

Article Figures & Data
Figures
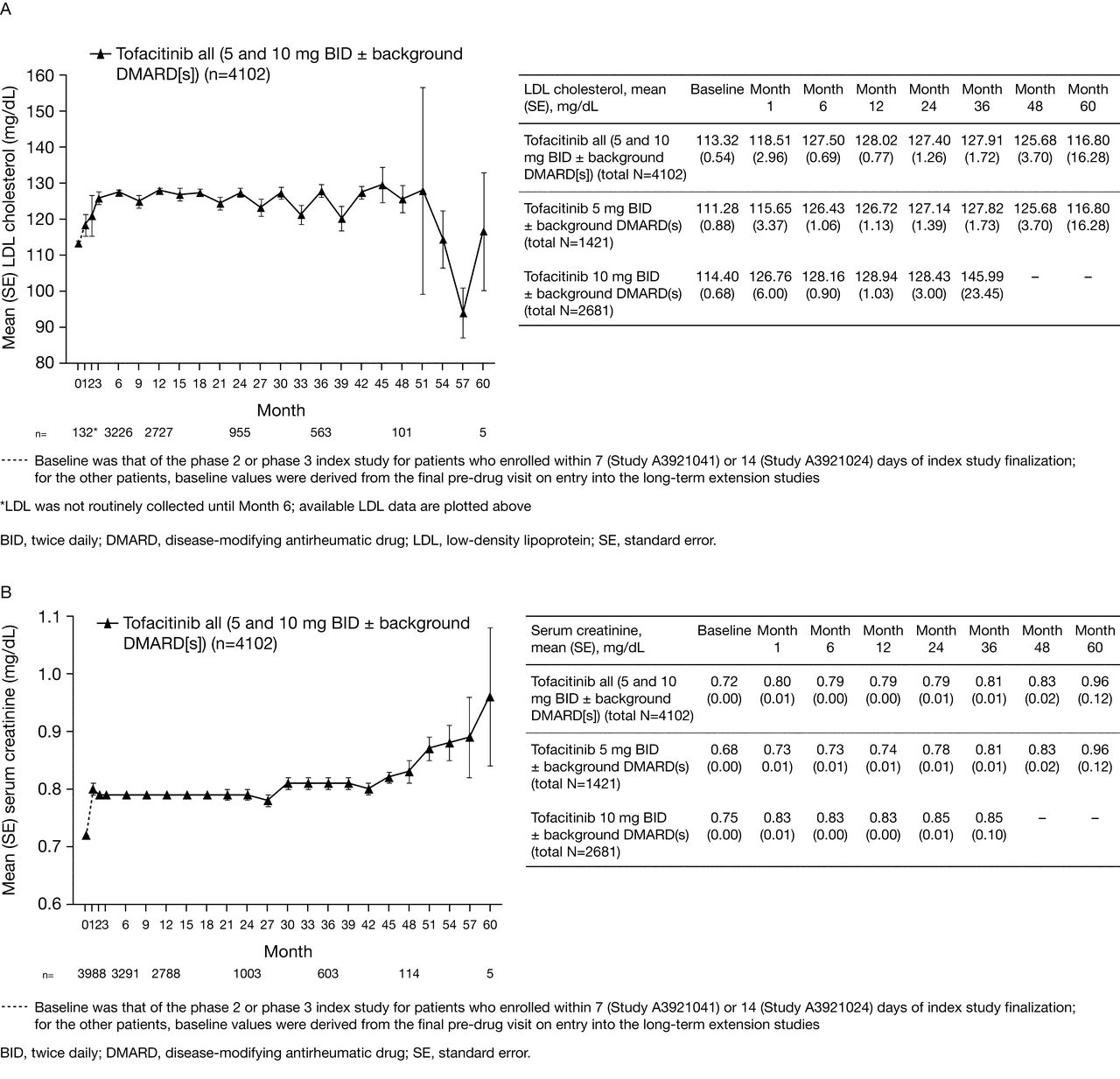
- Figure 1.
