

Abstract
The “Discrimination” part of the OMERACT Filter asks whether a measure discriminates between situations that are of interest. “Feasibility” in the OMERACT Filter encompasses the practical considerations of using an instrument, including its ease of use, time to complete, monetary costs, and interpretability of the question(s) included in the instrument. Both the Discrimination and Reliability parts of the filter have been helpful but were agreed on primarily by consensus of OMERACT participants rather than through explicit evidence-based guidelines. In Filter 2.0 we wanted to improve this definition and provide specific guidance and advice to participants.
Discrimination
The “Discrimination” part of the Outcome Measures in Rheumatology (OMERACT) Filter asks whether the measure discriminates between situations that are of interest. The situations can be states at one time (for classification or prognosis) or states at different times (to measure change). The word captures the issues of reliability and sensitivity to change (responsiveness). The “Discrimination” part of the filter has been helpful but was agreed on primarily by consensus of OMERACT participants rather than through explicit evidence-based guidelines. In Filter 2.0 we want to improve this definition and provide specific guidance and advice to participants.
Various conceptual models have been considered in OMERACT for discrimination. For example, a classification system for studies of discrimination was designed to help organize the specific purpose of such studies, and identify those with the potential to provide information on minimal clinically important difference (MCID). A 3-dimensional cube was developed1; and a simplified version of the cube is provided in Figure 1 into which studies of discrimination can be categorized based on their evaluation of 3 attributes: (1) Setting, which identifies whether the study results were targeted (a) to individuals; or (b) to groups; (2) Comparison, which identifies whether discrimination was considered as (a) differences between individuals or groups at 1 point in time; (b) change within individuals or groups over time; or (c) differences in the change within individuals or groups over time; and (3) Extent of difference, which identifies whether the difference being assessed is (a) the minimum detectable; (b) the minimum relevant or important; or (c) a higher and possibly specified level of importance.
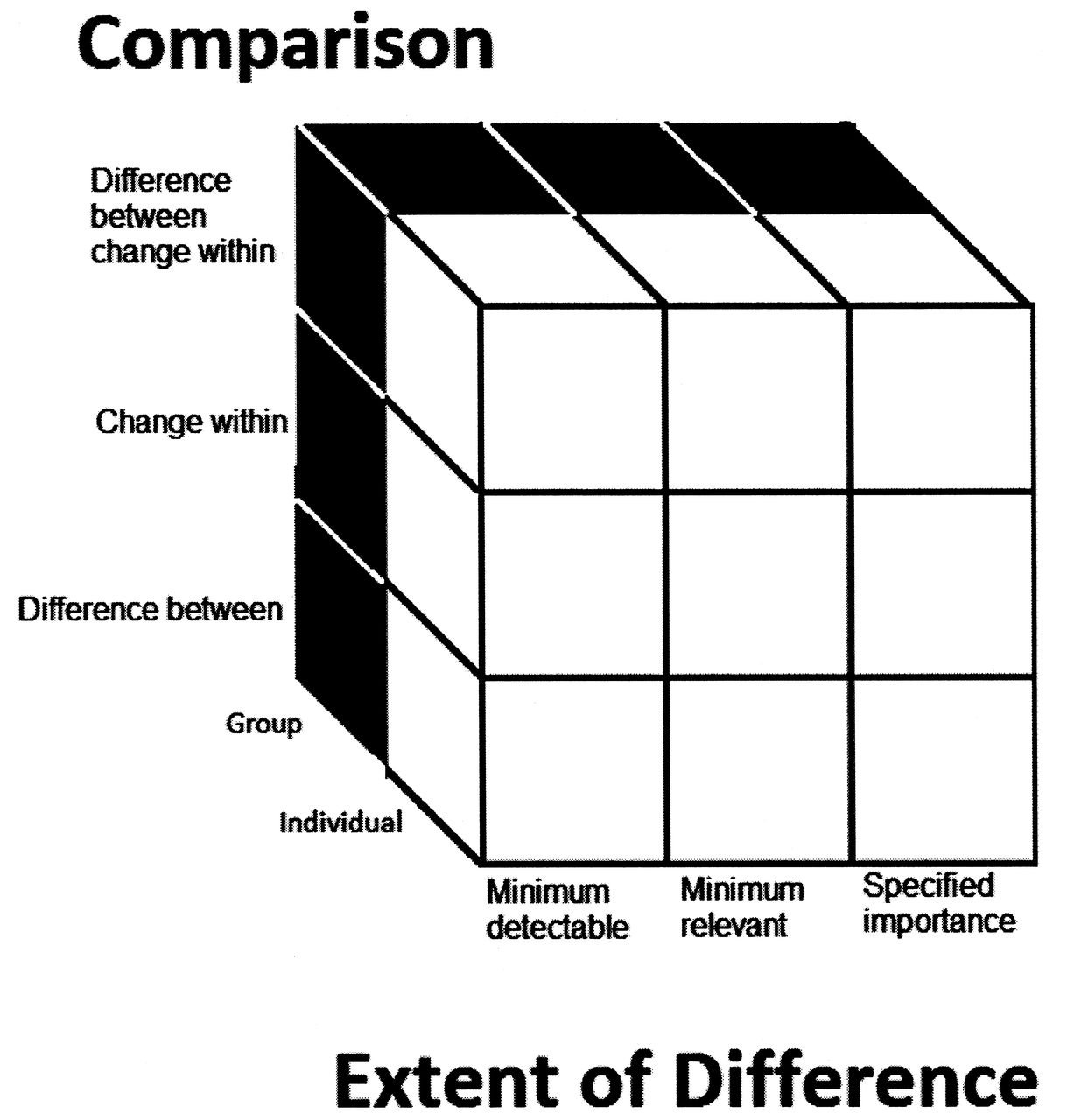
Simplified cube of discrimination. From Beaton, et al. J Rheumatol 2001;28:406–12.
