

Abstract
Objective. Systemic necrotizing vasculitides (SNV) are associated with more frequent subclinical atherosclerosis, suggesting that SNV might be associated with a higher risk of major cardiovascular events (MCVE). We aimed to identify factors predictive of MCVE in patients with SNV.
Methods. Patients in remission from SNV were assessed for CV risk factors and subclinical atherosclerosis. MCVE was defined as myocardial infarction, stroke, arterial revascularization, hospitalization for unstable angina, and/or death from CV causes. MCVE-free survival curves were compared using the log-rank test.
Results. Forty-two patients were followed for 7.1 ± 2.6 years. Eight patients (18.9%) had MCVE. The respective 5- and 10-year MCVE rates were 9.5% and 26.8%. National Cholesterol Education Program/Adult Treatment Panel III (NCEP/ATP III)-defined high-risk status [hazard ratio (HR) 5.02 (95% CI: 1.17–27.4), p = 0.03], BMI > 30 kg/m2 [HR 4.84 (95% CI: 1.46–116), p = 0.02], and plaque detection in the abdominal aorta (p = 0.01) were significantly associated with MCVE. SNV characteristics, corticosteroid maintenance therapy, and C-reactive protein > 5 mg/l were not associated with MCVE. Plaque in the aorta was significantly associated with high-risk status (p < 0.001), while BMI and high-risk status were independent variables. Thus, a BMI > 30 kg/m2 and/or a high-risk status were strongly associated with MCVE (p = 0.004). Carotid intima-media thickness (IMT) identified patients with early MCVE and was correlated with the time to MCVE (r2 = 0.68, p = 0.01).
Conclusion. These results suggest that factors associated with a higher MCVE risk in patients with SNV are NCEP/ATP III-defined high-risk status and BMI > 30 kg/m2. Carotid IMT could help identify patients with SNV at risk of early MCVE.
Vasculitides, inflammation of large, medium, and/or small blood vessel walls, have protean clinical manifestations that can be fatal or can damage organs1,2. Their initial clinical pictures and outcome vary among the different forms, and can be distinguished according to the types of vessels affected. The nomenclature for vasculitides was revised in 20123. Among vasculitides, systemic necrotizing vasculitides (SNV) may be individualized and include polyarteritis nodosa (PAN) and the antineutrophil cytoplasmic antibody (ANCA)-associated vasculitides [granulomatosis with polyangiitis (GPA), microscopic polyangiitis (MPA), and eosinophilic granulomatosis with polyangiitis (Churg-Strauss syndrome; EGPA)]. Over the past few decades, the development and subsequent optimization of immunosuppressive therapies have significantly reduced vasculitis-related mortality, but survivors may have disease-induced damage and resulting poor organ function, morbidity, and mortality related to treatment adverse events and cardiovascular (CV) diseases4,5,6. As for other chronic systemic inflammatory diseases, premature and accelerated atherosclerosis has emerged during the last 10 years as an important facet of vasculitides.
Previous studies demonstrated the presence of subclinical atherosclerosis in patients with SNV. First, experimental data showed that, in addition to lipid accumulation, arterial inflammation, attributable to Th1 and Th17-lymphocytes infiltration, and systemic inflammation resulting from increased tumor necrosis factor (TNF)-α and interleukin (IL)-6 production were associated with accelerated subclinical atherosclerosis7,8. Second, during the last decade, results of epidemiological studies showed the higher frequencies of subclinical atherosclerosis in patients with SNV9,10,11,12,13,14. Our group previously compared 50 primary patients with SNV to 100 age-matched and sex-matched controls and found that patients with SNV had higher frequency of plaque in the carotid artery and aorta than did controls, independent of CV risk factors and systemic inflammation9. Notably, the ability of surrogate markers of subclinical atherosclerosis to predict future major CV events (MCVE) has been reported15. However, the effect of those surrogate markers on MCVE occurrence in patients with SNV was not evaluated in a longterm followup.
Our study was undertaken to identify factors predictive of MCVE in patients with SNV by analyzing the longterm followup for CV risk and subclinical atherosclerosis.
MATERIALS AND METHODS
Patients
Between September 2002 and May 2005, 50 consecutive patients in complete remission of vasculitis (Birmingham Vasculitis Activity Score = 0) underwent baseline CV risk assessment and subclinical atherosclerosis detection9, and were prospectively followed in the same center; 8 were lost to followup. SNV, treatment characteristics, and outcomes were recorded for the remaining 42 patients.