Mean (A) LDL cholesterol, (B) serum creatinine, (C) hemoglobin, (D) neutrophil counts, (E) lymphocyte counts, and (F) proportion of patients with mild neutropenia over time.
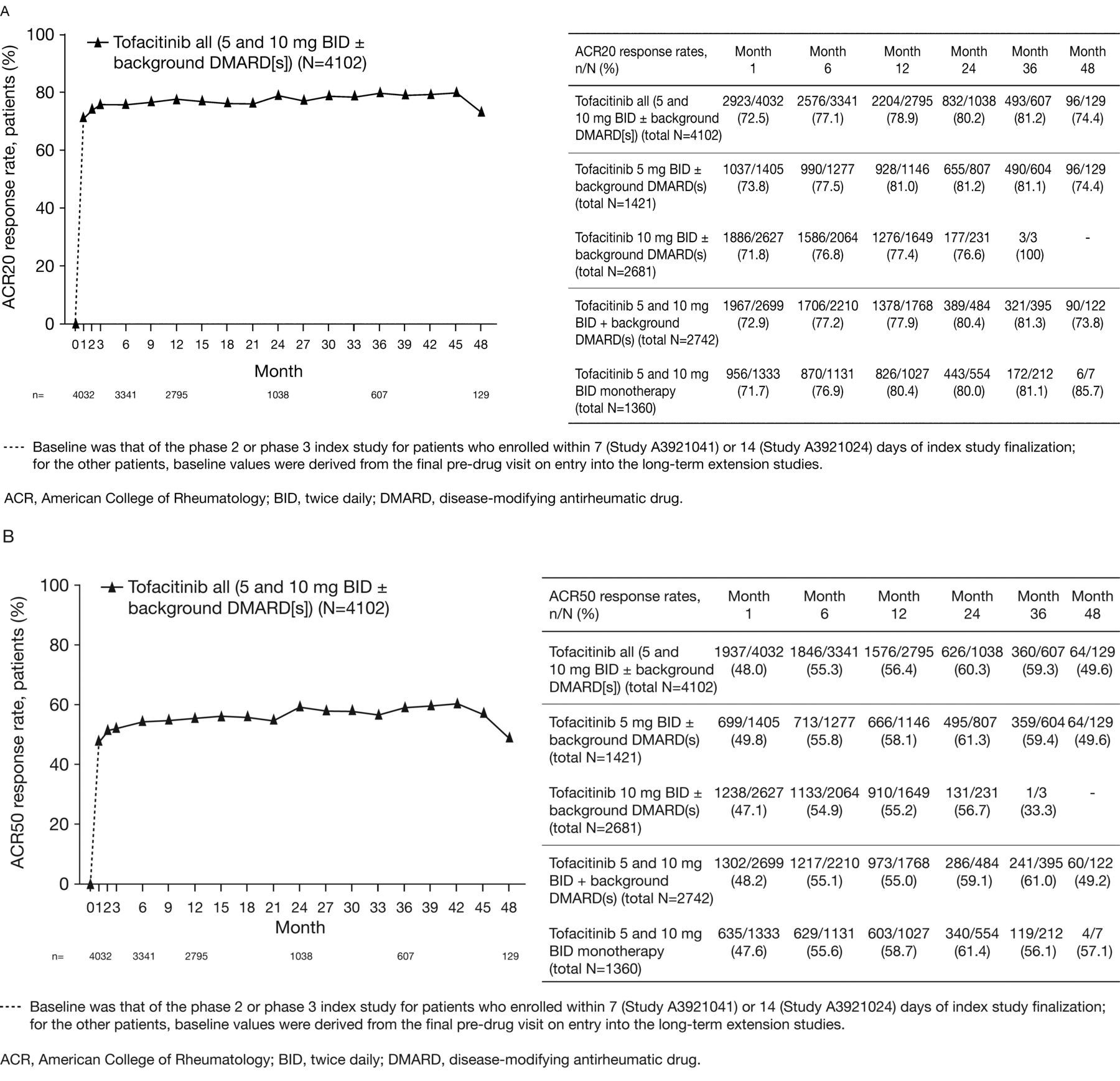
- Figure 2.