This classification system helps to focus attention on the specific type of discrimination of interest in specific assessment circumstances. It reinforces an understanding that an instrument that is able to discriminate between states as represented by 1 cell within the cube will not necessarily be able to discriminate between states as represented by another cell. In particular, it is easiest for an instrument to show discrimination in the bottom, left, front corner; and most difficult in the top, right, back corner of the cube.
In the context of clinical trials the setting is usually treatment groups and the comparison is change within groups — more particularly differences between changes within groups. The sensitivity required may depend on the person involved (e.g., physician, patient, or policy maker; group or individual) and the intended use (e.g., clinical service design or research exploration). Various measures have been proposed for considering important changes and states including the MCID2, which is not without its critics3,4,5,6; and more recently the patient acceptable symptom state (PASS)7. Most have been targeted to the individual (patient) level. Other novel methodologies may be informative, such as identifying a system of levels of improvements that, for example, patients are striving to achieve.
As part of the research agenda, various paradigms for considering discrimination that integrate the different measures, perspectives, and purposes were explored. Similarly, while different methods used to define MCID or clinically important changes or important differences were previously considered and categorized according to a version of the “cube” classification system8, literature on other methods within the derived paradigm will be considered. Also, OMERACT working groups and patient groups were consulted to identify different ways that results can be viewed and the extent of discrimination was assessed by physicians and patients in their area of interest.
Feasibility
Feasibility in the OMERACT Filter encompasses the practical considerations of using an instrument, including its ease of use, time to complete, monetary costs, and interpretability of the question(s) included in the instrument. Considerations include cost of equipment, training for observers, burden/difficulty for the patient, and in the case of patient self-report, the perceived length, wording of questions, reading level, and ease of response options (clarity, ease of retrieval of information, ease of responding on that scale).
Feinstein coined the term “sensibility” to reflect an enlightened common sense appraisal of the instrument under consideration9,10. He is credited with encouraging the clinical research community to accept that this is as important as some statistically based measurement property. In Feinstein’s framework, feasibility is a key concern addressed by 6 questions: (1) Is it easy to understand? (2) Are the items, their scaling, and the aggregate score simple and easy to use? (3) Does the data collection sheet conform to basic principles of questionnaire design; are there instructions and definitions provided and are procedures standardized? (4) Is it acceptable to the patient/participant and to the observer? (5) Is the format for administration appropriate for your purpose or does it require special tests or special skills? (6) Is the administration time suitable?
