

Abstract
Objective. To compare health status, effect on family, occupational consequences, and quality of life (QOL) 1 year after an accident between patients with whiplash versus other mild injuries, and to explore the relationship between initial injury (whiplash vs other) and QOL.
Methods. This was a prospective cohort study. The study used data from the ESPARR cohort (a representative cohort of road accident victims) and included 173 individuals with “pure” whiplash and 207 with other mild injuries. QOL at 1-year followup was assessed on the World Health Organization Quality of Life questionnaire. Correlations between explanatory variables and QOL were explored by Poisson regression to provide adjusted relative risks, with ANOVA for the various QOL scores explored.
Results. One year post-accident, more patients who had whiplash than other casualties complained of nonrecovery of health status (56% vs 43%) and of the occupational effect of pain (31% vs 23%). QOL and posttraumatic stress disorder (PTSD) were similar in the 2 groups. Impaired QOL did not correlate with whiplash when models were adjusted on sociodemographic variables and history of psychological distress. Whatever the initial lesion, PTSD was a determining factor for poorer QOL.
Conclusion. Sociodemographic factors, preaccident psychological history prior to the accident, and PTSD were the main factors influencing QOL, rather than whether the injury was whiplash. PTSD may also be related to pain.
Whiplash is the most frequently sustained injury in road accidents. While generally graded as a minor lesion (AIS-1) on the Abbreviated Injury Scale (AIS)1, it may nevertheless cause lasting disability. Many studies have reported a risk of persistent symptoms, described as whiplash-associated disorder (WAD) and defined by the Quebec Task Force as residual pain persisting 6 months or more after the accident, impairing neck mobility and everyday activity2; this may affect up to 74% of the injured 1 or even 2 years after the accident3.
A large number of studies have addressed whiplash injury. The consequences of whiplash have been widely documented4,5,6,7; for example, 1 study specifically found that 25% of whiplash casualties reported an effect on leisure activity and everyday quality of life (QOL)8.
Several metaanalyses have sought to identify factors leading to longterm symptoms6,7,9,10,11,12. Longterm consequences are commonly considered to depend on primary lesion variables and also on sociodemographic, cultural, and psychobehavioral factors11,13. The psychobehavioral factors, however, remain controversial14,15,16,17, particularly regarding the role of compensation in WAD. Psychological distress (in general) appears to be associated with WAD; some consider it specific to whiplash casualties, physical pain coming to be seen as a consequence rather than the cause of the distress12. Conversely, other authors15 argue in favor of whiplash pain being the cause, with psychological distress being only a consequence. The specificity of whiplash, however, may be questionable: there have been few comparative studies with other injuries of comparable severity. Perhaps other types of mild accident injuries may impair quality of daily life, but are not recognized as doing so.
One of the most interesting concepts measuring effect on daily life is QOL, which takes into account the complexity of the subject’s self-perception in the physical, psychological, social, and environmental domains of life18. Few studies have evaluated QOL in patients with whiplash, and those few results were not consistent: Rebbeck, et al found QOL to be systematically lower in whiplash casualties than in an Australian reference population19; Meerding, et al20, in contrast, found that QOL in nonhospitalized whiplash casualties was very close to general population levels 2 months after the accident; Polinder, et al21 reported that other nonhospitalized mild injury casualties in the Netherlands had recovered a general population QOL level by 5 months, whereas this was not the case for whiplash casualties; likewise, Versteegen, et al22 reported significant differences on various Medical Outcomes Study Short Form-36 questionnaire dimensions between neck-sprain casualties and a reference group, although this survey was limited by an elevated nonresponse rate (63%).
The ESPARR Cohort (Etude et Suivi d’une Population d’Accidentés de la Route dans le Rhône) included 1168 road-crash casualties23 from the moment of the accident and 5 years’ followup; it provides a good opportunity to explore the specificity of whiplash and its consequences for QOL. The primary objective of our present study was to compare the various consequences of a mild accident at 1 year of followup in terms of symptomatology, and familial, social, and occupational disturbances, and the effect on QOL between whiplash casualties versus other mild injury casualties. The secondary objective was to determine whether whiplash is a prognostic factor for poorer QOL at 1 year after the accident.
MATERIALS AND METHODS
The ESPARR cohort
The inclusion period lasted from October 2004 to December 2005, with the cooperation of all the emergency, secondary, and intensive care units of the Rhône administrative department in France. After initial assessment at the time of the accident, patients were offered followup at 6 months and 1, 2, 3, and 5 years. Further details on recruitment methodology are to be found in a previous report23. The ESPARR cohort constitutes a subpopulation that has been shown to be representative of the road-accident casualties in the Rhône Registry of Road Crash Trauma; this registry has recorded all road accident casualties who consulted in or were admitted to any of the hospital departments in the Rhône department since 199523,24.
The total cohort comprises 1168 adults (aged 16 years or over). At inclusion, the registry’s experienced physician codes all lesions according to the Abbreviated Injury Scale (AIS) criteria1, working from the initial medical records, which cover symptomatology, clinical, and biological examination results and imaging where judged necessary. Each elementary lesion is thus coded, as is severity on a scale from 1 (minor) to 6 (maximal).
