

Abstract
Objective. The recovery time from abnormal levels of proteinuria with standard treatment in longitudinal studies of patients with systemic lupus erythematosus has not been well described. We aimed (1) to determine the recovery time from proteinuria in patients with lupus nephritis (LN) receiving standard treatment, and (2) to determine whether the initial level of proteinuria predicts time to improvement.
Methods. We studied all patients with LN recorded in the database from 1970 until 2011. Proteinuria was defined as ≥ 0.5 g/24 h. Patients were grouped as follows: group 1 having 0.5–0.9 g/day, group 2 having 1–1.9 g/day, and group 3 having ≥ 2 g/day. Recovery from proteinuria was defined as proteinuria < 0.5 g/24 h. Time to recovery from proteinuria was studied with the Kaplan-Meier curves. Factors associated with proteinuria recovery were evaluated using proportional hazard models.
Results. Among the 212 patients studied, 52% recovered from proteinuria within 2 years and an additional 22% recovered within 5 years, for a total of 74%. The level of proteinuria at baseline visit predicted the time to improvement. Patients with a higher level of proteinuria at baseline needed a longer time to normalize their proteinuria. Male sex, hypocomplementemia, high level of proteinuria at diagnosis of LN, and disease duration > 5 years at onset of LN each independently predicted late recovery of proteinuria and had an effect on the percentage of patients who recovered.
Conclusion. The tempo of recovery from proteinuria in LN is slow and the level of proteinuria at baseline visit predicts the time to complete recovery.
Systemic lupus erythematosus (SLE) is a multisystem autoimmune disease that affects many organs. Lupus nephritis (LN) occurs in 50–75% of adults with SLE and predicts poor survival1. In general, most instances of LN emerge within the first 36 months from diagnosis, although some patients develop LN later in their course of disease2. Patients with LN display a spectrum of pathologic findings on renal biopsy, abnormal urinalysis with active urinary sediments and proteinuria, alteration of renal function, and active SLE serology.
In clinical trials and observational research studies, several endpoints and outcome measures have been developed or adopted to evaluate the activity of LN. In the majority of clinical trials for LN, the primary outcome of interest has been the achievement of complete, partial, or overall remission. The determination of remission is based on the assessment of the (1) level of proteinuria; (2) active urinary sediment (pyuria, hematuria, and red cell casts), and (3) renal function [serum creatinine (sCr) level and/or glomerular filtration rate (GFR)]3.
Although the level of proteinuria is considered an important measure to document improvement in LN, the recovery time from abnormal levels of proteinuria has not been well described with standard of care treatment in observational studies. Indeed, in daily clinical practice, rheumatologists rely on the level of proteinuria to evaluate the response to treatment. Moreover, in clinical trials response in proteinuria has been a primary outcome.
The objectives of our study were to determine (1) the time to recovery from proteinuria in patients with LN receiving standard of care treatment, (2) whether the initial level of proteinuria predicts improvement and the time to improvement, and (3) factors associated with proteinuria recovery.
MATERIALS AND METHODS
Patients
Patients were identified from the prospective longitudinal Toronto Lupus cohort followed from 1970 until 2011. Patients had SLE [4 or more American College of Rheumatology (ACR) criteria or 3 ACR criteria and a typical biopsy lesion of SLE]. All patients have been followed prospectively at the University of Toronto Lupus Clinic4,5. Collection, storage, and use of clinical and laboratory data on patients followed at the clinic are conducted in accordance with the Declaration of Helsinki and are approved by the Research Ethics Board of the University Health Network, Toronto, Canada. Signed informed consent was obtained from all patients.