CV risk factors and systemic inflammation
Brachial artery blood pressure was the average of 2 successive sphygmomanometric measurements obtained with the patient in the supine position after a 5-min rest. Hypertension was defined as blood pressure ≥ 140/90 mmHg or the use of antihypertensive drugs. Total cholesterol, high-density lipoprotein cholesterol after precipitation of low-density lipoprotein (LDL) and very LDL cholesterol, and triglycerides were measured enzymatically after overnight fasting. LDL cholesterol was calculated using the Friedewald formula16. Hypercholesterolemia was defined as total cholesterol ≥ 5.18 mmol/l, LDL cholesterol ≥ 3.30 mmol/l, or use of lipid-lowering drugs. Current smoking was defined as at least 1 cigarette smoked within the month before inclusion. Blood glucose was measured enzymatically. Diabetes mellitus was defined as fasting blood glucose ≥ 7 mmol/l or use of drugs for diabetes. Body mass index (BMI) was the ratio of weight (kg) to height squared (m2). High-risk status was defined according to the National Cholesterol Education Program—Adult Treatment Panel III guidelines as the presence of a known personal history of CV diseases, including all types of documented coronary, cerebrovascular, or peripheral arterial disease; diabetes mellitus; or a Framingham Risk Score ≥ 20% at 10 years17. Systemic inflammation was assessed by measuring C-reactive protein using a high-sensitivity immunoassay18.
Subclinical atherosclerosis
High-resolution ultrasonography (Ultramark 5000, Philips) measured the presence of plaque in 3 peripheral sites (both extracranial carotid arteries, abdominal aorta, and both femoral arteries), as described previously19. Briefly, a plaque was defined as a focal echogenic structure encroaching into the lumen > 1.5 mm, and a vessel examined was considered to be a carrier of plaque if at least 1 such structure was present, regardless of location, side, and number19. The number of plaque-containing sites (i.e., the sum of the 3 sites: carotid, femoral, and aorta) ranged from 0 to 319. Agreement between repeated plaque detection ranged from 94% to 100% depending on the vessel19. In addition to plaque detection, common carotid intima-media thickness (CIMT) was measured in the far wall along at least 1 cm of length, by high-resolution ultrasound, with a procedure described and validated previously20. Briefly, the CIMT image, obtained at end diastole, was analyzed offline using an automated computerized program, and the coefficient of variation of 2 repeated CIMT measurements was, on average, 4%.
MCVE
Any MCVE (defined as myocardial infarction, stroke, arterial revascularization procedure, hospitalization for unstable angina, and/or death from CV causes) occurring during followup was recorded.
Statistical analysis
Data are reported as n (%) for categorical variables and means ± SD or medians, as appropriate, for quantitative variables. Univariate analysis identified factors associated with MCVE. Kaplan-Meier MCVE-free survival curves were plotted and compared with the log-rank test. A chi-square test for independence was used to analyze the interaction between variables. A p < 0.05 was considered statistically significant. Statistical analyses were done using Prism (GraphPad Software Inc.).
RESULTS
Characteristics of the patients
Forty-two patients (27 males, age 54 ± 15 yrs) were included. SNV diagnoses were GPA in 20 patients, EGPA in 9, MPA in 8, and PAN in 5. CV risk factors are presented in Table 1.
Baseline characteristics of the 42 patients with SNV with longterm followup. Data are no. (%) or median (range) as appropriate.
Eighteen (43%) patients were taking aspirin and 22 (52%) received statins for primary prevention of CV events. The mean Framingham Risk Score was higher in patients with aspirin compared to those without (14.3% ± 9.0 vs 5.2% ± 4.4), and for patients with statins compared to those without (14.3% ± 9.0 vs 5.2% ± 4.4). Angiotensin-converting enzyme inhibitors were prescribed to 12 patients (29%) with arterial hypertension.
CV outcome of the patients
After a mean followup of 7.1 ± 2.6 years, 8 patients (19%) with SNV had MCVE: 4 had myocardial infarction or hospitalization for unstable angina, 2 underwent arterial revascularization, 1 had a stroke, and 1 died of CV causes. Respective 5-year and 10-year MCVE rates of 9.5% and 26.8% markedly exceeded the expected 10-year Framingham CV risk score (9%). We also distinguished between early and late (within the first 3 yrs and after 7 yrs of followup, respectively) MCVE that occurred in our study population (Figure 1).