(A) American College of Rheumatology response rate: ACR20, (B) ACR50, and (C) ACR70 response rates over time.
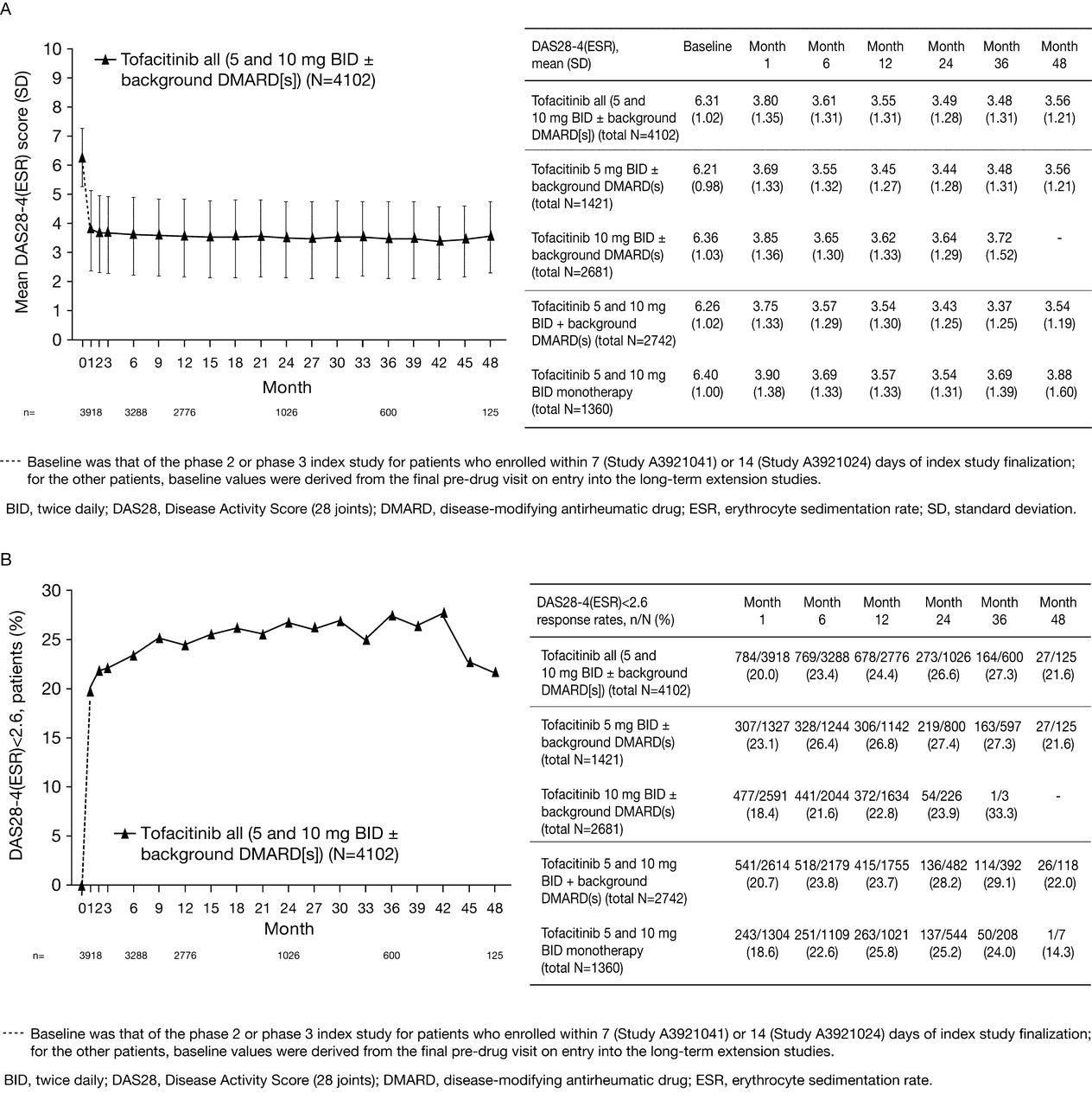
- Figure 3.