Patient assessment
Patients attend the lupus clinic at 2-month to 6-month intervals regardless of the state of activity of their disease. The standard protocol of patient assessment includes complete history, physical examination and laboratory evaluation, and collection of information on drugs. For this study we analyzed the laboratory/histological results including anti-DNA antibodies, complement levels (C3 or C4), GFR, sCr, high-sensitivity C-reactive protein (HsCRP; available since 2003), erythrocyte sedimentation rate (ESR), serum albumin, total cholesterol, and results of kidney biopsy by the World Health Organization (WHO) classification or the International Society of Nephrology (ISN)/Renal Pathology Society (RPS) classification. Global disease activity was measured at each visit by the SLE Disease Activity Index-2000 (SLEDAI-2K), a valid measure of disease activity in SLE6,7,8. The 24-h urine sample was collected as follows: patients were instructed to empty the bladder in the morning and discard the urine and from that point onward for 24 h, all urine was to be saved in the container. At the end of the 24-h period, the bladder was to be emptied and that urine saved.
Patient selection
Most of the patients with LN in the database of the Toronto Lupus Clinic had a kidney biopsy to confirm their diagnosis. For this study, the first identified episode for active LN for each patient with proteinuria documented by a 24-h urine collection and at least 1 of the urinary sediments (hematuria, pyuria, or urinary casts/red blood cell casts) present and persistent on 2 consecutive visits were identified and analyzed. Urine specimens are handled and interpreted by 1 laboratory and the appropriate measurements of preservation and shipment of the urine samples are applied.
Definitions of outcome measures
Proteinuria was defined as ≥ 0.5 g/24 h, hematuria as > 5 red blood cells/high power field (excluding stone, infection, or other causes), pyuria as > 5 white blood cells/high power field (excluding infection), and casts as heme-granular or red blood cell casts; based on the definitions of SLE Disease Activity Index 2K (SLEDAI-2K)7,8. We mandated the presence of active urinary sediments to ensure that the selected patients for analysis did have active LN. Proteinuria and active urinary sediments are recorded and scored in our database only if they are attributed to SLE activity. Thus, in cases where proteinuria and/or pyuria/hematuria/casts are present but not attributed to SLE activity, this will not be scored as present and therefore not contribute toward the renal component of SLEDAI-2K. The interpretation for the urine analysis is based on the physician’s judgment and his/her interpretation of the available laboratory and pathologic results of the urine analysis, urine culture, and kidney biopsy. In difficult situations, kidney biopsies are repeated along with the appropriate investigations to determine whether there is ongoing active disease leading to proteinuria or whether the proteinuria results from damage. We studied the extrarenal manifestations of SLE in this group of patients based on SLEDAI-2K. SLEDAI-2K is based on the presence of 24 descriptors in 9 organ systems7. We also separated the baseline patients’ characteristics by the subgroups of responders and nonresponders to therapy.
Study design
The “baseline visit” for the study was the onset of proteinuria. Based on the baseline proteinuria level, patients were grouped into group 1, having 0.5–0.9 g/day; group 2, 1–1.9 g/day; and group 3, ≥ 2 g/day. Each patient contributed once toward the analysis. Every patient had a baseline 24-h urine sample.
Study endpoints
The recovery from proteinuria was defined as proteinuria < 0.5 g/day8. The “end of study” was the recovery from proteinuria or last clinic visit available in the database in 2011. In the absence of a 24-h urine sample for the determination of recovery, dipstick or spot urine creatinine ratio were used. Two consecutive visits had to be completely free from proteinuria for recovery to be identified. Recovery was then identified as of the first date when proteinuria was absent.
Treatment
Patients were treated with standard of care as determined by the treating rheumatologist (Table 1).
Characteristics of patients at start of study (onset of proteinuria). * Results for nominal data are n (%), and for continuous data in mean ± SD.
Study analysis
Descriptive statistics were used to describe the characteristics of the patients (mean ± SD for continuous data, and frequencies for nominal data). For each of the SLEDAI-2K organ systems, the percent of patients who were active was evaluated separately for each of the 3 baseline protein levels and compared using Mantel-Haenszel chi-square. This was done for SLEDAI-2K at study start as well as study end.
