of stomatitis (mouth sores) was seen. However, both failed to reach statistical significance. It was not possible to draw meaningful conclusions on the effect of folic or folinic acid on hematologic side effects of MTX because of the small numbers of events and poor reporting of this outcome in included trials. Table 3 provides a detailed summary of findings, including the quality of evidence. Figures 4A and 4B show the pooled data based on liver toxicity and total withdrawals when taking folinic acid as compared to placebo.
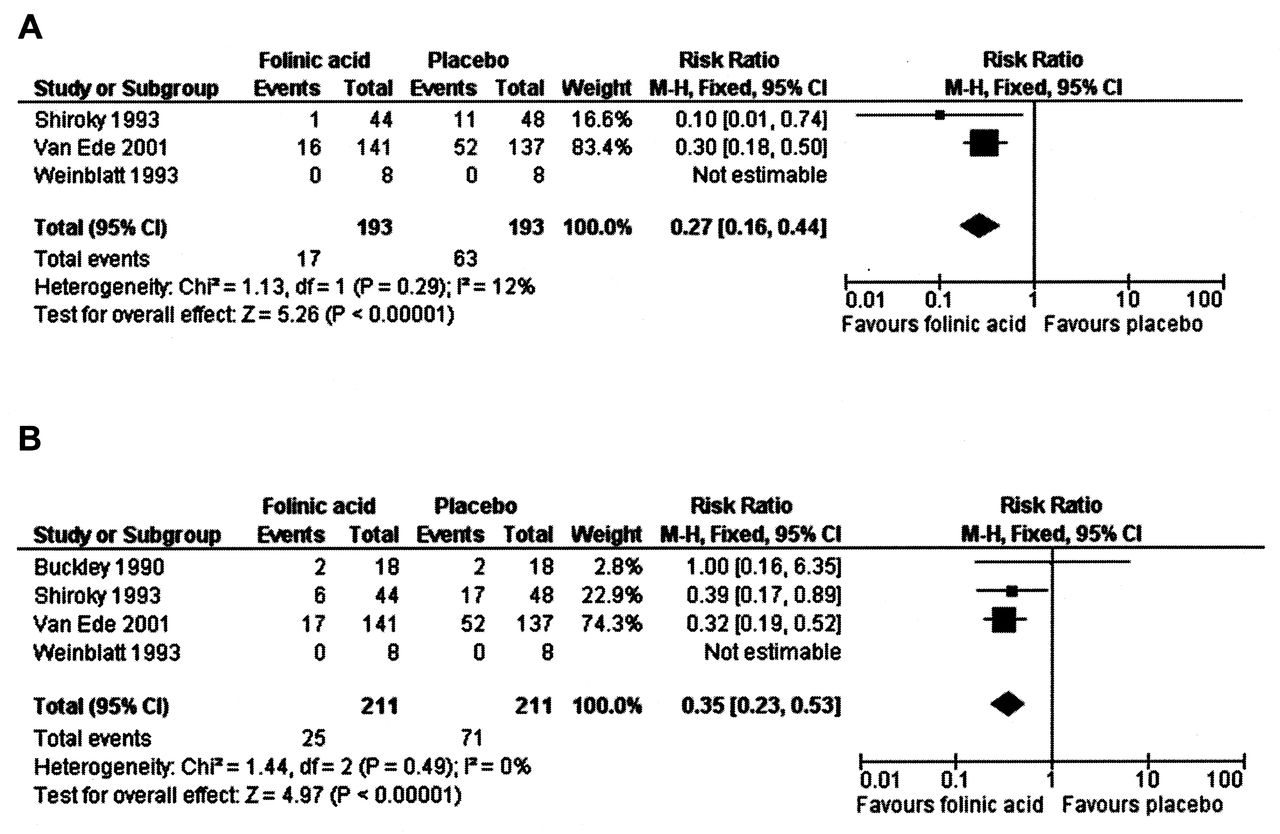
A. Liver toxicity (folinic acid vs placebo). B. Total withdrawals (folinic acid vs placebo).
Folinic acid compared to placebo for reducing side effects in patients receiving methotrexate (MTX) for rheumatoid arthritis.