(A) Mean 28-joint Disease Activity Score (DAS28)-4[erythrocyte sedimentation rate (ESR)], (B) DAS-defined remission (DAS28-4-ESR < 2.6), (C) low disease activity (LDA; DAS28-4-ESR ≤ 3.2), and (D) mean Health Assessment Questionnaire Disability Index (HAQ-DI) over time.




Tables
Characteristic Tofacitinib All (5 and 10 mg BID ± background DMARD), n = 4102* Tofacitinib 5 mg BID ± background DMARD, n = 1421 Tofacitinib 10 mg BID ± background DMARD, n = 2681 Tofacitinib 5 and 10 mg BID + background DMARD, n = 2742 Tofacitinib 5 and 10 mg BID monotherapy, n = 1360 Total patient-yrs of exposure 5963 3215 2748 3684 2279 Mean (maximum) duration of treatment/exposure, days 531 (1844) 826 (1844) 374 (1353) 491 (1822) 612 (1844) Sex, n (%) Male 696 (17.0) 235 (16.5) 461 (17.2) 479 (17.5) 217 (16.0) Female 3406 (83.0) 1186 (83.5) 2220 (82.8) 2263 (82.5) 1143 (84.0) Mean age, yrs (SD) 53.2 (11.5) 52.8 (11.9) 53.4 (11.3) 53.4 (11.5) 52.8 (11.6) Race, n (%) White 2330 (56.8) 648 (45.6) 1682 (62.7) 1652 (60.2) 678 (49.9) Black 110 (2.7) 22 (1.5) 88 (3.3) 75 (2.7) 35 (2.6) Asian 1087 (26.5) 624 (43.9) 463 (17.3) 679 (24.8) 408 (30.0) Hispanic 14 (0.3) 14 (1.0) 0 12 (0.4) 2 (0.1) Other† 312 (7.6) 106 (7.5) 206 (7.7) 206 (7.5) 106 (7.8) Unspecified‡ 249 (6.1) 7 (0.5) 242 (9.0) 118 (4.3) 131 (9.6) Mean weight, kg (SD) 70.2 (19.2) 65.5 (17.1) 72.9 (19.9) 71.1 (19.5) 68.2 (18.5) BMI, kg/m2 (SD) 26.7 (6.4) 25.4 (5.8) 27.4 (6.6) 26.9 (6.5) 26.1 (6.1) -
↵* Baseline values were available for 3783 patients (92.2%) from the index study; 319 patients (7.8%) had new baseline values derived from the last pre-drug visit on entry to the LTE studies, or were missing baseline values as of the data cutoff.
-
↵† Excluding white, black, Asian, and Hispanic patients.
-
↵‡ Race was not provided by patients. BID: twice daily; BMI: body mass index; DMARD: disease-modifying antirheumatic drug.