Kaplan-Meier curves were used to compare the time to recovery for baseline proteinuria level as well as other possible risk factors. We studied the following variables as potential risk factors: ethnicity, sex, age at start of study (< 30, 30–50, and ≥ 50 yrs), SLE duration at start of study (< 5 and ≥ 5 yrs), SLEDAI-2K (4–10 and ≥ 11), anti-DNA antibodies (positive and negative), complements (C3 and/or C4; normal, low levels), kidney biopsy [biopsy class by ISN/RPS or WHO: III, IV (or IV and V), and V], GFR (≥ 60, < 60 ml/min/1.73 m2), sCr (> 140 μmol/l), HsCRP (≤ 3 and > 3 mg/l), ESR (female: normal ≤ 20 mm/h and high > 20; male: normal ≤ 15 and high > 15 mm/h), serum albumin (≥ 35 and < 35 g/l), total cholesterol (≤ 5.2 and > 5.2 mmol/l), use of medications [steroids, immunosuppressant, antimalarial, azathioprine (AZA), mycophenolate mofetil (MMF), cyclophosphamide (CYC), methotrexate (MTX), steroids, antihypertensive drugs, angiotensin-converting enzyme inhibitors and/or angiotensin II receptor blockers, antihyperlipidemic agents or statins].
The Kaplan-Meier curves were compared using the Wilcoxon test because it places more emphasis on earlier differences. In the analysis using the Kaplan-Meier curves, the maximum length of followup used was 5.5 years. Therefore, if a patient was still unrecovered at this point, even if recovery occurred at a later date, the time to event was cut off at 5.5 years and the observation would be classified as “censored”. Survival analysis was used to determine the association of potential risk factors and time to recovery.
A proportional hazard model with stepwise selection was constructed including the covariates from the Kaplan-Meier analysis with p < 0.1 in addition to age, sex, ethnicities, and baseline proteinuria levels. We constructed models using all available visits and repeated it censoring at the 5.5 years mark, as was done in the Kaplan-Meier analysis. A second model was run where all of the followup information available was used until 2011. The analysis was conducted using SAS (9.2), and p values < 0.05 were considered statistically significant.
RESULTS
Patient characteristics
Two hundred twelve patients (84% female) who had proteinuria documented with a 24-h collection and active urinary sediment were studied (Table 1). Among the 212 patients, 98 (46.2%) were inception patients who have been followed in the Lupus Clinic since within 1 year of their onset of SLE. In this group of 98 patients, 43 presented at clinic with proteinuria. The mean disease duration for all patients was 5.7 ± 6.3 years at the start of study (onset of proteinuria). In our clinic, steroids plus immunosuppressive (AZA, MTX, and MMF) have been primary therapy for LN with only a minority of patients being treated with CYC9. In the first year following onset of proteinuria, 208 (98.1%) of the patients were taking steroids, 107 (50.5%) were taking antimalarial drugs, and 169 (80.1%) were taking immunosuppressives (118 AZA, 14 MTX, 31 CYC, and 56 MMF). In the first 2 years from proteinuria onset, 208 (98.1%) were taking steroids, 116 (54.7%) antimalarial drugs, and 178 (83.9%) immunosuppressants.
In patients who recovered their proteinuria at last visit compared to those who did not recover, no statistically significant or clinically relevant difference was found in their baseline characteristics (Table 2). The extrarenal manifestations did not differ in patients who recovered their proteinuria at last visit compared to those who did not recover (Appendix 1).
Characteristics of patients at start of study in responders and nonresponders. Start of study is onset of proteinuria. Responders are patients with < 0.5 g/day of proteinuria at last visit and nonresponders are patients with ≥ 0.5 g/day of proteinuria. Results for nominal data are n (%), and for continuous data, mean ± SD.