Effect of folic or folinic acid on disease activity (efficacy of MTX)
No statistically significant difference in disease activity (i.e., no statistically significant lowering of the effectiveness of the MTX to treat RA) was observed between placebo and folic or folinic acid at low dosages. There was a weak signal for an increased number of tender joints in patients treated with folic acid (+2.46 swollen joints per patient, 95% CI −6.08 to 11.00; p = 0.61), and both tender and swollen joints for folinic acid (+1.13 tender joints per patient, 95% CI −4.25 to 6.51; p = 0.68), and +1.72 swollen joints per patient (95% CI −3.47 to 6.92; p = 0.52); however, the wide CI suggest that this is likely due to chance. The mean differences in disease activity (SJC and TJC, patient global assessment) between placebo and folate supplementation were analyzed. There was no evidence of a reduction in the mean differences in disease activity (SJC and TJC, patient global assessment) in the folate supplementation groups compared to placebo.
Folic acid or folinic acid versus placebo
When studies using either folic acid or folinic acid were pooled, the results were similar to the analyses of the individual agents versus placebo. Table 4 provides a detailed summary of findings, including the quality of evidence. Figures 5A, 5B, and 5C show the pooled data for nausea, liver toxicity, and total withdrawals when taking either folic acid or folinic acid compared to placebo.

A. Nausea/gastrointestinal upset (folic or folinic acid vs placebo). B. Liver toxicity (folic or folinic acid vs placebo). C. Total withdrawals (folic or folinic acid vs placebo).
Summary of findings: folic or folinic acid (any) compared to placebo for reducing side effects in patients receiving methotrexate (MTX) for rheumatoid arthritis.
Publication bias
A funnel plot to assess publication bias was not provided because there were not enough included studies to conduct this type of analysis.
DISCUSSION
The results support the protective effect of folic or folinic supplementation in patients with RA during treatment with MTX. There was a clinically important and statistically significant reduction in the incidence of abnormal transaminase elevation as well as a clinically important and statistically significant reduction in discontinuation of MTX treatment for any reason in the population studied. A trend toward a reduction in GI side effects and stomatitis was demonstrated, and although this did not reach statistical significance the concurrent statistically significant reduction in discontinuation of MTX treatment for any reason may indicate that the decrease in these side effects was greatest where the side effects were severe enough to result in MTX withdrawal. Although the analysis of hematologic side effects was made difficult by small numbers of events and the outcome being poorly reported in included studies, pooled trials reported no statistically significant differences between patients with RA who received folate supplementation or placebo. The incidence of clinically important cytopenia in patients treated with low dose MTX is estimated to be < 1%25, and therefore the size of a trial designed to detect any differences would be enormous.
Overall completeness and applicability of evidence
Sample size could potentially be a confounding variable because only 1 folinic acid study entered more than 40 patients per group. Interestingly, it appears that the benefit shown was greater for trials with higher numbers of patients and overall higher quality. Several authors26,27 have reported that the inverse is usually true with lower-quality studies showing greater benefits, suggesting biases from poor design. The finding of a trend in the opposite direction in this metaanalysis is reassuring and indicates the likely validity of the reduction of side effects from folate co-administration.
A concern with metaanalysis is the potential existence of publication bias. It is possible that some trials have been completed that found no benefit of folic or folinic acid supplementation. It is difficult to be more definitive about publication bias in this review but we feel it is unlikely that we would be unaware of negative studies of sufficient size to eliminate the benefit seen in this metaanalysis.
Three studies (excluded from our analysis) have suggested that high-dose folinic acid supplementation may reduce the beneficial effects of MTX on RA7,8,9. In a previous version of this review (where these trials were included) there was a difference observed for high-dose folinic acid, which may have suggested a decrease in benefit of the MTX on the arthritis (an isolated increase in the number of tender joints but not in other clinical variables such as patient global assessment). These results were mostly driven by the study by Joyce, et al8 and in our view are still inconclusive. We analyzed the effect of adding these studies back into our metaanalysis, and even when these studies were included the overall results did not show a statistically significant decrease in MTX efficacy. There are no studies that suggest folic acid may alter the efficacy of MTX, despite a folic acid to MTX ratio in some trials higher than the folinic acid to MTX ratio used in the study by Joyce, et al8, a finding that suggested a decrease in MTX efficacy. We did not find any major differences in disease activity between placebo and folic acid at low dosages. It is possible that the timing of administration of folinic acid and MTX, as well as the folinic acid to MTX ratio, may alter the efficacy of MTX, and it should be noted that this question was not possible to include in the design of this review.