Kaplan-Meier estimate of the major cardiovascular event (MCVE)-free survival rates for the 42 patients with systemic necrotizing vasculitides included in the study.
SNV-related factors predictive of MCVE
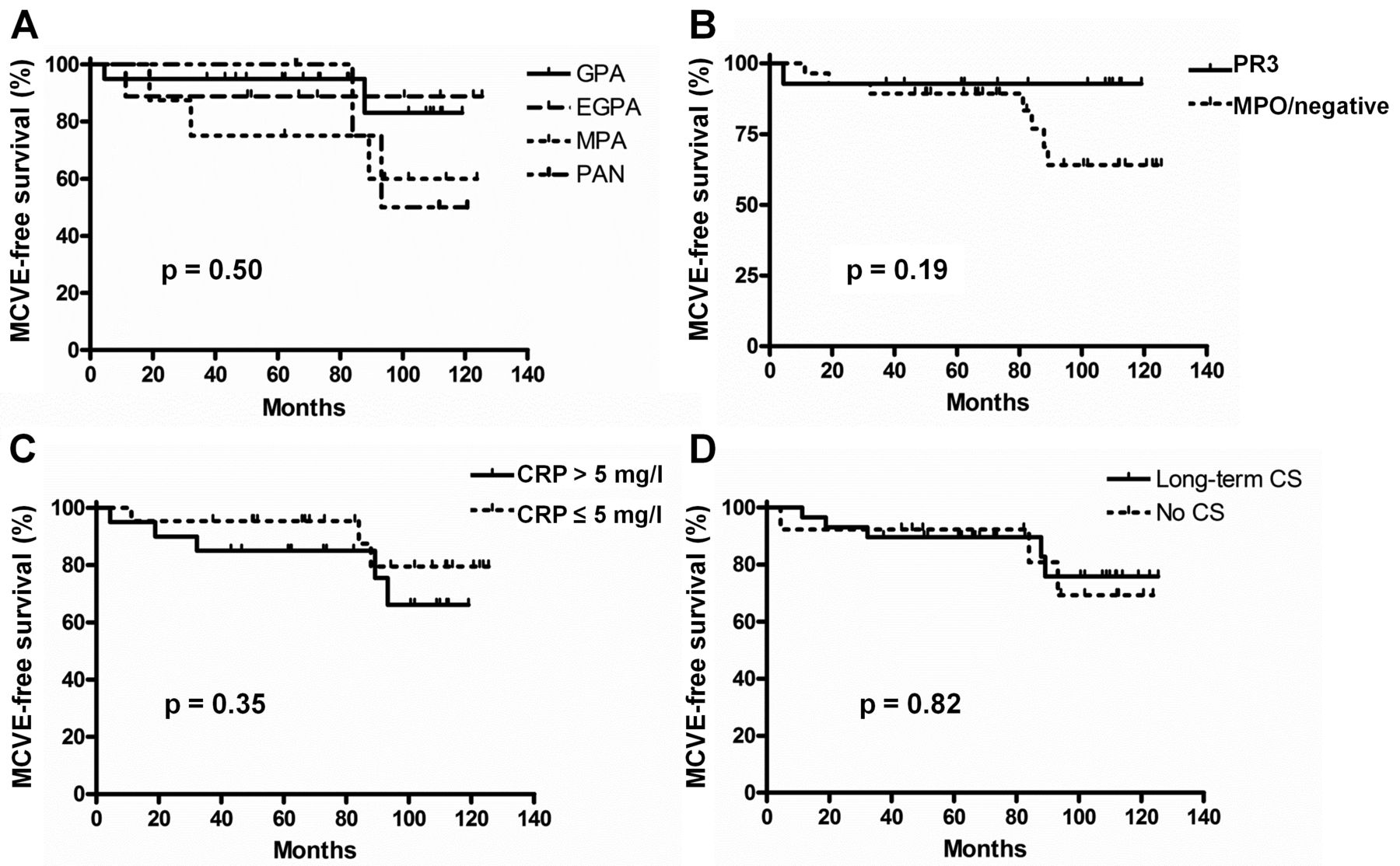
The effect of SNV-related features on MCVE occurrence during followup was assessed using univariate analysis. None of the SNV characteristics at the time of inclusion (e.g., vasculitis type, ANCA status, systemic inflammation, or longterm corticosteroid use) was associated with MCVE (Figure 2). However, more MCVE appears to have occurred in patients with MPA than in those with GPA or EGPA, and in patients with myeloperoxidase (MPO)-ANCA or in ANCA-negative patients than in those with proteinase 3 (PR3)-ANCA, but this was not significant. Fifteen patients (36%) experienced SNV flares during followup, but the flares had no effect on MCVE occurrence.