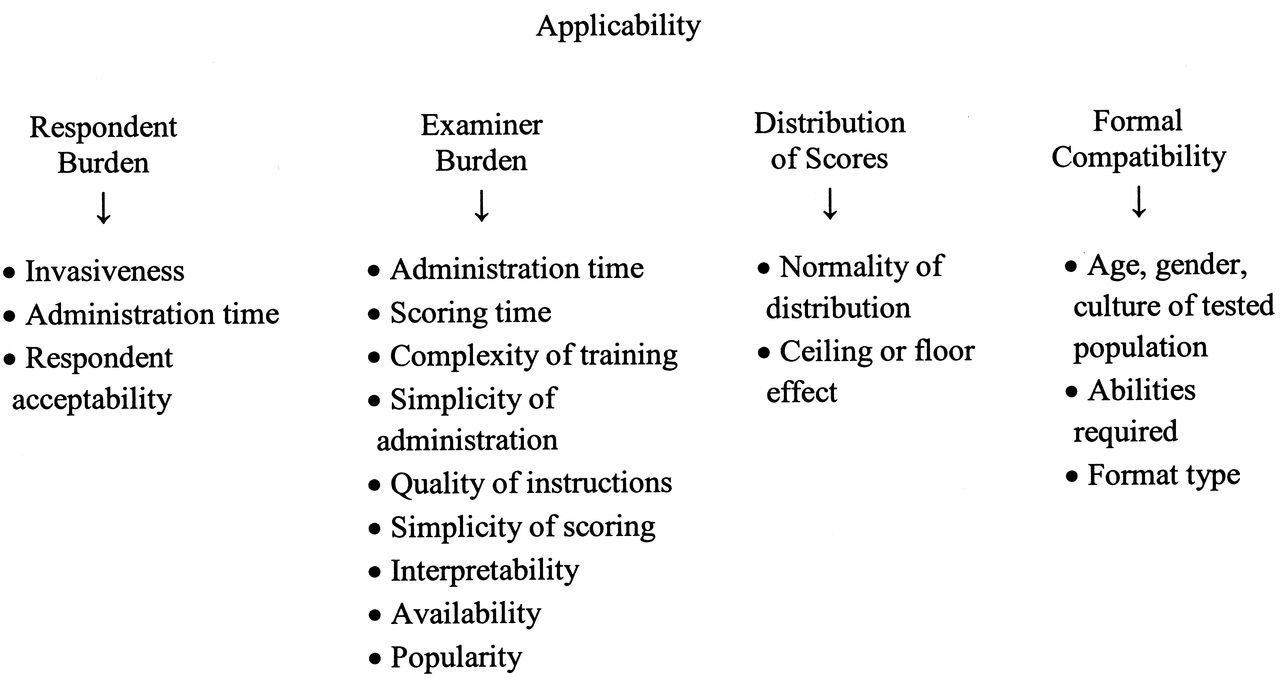
Auger, et al reviewed potential instruments to conduct this “common sense appraisal” and suggested the following main domains for assessment of feasibility (termed “applicability”): respondent burden, examiner burden, distributional issues, and format issues11.
The questions asked within Feinstein’s feasibility assessment are consistent with the domains and subdomains described by Auger (Figure 2). Note that OMERACT has traditionally used the term “applicable” to a measurement instrument that has passed all the filter requirements of Truth, Discrimination, and Feasibility12.

Feasibility is most often appraised by a researcher or clinician who is selecting the instrument. And it is the most frequently and quickly endorsed step in the OMERACT Filter. In Filter 2.0 we are seeking a more thoughtful reflection on each of the components, and consideration of a combined point of view from the researcher/clinician and patients. We proposed a merger of Feinstein and Auger’s points.
Breakout Discussion Groups
Following a plenary presentation of the topics reviewed above, conference participants were divided into 5 pairs of breakout (discussion) groups. Examples of the conduct of some discrimination exercises that had already taken place in different areas of OMERACT activity were presented to each pair of breakout groups. These were taken from work on gout, ultrasound, psoriatic arthritis, MCID, and worker productivity (Table 1, column 1). They served to provide concrete examples of the discrimination issues being addressed, and to help the discussions focus on the main questions of discrimination and feasibility for each breakout group.
Summary of the report back and discussion from the breakout groups.
Report Back and Plenary Discussion
The summary of the discussions from the breakout groups is provided in Table 1.
Discrimination
Two groups deliberated on general methods and procedures for assessing discrimination when only non-inferiority head-to-head trial data are available. The following points were noted. If a current standard treatment is effective, then placebo-controlled trials may not be possible, because they are likely unethical. New treatments can then only be compared with active treatments so there will be no comparison of the new treatment against placebo and hence no measure of the “actual” effect of the new treatment. If superiority of the new treatment is not anticipated, but the new treatment may be safer, cheaper, and/or easier to administer, then a head-to-head non-inferiority trial could be considered. A non-inferiority trial is designed to demonstrate the efficacy of a new treatment by showing that it is not less efficacious than the active control (standard treatment) by more than a specified margin, known as the non-inferiority margin. An important fact is that a well-designed and properly conducted non-inferiority trial that correctly demonstrates the treatments to be similar cannot be distinguished in itself from a poorly executed trial that fails to find a true difference. The ability of a trial to demonstrate a difference between treatments, if such a difference truly exists, is known as “assay sensitivity.” A non-inferiority trial that finds the effects of the treatments to be similar has not demonstrated assay sensitivity, and must rely on an assumption of assay sensitivity on the basis of information external to the trial. Use of past placebo-controlled trials may accomplish this, and we must have available historical data in which it has been established that standard treatment is superior to placebo. Further, we must have constancy, namely, that the historical difference between the standard and placebo is assumed to hold in the setting of the new trial if a placebo control had been used. How to use information from these trials to determine pertinent differences between groups and within patients must be identified. We would now have available direct evidence comparing the new treatment to standard treatments, and standard treatment to placebo; and, in using the standard as the common linking treatment, we can consider indirect evidence of the new treatment to placebo on which we could base these differences.