Our results support the protective effects of low-dose folate supplementation in reducing GI and hepatic side effects of MTX in patients with RA. This is consistent with the recommendations by some authors22,24,28,29, as well as current prescribing guidelines. Deciding which of the 2 forms of folate supplementation should be recommended is more difficult. Experts have differing recommendations, often acknowledging that there is insufficient evidence for advising the use of one compound over the other5,24,26,27,30.
There is no evidence to date of a significant difference between folic or folinic acid. The results in this metaanalysis were less impressive for folinic acid, but 4 of the 5 studies had small sample sizes, and the larger study by Shiroky, et al22 did show a benefit. Given both the efficacy of folic acid in reducing MTX side effects and its low cost compared with folinic acid, the use of folic acid is likely to be the more cost-effective therapy. For folinic acid to be considered cost-effective it must be proven more effective than folic acid at reducing MTX side effects.
One study31 examined in detail the economics of folate supplementation in patients with RA and concluded that, aside from the differences in cost between folic and folinic acid, potentially the largest influence on overall treatment costs relates to the increased drug survival seen with either agent. If folate supplements can help patients tolerate MTX longer, it may delay or prevent a change in treatment to a far more expensive biologic agent. It is unclear whether all patients taking MTX, or only those with side effects, should receive folate supplementation. Our systematic review cannot address this issue. Most guidelines and texts recommend folate be given to all patients receiving MTX. Yet the effects of folic or folinic acid on the development of liver disease are unknown. It has been suggested that supplementation may have a protective effect on the development of liver disease, in which case universal administration could perhaps be considered.
Supplementation with folic or folinic acid in patients with RA who are taking MTX provides a reduction in the incidence of abnormal liver function tests and a reduction in overall withdrawal from treatment. There is also a trend toward a reduction in the incidence of GI side effects and stomatitis. The results of our review do not suggest any clear clinical advantage of one form of folate over the other.
Quality of the evidence
A major problem in synthesizing evidence is the lack of uniformity in outcome measures. All studies described themselves as randomized but some did not give details of how the randomization sequence was generated and what precautions were taken in relation to concealment of allocation. We encourage investigators to describe fully the numbers and flow of patients by treatment group throughout the trial and to clearly report the reasons for dropouts for each group. The studies were small, with few events. This metaanalysis was hampered by lack of uniformity in the way these items were reported.
Potential biases in the review process
The review was restricted to RCT; we excluded clinical controlled trials, thus limiting the potential for bias.
Our results support the protective effect of low doses of folic or folinic acid supplementation in reducing GI and liver side effects of MTX in patients with RA as well as in reducing patient discontinuation of MTX therapy. A multicenter RCT comparing both folate compounds and including an economic analysis may be necessary to adequately assess potential differences between the drugs.
Acknowledgment
We acknowledge Maria E. Suarez-Almazor and David Moher for their contribution to the original systematic review. The authors also acknowledge Alicia White for preparing the retrospective risk-of-bias tables and the original summary of findings tables, and Jessie McGowan and Margaret Sampson for preparing and executing the original search strategy. We also acknowledge Micere Thuku, Jordi Pardo, Lara Maxwell, and the Cochrane Musculoskeletal Group for their ongoing support and their help with the preparation of this manuscript.
Footnotes
-
This report is based on a Cochrane review published in The Cochrane Library 2013, Issue 5 (see www.thecochranelibrary.com for information). Cochrane reviews are regularly updated as new evidence emerges and in response to feedback, and The Cochrane Library should be consulted for the most recent version of the review.
- Accepted for publication January 31, 2014.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}