The mean length of followup period to protein recovery or last clinic visit for the 212 patients was 2.3 ± 2.7 years (median 1.2 and range 0.2–15.4) and 2.0 ± 2.1 years in the group of 128 patients who recovered (median 1.2 and range 0.2–11.1). The length of followup in 84 patients who had not recovered at last clinic visit was 2.7 ± 3.3 years (median 1.4; range 0.2–15.4; Table 1). Among the 212 studied patients, kidney biopsy was available on 150 patients. The mean time between onset of proteinuria and biopsy was 1.8 ± 2.9 years (median = 0.4 year). The results were as follows: class III, n = 29; class IV or IV + V, n = 69; and class V, n = 26 (Table 3). The activity index of the biopsies was 5.66 ± 4.17 (median 5.0) and the chronicity index was 2.20 ± 2.39 (median 2.0).
No. patients in each class by WHO and ISN classification.
Disease activity
SLEDAI-2K was 17.0 ± 6.7 at the start and 8.0 ± 7.1 at the end of the study (Table 1). Patients’ extrarenal manifestations at the start and end of the study are represented in Appendix 1 and 2. There was no statistically significant difference in the distribution of the majority of the 9 organ systems of SLEDAI-2K among patients at the start and end of the study when we compared the patients based on their baseline level of proteinuria. With higher levels of proteinuria, there was a trend toward an associated increase in vascular involvement and constitutional manifestations at the start of the study (p = 0.07 and 0.02, respectively; data not shown). At last visit, patients who did not achieve a proteinuria recovery continued to have active disease with a SLEDAI-2K of 13.0 ± 7.9 compared to a SLEDAI-2K of 4.6 ± 3.7 in patients who recovered (p < 0.0001; Table 2).
Laboratory results
The mean sCr was 102 ± 77 μmol/l (median 83; (normal ≤ 100 μmol/l; 33.5% had sCr > 100 μmol/l, and 5.7% patients had sCr > 200 μmol/l). Of the 212 patients, 145 had eGFR ≥ 60 ml/min/1.73m2. The majority of the patients were serologically active with 66.7% of patients having positive anti-DNA antibodies while 62.4% and 45.8% had low C3 or C4 levels, respectively (Table 1).