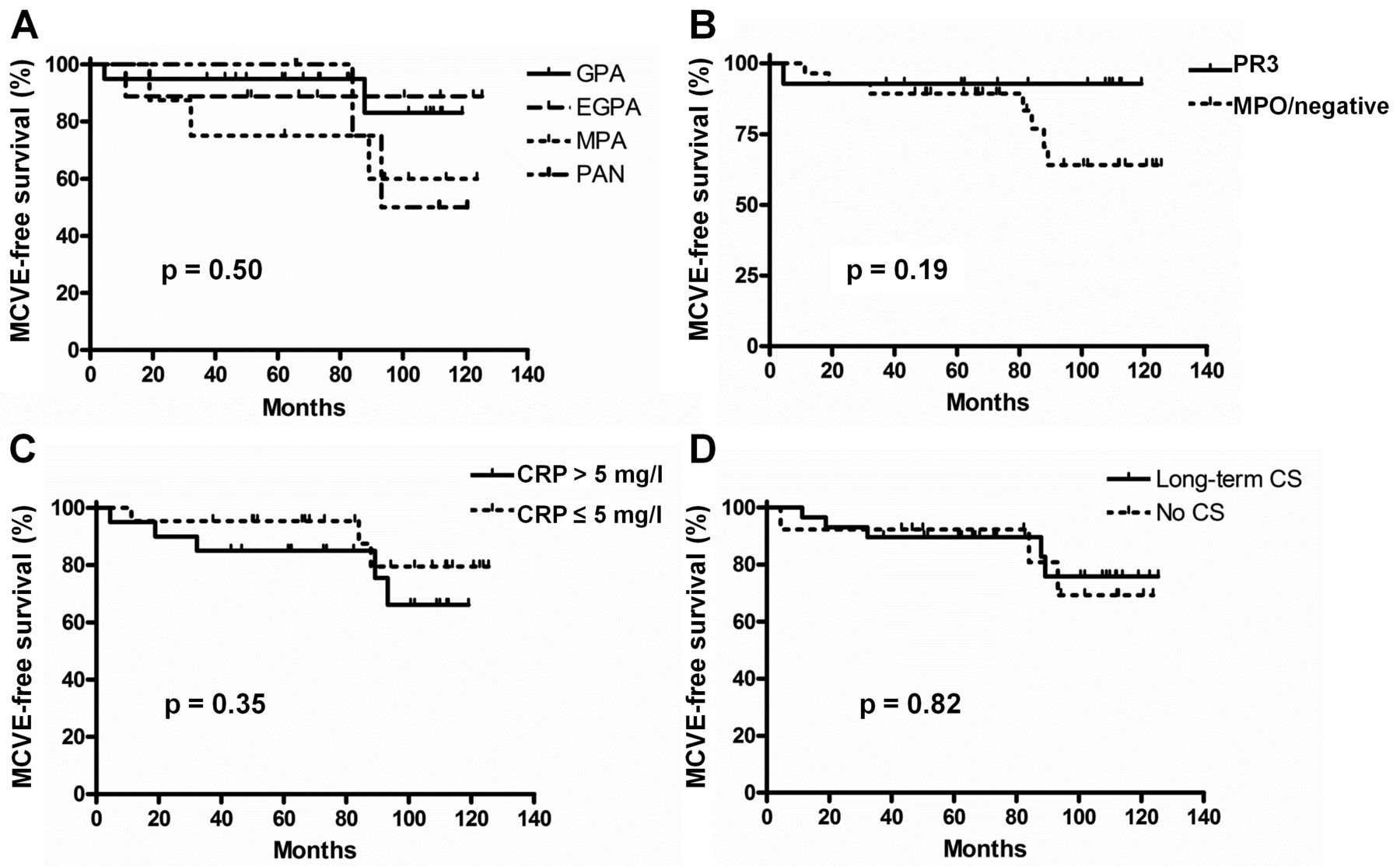
Kaplan-Meier estimates of the major cardiovascular event (MCVE)-free survival rates for the 42 patients according to their (A) systemic necrotizing vasculitides diagnosis; (B) proteinase 3 (PR3)-ANCA or myeloperoxidase (MPO)/negative ANCA; (C) systemic inflammation [C-reactive protein (CRP) ≤ or > 5 mg/l]; and (D) the longterm corticosteroid (CS) use (duration > 36 mos) or not (duration ≤ 36 mos). MCVE-free survival rates were compared using the log rank test in univariate analysis. ANCA: antineutrophil cytoplasmic antibodies.