-
Tofacitinib All (5 and 10 mg BID ± background DMARD), n = 4102 Tofacitinib 5 mg BID ± background DMARD, n = 1421 Tofacitinib 10 mg BID ± background DMARD, n = 2681 Tofacitinib 5 and 10 mg BID + background DMARD, n = 2742 Tofacitinib 5 and 10 mg BID monotherapy, n = 1360 Total patient-yrs of exposure* 5963 3215 2748 3684 2279 Events, n (events per 100 patient-yrs) Patients with AE 3152 (52.9) 1181 (36.7) 1971 (71.7) 2051 (55.7) 1101 (48.3) Discontinuations due to AE 437 (7.3) 211 (6.6) 226 (8.2) 284 (7.7) 153 (6.7) Patients with serious AE 630 (11.1) 295 (9.8) 335 (12.6) 400 (10.9) 230 (10.1) Patients with malignancies exc. NMSC 60 (1.0) 33 (1.0) 27 (1.0) 36 (1.0) 24 (1.0) Mortality 31 (0.5) 21 (0.6) 10 (0.4) 22 (0.6) 9 (0.4) Most frequently reported treatment-emergent (all-causalities) AE by MedDRA preferred term, n (events per 100 patient-yrs) Nasopharyngitis 521 (8.7) 303 (9.4) 218 (7.9) 296 (8.0) 225 (9.9) Upper respiratory tract infection 432 (7.2) 141 (4.3) 291 (10.6) 290 (7.9) 142 (6.2) Urinary tract infection 271 (4.5) 95 (3.0) 176 (6.4) 195 (5.3) 76 (3.3) Bronchitis 270 (4.5) 127 (4.0) 143 (5.2) 181 (4.9) 89 (3.9) Herpes zoster 245 (4.1) 127 (4.0) 118 (4.3) 133 (3.6) 112 (4.9) Influenza 162 (2.7) 92 (2.9) 70 (2.5) 104 (2.8) 58 (2.5) Hypertension 229 (3.8) 128 (4.0) 101 (3.7) 149 (4.0) 80 (3.5) Headache 185 (3.1) 94 (2.9) 91 (3.3) 106 (2.9) 79 (3.5) Diarrhea 179 (3.0) 85 (2.6) 94 (3.4) 112 (3.0) 67 (2.9) Fall 133 (2.2) 73 (2.3) 60 (2.2) 83 (2.3) 50 (2.2) Infection events, n (events per 100 patient-yrs; 95% CI) Serious infection events‡ 184 (3.1; 2.66, 3.55) 84 (2.6; 2.11, 3.24) 100 (3.6; 2.96, 4.38) 111 (3.0; 2.50, 3.62) 73 (3.2; 2.53, 4.01) Opportunistic infections (including tuberculosis)‡ 27 (0.4; 0.31, 0.65) 13 (0.4; 0.23, 0.69) 14 (0.5; 0.30, 0.85) 18 (0.5; 0.31, 0.77) 9 (0.4; 0.20, 0.75) Tuberculosis‡ 10 (0.2; 0.09, 0.31) 5 (0.2; 0.06, 0.37) 5 (0.2; 0.08, 0.43) NR NR Herpes zoster‡ 250 (4.3; 3.83, 4.90) 128 (4.2; 3.51, 4.97) 122 (4.5; 3.77, 5.38) 137 (3.8; 3.23, 4.52) 113 (5.2; 4.29, 6.20) Adverse cardiovascular events of special interest, n (%) Nonfatal myocardial infarction 3 (0.05) 3 (0.1) 0 NR NR Nonfatal cerebrovascular accident 10 (0.2) 3 (0.1) 7 (0.3) NR NR Nonfatal congestive heart failure 5 (0.1) 2 (0.1) 3 (0.1) NR NR Composite adverse cardiovascular events§ 16 (0.3) 8 (0.3) 8 (0.3) NR NR Discontinuations due to AE (all causalities), n (%) Blood and lymphatic system disorders 14 (0.3) 7 (0.5) 7 (0.3) 11 (0.4) 3 (0.2) Hepatobiliary disorders 11 (0.3) 6 (0.4) 5 (0.2) 8 (0.3) 3 (0.2) Infections and infestations 156 (3.8) 69 (4.9) 87 (3.2) 89 (3.2) 67 (4.9) Investigations (e.g., blood, creatinine increased, ALT increased, AST increased) 66 (1.6) 31 (2.2) 35 (1.3) 50 (1.8) 16 (1.2) Neoplasms (benign, malignant, and unspecified) 59 (1.4) 34 (2.4) 25 (0.9) 34 (1.2) 25 (1.8) Temporary discontinuations / dose