Kaplan-Meier estimator for proteinuria recovery based on proteinuria level and potential risk factors
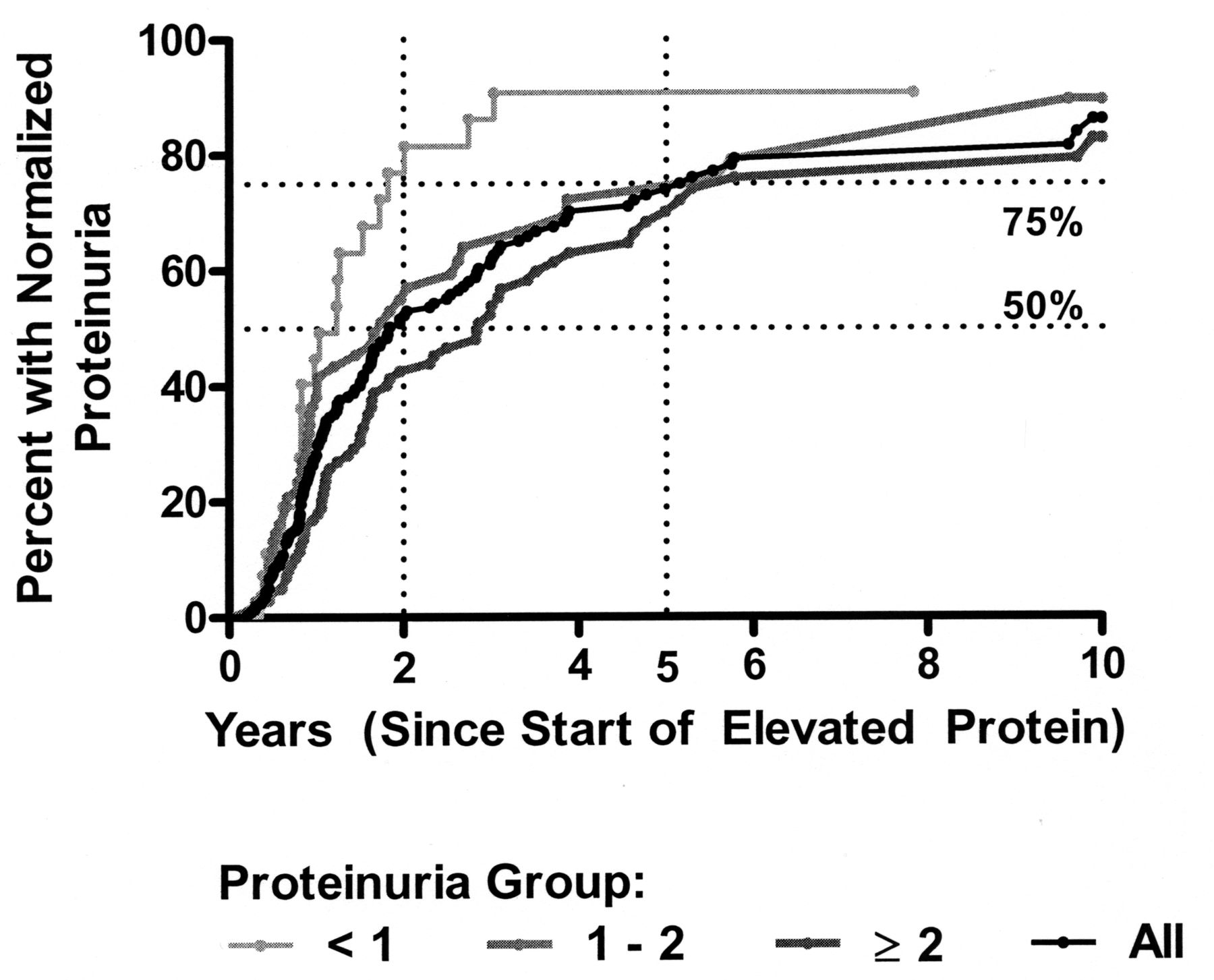
Patients with ≥ 2 g/day had the longest time to recover to normal levels of proteinuria as compared to the other 2 groups at 1 and 3 years.
In the analysis with all 212 patients, 52% of the patients recovered from proteinuria within 2 years and an additional 22% (for a total of 74%) recovered within 5 years (Table 4). The level of proteinuria at baseline visit predicted the time to improvement. Patients with higher proteinuria levels had a lower likelihood of complete recovery (77% vs 55% vs 43% recovery at 2 yrs for patients in group 1 vs 2 vs 3 and 91% vs 72% vs 70% at the 5-yr mark for the same patient groups; p = 0.003; Figure 1). The number of patients and mean time until recovery for patients who achieved it within 5 years was group 1 (n = 21/30), 1.19 ± 0.73 years; group 2 (n = 41/74), 1.24 ± 0.94 years; and group 3 (n = 56/108), 1.84 ± 1.24 years (p = 0.004). Beyond 5 years a total of 10 additional patients recovered completely as follows: in group 2, 3 patients were identified and in group 3, 7 patients.

Kaplan-Meier curve for time to recovery from proteinuria in all patients and in 3 groups.
Percentage of patients who recovered over 5 years.
In clinical practice, physicians are most concerned about nephrotic range proteinuria (> 3.5 g/day) vs non-nephrotic range; thus further analysis was performed. We studied patients in group 3 and divided them into 2 groups: ≥ 2 but ≤ 3.5 and > 3.5 g/day. This analysis showed that the patients in the nephrotic group with proteinuria > 3.5 g/day did not have worse outcome compared to the patients with ≥ 2 but ≤ 3.5 g/day (Table 5).
Percent of patients who recovered over 5 years.
Increased time to recovery of proteinuria was associated with presence of low complement (p = 0.01). Borderline results were also found with increased disease duration at study start being associated with longer time to recovery (p = 0.12; Table 6).
Percent survival rates by risk factors (from Kaplan-Meier modeling).