Subclinical atherosclerosis factors predictive of MCVE
The effect of subclinical atherosclerosis on MCVE occurrence during followup was assessed next. Plaque detection in carotid arteries was not significantly associated with MCVE (Figure 3A). In contrast, plaque detection in the abdominal aorta was strongly associated with plaque presence in the femoral arteries (chi-square 21.95, p < 0.0001), and was significantly associated with MCVE [hazard ratio (HR) 7.09, 95% CI: 1.07–17.4, p = 0.03; Figure 3B]. Finally, plaque detection in ≥ 2 of the 3 peripheral vessels analyzed compared to plaque in 0 or only 1 vessel was also significantly associated with MCVE (HR 8.27, 95% CI: 1.34–21.8, p = 0.02; Figure 3C).
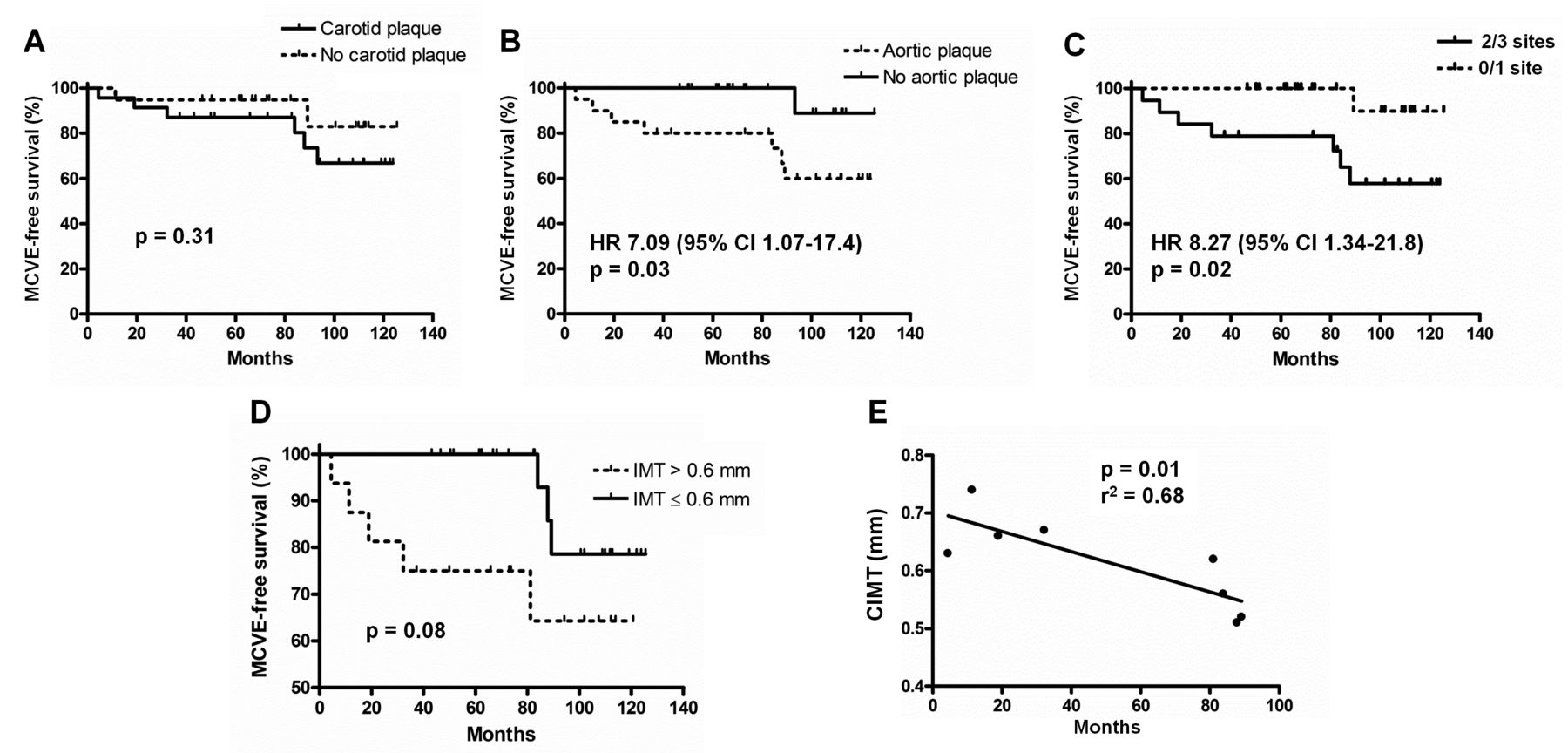
Kaplan-Meier estimates of the major cardiovascular event (MCVE)-free survival rates for the 42 patients with systemic necrotizing vasculitides according to the presence or absence of (A) carotid or (B) aortic plaque; (C) plaque in ≥ 2 of the 3 peripheral vessels analyzed or none; and (D) the carotid intima-media thickness measurement (CIMT ≤ or > 0.6 mm). E. Correlation between CIMT measurement and time to first MCVE.
CIMT tended to be associated with MCVE (p = 0.08), and identified patients with early (within the first 3 yrs of followup) MCVE. Four of 16 patients with CIMT > 0.60 mm (vs none of those with CIMT ≤ 0.60 mm) experienced early MCVE, while 3/26 patients with CIMT ≤ 0.60 mm (vs only 1 of those with CIMT > 0.60 mm) experienced a first MCVE after 7–10 years of followup (Figure 3D). Moreover, CIMT was correlated with the time to MCVE (r2 = 0.68, p = 0.01; Figure 3E).
CV risk factors predictive of MCVE
Finally, the effect of CV risk factors on MCVE occurrence during followup was evaluated. MCVE was significantly associated with NCEP/ATP III-defined high-risk status (HR 4.16, 95% CI: 1.14–24.6, p = 0.03) or BMI > 30 kg/m2 (HR 4.91, 95% CI: 1.72–152, p = 0.01; Figures 4A and 4B).