reduction of study medication due to AE (all-causalities), n (%) Any AE 1032 (25.2) 446 (31.4) 586 (21.9) 639 (23.3) 393 (28.9) Blood and lymphatic system disorders 29 (0.7) 9 (0.6) 20 (0.7) 20 (0.7) 9 (0.7) Hepatobiliary disorders 16 (0.4) 6 (0.4) 10 (0.4) 9 (0.3) 7 (0.5) Infections and infestations 590 (14.4) 264 (18.6) 326 (12.2) 358 (13.1) 232 (17.1) Neoplasms (benign, malignant and unspecified) 12 (0.3) 3 (0.2) 9 (0.3) 8 (0.3) 4 (0.3) Laboratory variable observations Decreased hemoglobin, n (%)† n = 4095 n = 1419 n = 2676 n = 2741 n = 1354 Decrease ≥ 1 g/dl to ≤ 2 g/dl 521 (12.7) 187 (13.2) 334 (12.5) 339 (12.4) 182 (13.4) Decrease > 2 g/dl to < 3 g/dl or hemoglobin > 7 g/dl, but < 8 g/dl 109 (2.7) 49 (3.5) 60 (2.2) 64 (2.3) 45 (3.3) Decrease of ≥ 3 g/dl or hemoglobin ≤ 7 g/dl 41 (1.0) 24 (1.7) 17 (< 1.0) 21 (< 1.0) 20 (1.5) Neutropenia, n (%)† n = 4095 n = 1419 n = 2676 n = 2741 n = 1354 1500–1999 cells/mm3 158 (3.9) 78 (5.5) 80 (3.0) 91 (3.3) 67 (4.9) 500–1499 cells/mm3 30 (< 1.0) 15 (1.1) 15 (< 1.0) 20 (< 1.0) 10 (< 1.0) < 500 cells/mm3 0 0 0 0 0 Lymphopenia, n (%)† n = 4095 n = 1419 n = 2676 n = 2741 n = 1354 1500–1999 cells/mm3 966 (23.6) 280 (19.7) 686 (25.6) 631 (23.0) 335 (24.7) 500–1499 cells/mm3 2197 (53.7) 950 (66.9) 1247 (46.6) 1495 (54.5) 702 (51.8) < 500 cells/mm3 17 (< 1.0) 9 (< 1.0) 8 (< 1.0) 12 (< 1.0) 5 (< 1.0) Aminotransferases, n (%) n = 4054 n = 1413 n = 2641 n = 2721 n = 1333 AST ≥ 1 × ULN with normal baseline 1205 (29.7) 471 (33.3) 734 (27.8) 832 (30.6) 373 (28.0) AST ≥ 2 × ULN with normal baseline 152 (3.8) 69 (4.9) 83 (3.1) 106 (3.9) 46 (3.5) AST ≥ 3 × ULN with normal baseline 50 (1.2) 25 (1.8) 25 (1.0) 37 (1.4) 13 (1.0) AST ≥ 1 × ULN without regard to baseline abnormality 1516 (37.4) 545 (38.6) 971 (36.8) 1097 (40.3) 419 (31.4) AST ≥ 2 × ULN without regard to baseline abnormality 202 (5.0) 90 (6.4) 112 (4.2) 147 (5.4) 55 (4.1) AST ≥ 3 × ULN without regard to baseline abnormality 63 (1.6) 31 (2.2) 32 (1.2) 45 (1.7) 18 (1.4) ALT ≥1 × ULN with normal baseline 1134 (28.0) 451 (31.9) 683 (25.9) 774 (28.5) 360 (27.0) ALT ≥2 × ULN with normal baseline 244 (6.0) 109 (7.7) 135 (5.1) 173 (6.4) 71 (5.3) ALT ≥3 × ULN with normal baseline 90 (2.2) 43 (3.0) 47 (1.8) 61 (2.2) 29 (2.2) ALT ≥1 × ULN without regard to baseline abnormality 1513 (37.3) 553 (39.1) 960 (36.4) 1089 (40.0) 424 (31.8) ALT ≥ 2 × ULN without regard to baseline abnormality 355 (8.8) 154 (10.9) 201 (7.6) 258 (9.5) 97 (7.3) ALT ≥ 3 × ULN without regard to baseline abnormality 133 (3.3) 64 (4.5) 69 (2.6) 95 (3.5) 38 (2.9) Serum creatinine, n (%)† n = 4102 n = 1421 n = 2681 n = 2742 n = 1360 > 50% from baseline 136 (3.3) 49 (3.4) 87 (3.2) 82 (3.0) 54 (4.0) -
↵* Total patient-years of exposure are based on the safety population; some individual rates have been calculated using exposures based on specific databases for that variable/group.