The percentage of patients who recovered was almost equal in negative anti-DNA compared to positive (31% vs 28% at yr 1 and 79% vs 71% by yr 5; p = 0.20), but was greater in those with normal complements compared to those with low complement levels (36% vs 25% at yr 1 and 84% vs 68% by yr 5; p = 0.01; Table 6).
Prediction models using a proportional hazard model with stepwise selection
In this analysis we included the following covariates selected a priori: ethnicity (white vs all others), age (< 30, 30–50, ≥ 50 yrs), sex, and proteinuria group. Risk factors selected from the results of the Kaplan-Meier analysis were disease duration (< 5 yrs ≥ 5 yrs), and complement levels (normal, low). In the first model, patients were censored at the 5.5-year timepoint.
Normal complement levels (C3 or C4; HR = 1.83) and SLE disease duration < 5 years (HR = 1.74) at the time of development of proteinuria were associated with an increased chance of proteinuria recovery, as were lower levels of proteinuria. Patients in group 1 had an HR of 2.96 to achieve recovery of proteinuria in 5 years and group 2 had HR of 1.54.
A second model was run using all the followup information available. In addition to the previously listed covariates, females had a higher likelihood of achieving recovery in proteinuria (HR = 1.69; Table 7).
Final results of the prediction models, using categorical values.
DISCUSSION
Quantification of proteinuria is essential for monitoring renal disease activity in patients with LN and an important measure of improvement and flare in LN. The definition of partial and complete remission in previous studies is based on a decrease in baseline proteinuria levels. Previous studies have shown that partial and complete remission in diffuse lupus glomerulonephritis is associated with a significantly better prognosis and patient survival, as compared to patients with no remission10,11. The patient survival at 10 years was 95% for complete remission, 76% for partial remission, and 46% for no remission10. The patient survival without endstage renal disease at 10 years was 92% for complete remission, 43% for partial remission, and 13% for no remission10.
In daily practice, rheumatologists face a number of challenging questions in the management of LN. The goal of our study was to determine the recovery time of proteinuria using 24-h urine protein samples. We have shown that 28% of the patients, regardless of the baseline proteinuria levels, had complete recovery (< 0.5 g/day) after the first 12 months of standard of care treatment. The number of patients with complete recovery in proteinuria increased to 52% by 2 years and reached 74% by Year 5. Standard of care treatment included steroids plus immunosuppressives (AZA, MTX, and MMF), with only a minority of patients being treated with CYC. Urowitz, et al showed that use of CYC made no difference in the outcomes of death, renal failure, reversal or relapse of active renal disease, or toxicity9.
Our study showed that the tempo of recovery from proteinuria in LN on standard of care treatment is slow and it is very important not to change the treatment regimen at an early stage. In our center, patients who do not show improvement in their proteinuria levels after 6 months of treatment are eligible for a change in therapy. The ACR recommends that patients with ISN Class III/IV be followed for 6 months after initiation of induction treatment with either CYC or MMF before making major changes in treatment other than alteration of glucocorticoid doses, unless there is clear evidence of worsening at 3 months (50% or more worsening of proteinuria or serum creatinine; level A evidence)12. Grootscholten, et al showed that after 8 weeks of induction treatment with either CYC or MMF, patients with LN who showed ≥ 25% reduction in proteinuria and/or normalization of C3 and/or C4 serum levels were likely to show good clinical renal responses13.
Our second research question was to determine whether the level of baseline proteinuria predicted the time to complete recovery in proteinuria. We have shown that the higher the level of proteinuria at baseline, the longer the time needed to achieve a complete recovery in proteinuria on standard of care treatment. Patients with higher proteinuria levels had a lower likelihood of complete recovery at the 2-year and 5-year marks. These results can be translated into daily practice and help in physician decision making about the appropriate time to consider strategic treatment adjustment, including the decrease in the prednisone dose in response to treatment or modification of immunosuppressants in nonresponders.