Kaplan-Meier estimates of the major cardiovascular event (MCVE)-free survival rates for the 42 patients with systemic necrotizing vasculitides according to (A) the presence or absence of NCEP/ATP III-defined high-risk status; (B) body mass index (BMI ≤ or > 30 kg/m2); or (C) BMI > 30 kg/m2 and/or high-risk status. MCVE-free survival rates were compared using the log rank test in univariate analysis. NCEP/ATP: National Cholesterol Education Program/Adult Treatment Panel III.
Analysis of the interaction of the factors (i.e., plaque in the abdominal aorta, high-risk status, and BMI > 30 kg/m2) associated with MCVE showed that aortic plaque was significantly associated with high-risk status (chi-square 11.24, p = 0.0008), while BMI and high-risk status remained independent variables (chi-square 0.04, p = 0.83). Thus, BMI > 30 kg/m2 and/or a high-risk status were strongly associated with MCVE (HR 11.30, 95% CI: 1.94–33.8, p = 0.004; Figure 4C).
DISCUSSION
Subclinical atherosclerosis in patients with SNV compared to healthy controls was previously described9,10,11 and only 1 study to date identified factors predictive of MCVE in patients with SNV13. To provide additional data concerning this comorbidity, we analyzed the longterm followup of patients with SNV previously evaluated for CV risk factors and subclinical atherosclerosis9 and prospectively followed up at our SNV referral center. The most striking conclusions of our analysis are (1) the confirmation of accelerated atherosclerosis in patients with SNV compared to the calculated Framingham risk expected; (2) the identification of factors routinely assessed in daily clinical practice that are predictive of MCVE in patients with SNV; and (3) the potential contribution of CIMT measurement in high-risk patients to identify those at early risk of MCVE.