In making this assessment, in addition to assay sensitivity and constancy, an adjusted indirect treatment comparison method must be used in which the comparison of the treatments of interest is adjusted by results of their direct comparison with the standard group, thus partially using the strength of the randomized controlled trial (RCT). In the simplest, yet widely applicable setting, the method by Bucher, et al13, and generalized by Wells, et al14, is one such method.
Two breakout groups considered what general methods and procedures could be considered for determining minimum detectable, minimum relevant (important), and major differences. The breakout groups reviewed the “discrimination cube,” looking at changes within patients and at differences between groups. Considering the MCID, several issues were raised and discussed. More consideration and explanation is needed on whether the MCID applies only to patient-reported outcome (PRO) measures or whether it also applies to composite measures. Can physicians determine what an MCID is for an objective measure such as the erythrocyte sedimentation rate (ESR)? The scaling method used (e.g., numeric rating scale vs Likert scaling) may change the signal-to-noise ratio. For example, the MCID established using the anchor-based method and distribution-based method for the Health Assessment Questionnaire (HAQ) in psoriatic arthritis with etanercept was greater than that for rheumatoid arthritis, which may be a problem when considering a nonlinear score such as the HAQ. The MCID calculated for improvement may not be the same as the MCID for worsening; in this regard, it has been found that the MCID for improvement is more than that for deterioration for health-related quality of life in systemic lupus erythematosus15.
Patient involvement in the determination of MCID was raised, noting that the choice of anchors can determine the MCID, and there may be importance in obtaining patient input for determining the appropriate question. And it may make a difference, if asking about the state you would be comfortable in, if the inquiry takes the form of a global assessment, PASS, or the determination of the amount of change. Also the anchor question may be dependent on the study design or the primary outcome, and for a composite measure examining multiple aspects of disease (e.g., skin/joint), the MCID may be different for different areas involved.
Finally, the determination of MCID may be dependent on contextual factors such as the initial disease state and the disease experience (including duration and coping mechanisms), which could lead to a response shift in the MCID as well as expectations for treatment.
Two other breakout groups considered what different “situations of interest” could be considered for assessing discrimination. The difficulty in defining “situations of interest” may be most usefully considered in terms of providing examples for RCT, longitudinal observational studies, and clinical practice for each situation in the “cube of discrimination.” In particular, OMERACT has required information from 2 RCT before endorsing a measure or a responder index, and the need for 2 RCT was questioned. There may be a situation where it is not possible to obtain results from 2 RCT, or there is a negative trial with no difference in outcome between groups.
Two other breakout groups deliberated on what general methods and procedures could be considered for determining a responder index. A responder index is a combination of a series of indicators, each a threshold value on a measurement instrument. American College of Rheumatology 20% response and European League Against Rheumatism response criteria are reasonable examples of responder indices. Such an index should ideally be discriminative in situations of both improvement and worsening.
The final pair of breakout groups each considered what items constitute a practical checklist for discrimination. While noting the COnsensus-based standards for the selection of Health Measurement INstruments (COSMIN) checklist16, discussion on this was limited because necessary information was lacking and time was too short. One breakout group noted that discrimination as presented in Filter 112 appears to be the best way to proceed, but there is a need for more examples. To test responsiveness, the group believed that one should consider an RCT where there is a known treatment effect and then assess the change in the outcome of interest. Further, one should look for responsiveness first at group level, and then at individual level. The treatment effect should be anchored to a PRO to be best understood by patients. The discussion on diminishing the role of effect size in assessing discrimination was not resolved.
Feasibility
Three pairs of breakout groups also deliberated on how the feasibility of a measure or group of measures could be assessed, taking into consideration aspects such as cost, burden, and interpretability. Two groups felt feasibility should be considered early, as part of the “development loop” from the beginning to the end of the process in developing an instrument, and that pilot testing for feasibility should be conducted. The issue of capturing information on paper versus by computer in different sites globally was raised as an important issue related to feasibility. Longitudinal data capture and frequency of data collection can be burdensome issues related to feasibility and, for that matter, to validity. The possibility of developing a feasibility “score” was raised.
In summary, this OMERACT session was designed to evaluate key aspects of discrimination and feasibility proposed for the Filter 2.017 framework that had been discussed prior to the meeting and/or arisen as issues in using the discrimination and feasibility descriptions of the original filter over the years. Using specific topics on discrimination and a general question on feasibility raised in questions, OMERACT 11 participants were able to probe the theoretical and practical implications of the framework and examine areas of strength and weakness. Although specific aspects and issues were raised regarding the various topics related to discrimination and feasibility, providing guidance and research agenda topics, there was general agreement that the more explicit explanations of discrimination and feasibility to be included in Filter 2.0 would help developers of core outcome measures.








{kind=link}
{kind=link}