In our study we showed that normal complement levels were associated with a higher probability of achieving complete recovery in proteinuria as compared to low complement levels. Nieves-Plaza, et al, showed that low C4 levels were predictors of an earlier decline in renal function as determined by GFR14. Further, our analysis showed that males had lower probability of achieving complete remission of proteinuria than female patients. Previous studies suggested that there are major clinical differences between male and female patients with SLE, with men more likely to have experienced renal damage15. Risk factors for death from SLE were male sex, age > 40 at disease onset, active nephritis, a reduction of sCr clearance, heart disease, and central nervous system disease at SLE onset16. Other studies indicated that patients developing LN after 3 years are defined as having late LN2. Among patients who developed LN after 3 years, age at diagnosis was the only significant predictor of late development of LN2. In our study we showed that the development of late LN with proteinuria, in particular with disease duration ≥ 5 years at the onset of proteinuria, increased the risk of not achieving recovery of proteinuria.
In clinical trials and observational studies the percentage of patients who achieve a complete recovery in proteinuria is dictated by several factors. First, the definition of proteinuria itself varied between studies and centers, and the lower the bar is set for normal 24-h proteinuria improvement, the lower the percentage of complete recovery in proteinuria. The results of a recent metaanalysis on randomized clinical trials for induction treatment of LN with MMF and CYC showed that overall, 11% of the patients achieved complete remission at 6 months3. Second, the study length needs to ensure that enough time is being given to achieve complete renal remission. Previous studies have shown some patients might achieve complete remission during or after the induction period, while other patients achieve remission during the maintenance treatment or not until ≥ 12 months3.
Our study had limitations. First, the diagnosis of LN is usually based on the results of kidney biopsy and abnormal laboratory results in almost all patients. In 43% of the patients a kidney biopsy was not available at the baseline visit; however, we mandated the presence of active urinary sediments to ensure that the selected patients demonstrated active LN. We included patients with proteinuria and active urinary sediments on 2 consecutive visits. This approach excluded 20 patients with pure class V LN with bland urine sediment on whom further analysis is not provided. Second, in our study patients were divided into 3 groups based on proteinuria level instead of considering proteinuria as a continuous variable. We would like to emphasize that the levels of proteinuria chosen were based on clinical significance to the practitioner. Many would consider 500–1000 mg mild proteinuria and 1–2 g would be considered moderate proteinuria. Greater than 2 g cutoff has been adopted in non-nephritis SLE trials to randomize the patients in different groups17. Thus we have chosen these 3 levels (0.5–0.9 g; 1–1.9 g; ≥ 2 g). The third limitation in our study is that the effect of each of the immunosuppressants, its different doses, and combination were not studied. In our study, in the presence of proteinuria and absence of kidney biopsy, the urine sediment was used to indicate LN activity. We understand that the interpretation of urine sediment is highly dependent on the laboratory methods and the readers and this can be variable. Nevertheless, the attribution of urine sediments to SLE disease activity in our clinic is based on the physician’s judgment, and this approach could have helped improve the specificity of the tests.
Twenty-eight percent of the patients with LN normalized their proteinuria at Year 1 and 52% at Year 2. Others continued to improve over time, with 74% recovering at Year 5. The level of proteinuria at baseline visit predicts the time to improvement. Male sex, hypocomplementemia, high level of proteinuria at diagnosis of LN, and disease duration ≥ 5 years at onset of LN, each independently decreased the likelihood of recovery. Physicians should be aware of these factors when managing LN.
Acknowledgment
We acknowledge Rebecca Smith and Jonathan Ding, medical students with the University of Toronto, for the extraction of the data from the charts.
APPENDIX 1.
Extrarenal manifestations by systems in all 212 patients at baseline visit and end of study.
APPENDIX 2.
Extrarenal manifestations by systems in responders and nonresponder patients at baseline visit and end of study.
Footnotes
-
Dr. Zahi Touma is a recipient of the Great-West Life, London Life and Canada Life Fellowship.
- Accepted for publication November 13, 2013.








{kind=link}