Herein, the observed respective 5- and 10-year MCVE rates of 9.5% and 26.8% were similar to the 5-year MCVE rates of 13.8% reported by Suppiah, et al in patients with newly diagnosed GPA and MPA without premorbid CV disease13. However, our study population was quite different, because it included 21% patients with EGPA and 12% patients with PAN, and 29% of our patients had NCEP/ATP III-defined high-risk status. Our observations confirmed accelerated atherosclerosis in patients with SNV based on their longterm followup rather than the presence of markers of subclinical atherosclerosis, and are further supported by the observed 10-year MCVE rate that largely exceeded the expected 10-year Framingham risk score of 9%. Thus, this longitudinal followup indicated that patients with SNV had 2-fold to 3-fold accelerated atherosclerosis, which may classify them as being at high CV risk, regardless of their traditional risk factors.
The elevated MCVE rate in patients with SNV led us to assess the effect of SNV characteristics, traditional CV risk factors, and subclinical atherosclerosis markers on the occurrence of MCVE during followup, to identify patient characteristics commonly used in routine clinical practice, and be able to predict MCVE. Traditional CV risk factors were the most effective predictors of MCVE occurrence. In contrast, SNV characteristics and corticosteroid maintenance therapy had no effect on the MCVE rate. Although not significant because of the small number of patients, our findings are consistent with those of Suppiah, et al, who reported that PR3-ANCA were associated with a lower CV risk than MPO-ANCA or ANCA negativity13. Although our study did not have sufficient power to enable us to draw definitive conclusions, we think that ANCA status probably has limited effect compared to traditional CV risk factors. Notably, NCEP/ATP III-defined high-risk status and/or a BMI > 30 kg/m2 were strongly associated with MCVE. The presence of markers of subclinical atherosclerosis, particularly plaque detection in the abdominal aorta, was associated with NCEP/ATP III-defined high-risk status. Studies on patients without SNV demonstrated the contribution of subclinical carotid atherosclerosis to predict future MCVE15, but surprisingly, carotid plaque failed to provide additional support in predicting MCVE occurrence in our patients with SNV. It was previously shown that the use of additional atherosclerosis markers to assess CV risk in individuals often added only moderately to standard risk factors21. Thus, as in the general population, simple predictive factors, i.e., NCEP/ATP III-defined high-risk status and/or a BMI > 30 kg/m2, can be used to identify patients with SNV at risk of MCVE.
Finally, CIMT > 0.6 mm tended to be associated with MCVE and helped identify at-risk patients with early MCVE. These findings strongly suggest that the assessment of CV risk factors and BMI should be mandatory for management of patients with SNV. At-risk patients should be screened for atherosclerosis, especially CIMT measurement, which could guide preventive management of therapy and/or revascularization procedure if necessary. In contrast, low-risk patients should be screened regularly for CV risk factors and obesity.
Our study contains some limitations. First, we included a small and heterogeneous sample of patients, with 8 out of 50 patients from the original study lost to followup after the initial evaluation, and no control group available for comparison. Second, our pooling of patients with different SNV, rather than focusing on a specific disease, might have introduced bias into the analysis. However, no differences between the different types of vasculitides were found. Third, we did not include other subclinical atherosclerosis markers that could represent interesting tools in daily clinical practice. For example, a more frequently abnormal ankle-brachial pressure index, a noninvasive assessment of CV risk, was previously shown to occur more frequently in patients with SNV compared to healthy controls and to be associated with CV events in patients with SNV22. Similarly, endothelial dysfunction, a predictor of atherosclerotic disease, assessed by flow-mediated brachial artery vasodilatation, was very common in primary SNV23. However, these 2 biomarkers add little to the Framingham score’s predictive value in the non-SNV general populations24,25. Fourth, we cannot exclude the influence of corticosteroids on MCVE occurrence, because patients with higher inflammatory activity were probably more likely to receive longterm corticosteroids than those with less inflammatory disease. In contrast, one of our study’s strong points is the monocenter design of its initial assessment and followup using homogeneous management.
Our results indicate that patients with SNV have factors associated with a higher MCVE risk: NCEP/ATP III-defined high-risk status and BMI > 30 kg/m2. CIMT measurement in patients with SNV might help identify those at risk of early MCVE and should probably be done systematically in patients with NCEP/ATP III-defined high-risk status and BMI > 30 kg/m2 to adapt their CV risk management.
- Accepted for publication December 13, 2013.








{kind=link}
{kind=link}
{kind=link}
{kind=link}