-
↵† Two consecutive values.
-
↵‡ Some events may have occurred post end of treatment.
-
↵§ All cardiac deaths, i.e., coronary heart disease, cardiac death [sudden and other]; non-cardiac vascular death, i.e., pulmonary embolism cerebrovascular and other; non-fatal cardiovascular event, i.e., myocardial infarction (MI), procedural MI, cerebrovascular event. AE: adverse event; ALT: alanine aminotransferase; AST: aspartate aminotransferase; BID: twice daily: DMARD: disease-modifying antirheumatic drug; MedDRA: Medical Dictionary for Regulatory Activities; NMSC, non melanoma skin cancer; NR: not reported; ULN: upper limit of normal.
-
- Table 3.
Definite or probable cases of gastrointestinal perforations in the tofacitinib program.
Patient Age/sex Tofacitinib Dose Event Location of Perforation/surgery Concomitant Medications Onset Study Day/outcome Related Factors 52/female 3 mg twice daily + MTX Gastric ulcer perforation Upper GI/simple gastrectomy Prednisolone, methotrexate, diclofenac, rabeprazole Day 19/recovered Peritonitis was also presented, had prior recurrent gastric ulcer, smoking for 17 years, and NSAID/low-dose steroid use. 58/female 5 mg twice daily + MTX Diverticulitis and diverticular perforation Lower GI/hemicolectomy Prednisone, methotrexate, acetylsalicylic acid, diclofenac, omeprazole Day 815/recovered Diverticulitis was also presented. Perforation confirmed by pathology report. 46/male 5 mg twice daily + MTX Appendicitis Lower GI/retrocecal appendectomy Prednisone, methotrexate Day 664/death Ascending colon necrosis was also presented. Fourteen days delayed treatment for appendicitis and subsequently developed septicemia and cardiac and respiratory arrest. 55/female 5 mg twice daily + MTX Diverticulitis and intestinal perforation Lower GI/resection of sigmoid Methylpresnisolone, methotrexate, nimesulide, omeprazole Day 551/recovered 59/female 5 mg twice daily + MTX Abdominal abscess Lower GI/laparatomy omentectomy, transversectomy Methylprednisolone, aceclofenac (previous medication) Day 447/recovered Peritoneal infection was also presented. 59/male 10 mg twice daily + MTX Diverticular perforation Lower GI/sigmoid colon resection Prednisone, methotrexate, aspirin Day 362/recovered History of severe diverticulosis. Abscess intestinal was also presented. 52/female 10 mg twise daily + MTX Peritonitis and appendicitis Lower GI/appendectomy Methylprednisolone, methotrexate, omeprazole Day 45/recovered History of diverticulum. Abscess was also presented. 62/female 10 mg twice daily + MTX Diverticular perforation Lower GI/colostomy Methylprednisolone, methotrexate Day 128/recovering 62/female 10 mg twice daily + MTX Peridiverticular abscess Upper GI/sigmoid resection Prednisone, meloxicam, methotrexate, cortisone injection, pantoprazole, omeprazole Day 950/recovered Possibly secondary to the previous event of sigmoid colitis with Clostridium difficile infection; aspiration of abscesses was carried out. 61/female 10 mg twice daily + MTX Peritonitis Lower GI/unspecified surgery Prednisone, hydroxychloroquine, methotrexate, ketoprofen, deflazacort Day 357/recovered Classic symptoms of acute appendicitis. CT and surgery reports described in the narrative confirmed perforation. 66/female 10 mg twice daily + MTX Diverticular perforation Lower GI/laparoscopy Methotrexate, celecoxib Day 63/recovered Confirmed by surgical report and pathology report. -
CT: computed tomography; GI: gastrointestinal; MTX: methotrexate; NSAID: nonsteroidal antiinflammatory drugs.
-








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}