Study population
Our present study selected the 548 adults in the ESPARR cohort who had sustained only mild injury, defined as a maximum AIS grade 1 (MAIS1), excluding cases of 1 or more associated AIS ≥ 2 lesions in different body regions; 255 of these subjects had sustained whiplash injury and the other 293 had any other type of MAIS1 lesions, such as an ankle or shoulder sprain, superficial wounds or contusions, tendon tear, and others. In all, 380 subjects (69.3%) responded to the 1-year followup questionnaire: 173 of the 255 whiplash cases (68%) and 207 of the 293 other mild injury casualties (70.6%; Figure 1).
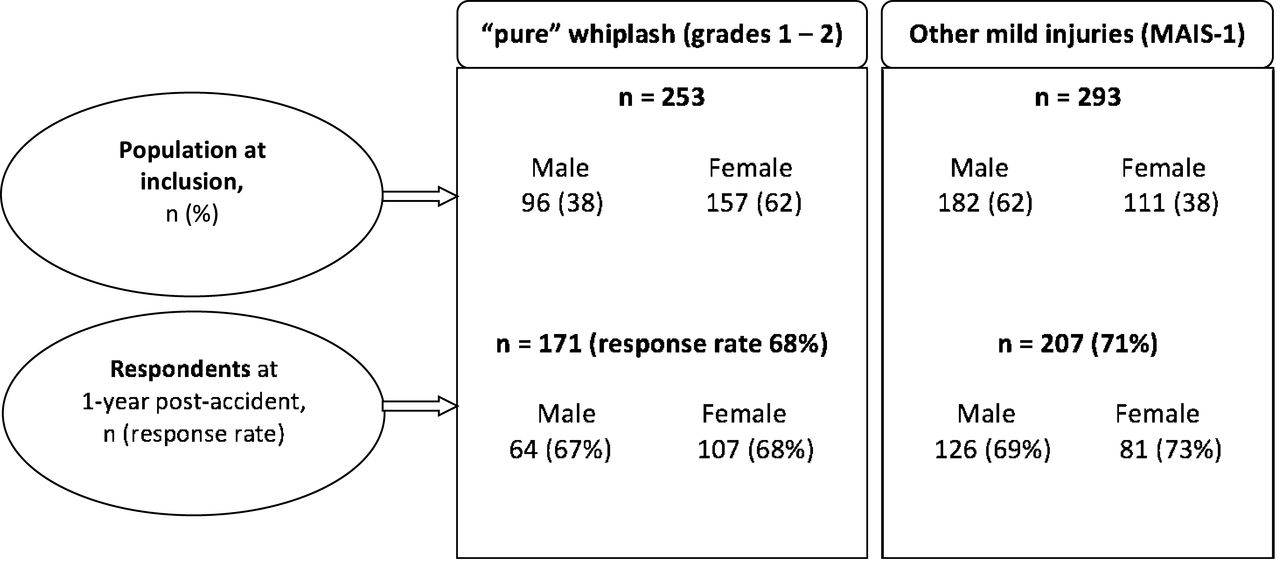
Response rate at the 1-year followup by sex and type of population. MAIS1: maximum Abbreviated Injury Scale grade 1.
Clinical definition of the whiplash group
In our present study, all subjects with lesions classified as cervical contusion (AIS code 310402) or neck sprain (AIS code 640278) were considered whiplash casualties. Diagnosis was made by physicians at the outset of hospital care, based on interviews, clinical findings, and radiographs. In the AIS classification, Code 310402 is attributed to neck pain following a road accident with painful neck on palpation, without other objective signs; Code 640278 is attributed to neck pain associated with cervical stiffness and radiologic loss of cervical lordosis.
Initial AIS grades were compared to Quebec Task Force categories2, a standard classification universally used for whiplash, comprising 4 cervical distortion severity grades: grade 1, simple contusion; grade 2, neck sprain; grade 3, cervical symptomatology with associated neurological abnormality (such as impaired tendon reflex or motor and/or sensory impairment); and grade 4, clinical signs of major structural pathology involving severe osteoarticular lesions (fracture or dislocation). The consultation reports of 40 ESPARR subjects were reviewed and classified on the Quebec system. Comparing the 2 classification methods found perfect agreement in all cases, so that transposition between the 2 was judged licit. In what follows, the distribution for all subjects is reported in terms of the Quebec classification.
Cervical spine lesions graded AIS-1 (code 640278) but with associated neurologic abnormality (n = 2; Quebec grade 3) were excluded, bringing the number of subjects included to 171, comprising 62 grade 1 and 109 grade 2 injuries.
Variables and measurement tools
The World Health Organization Quality of Life tool (WHOQOL-BREF)18 was used to assess QOL. It has been shown to have good psychometric properties and validity25,26, including in its French-language version27. It comprises 26 questions: 2 independent items assessing QOL and health satisfaction, and 24 exploring 4 dimensions (physical, psychological, social, and environmental). Responses to each question are on a 5-point Lickert scale, quantifying intensity, capacity, frequency, or an assessment, and weighted by an algorithm to calculate “profile” scores28 (scale 0–100 to be congruent with the generic WHOQOL questionnaire). The different variables describing the QOL are the outcome variables (dependent variables). For analysis, whiplash status (no whiplash/grade 1/grade 2) was the explanatory variable of interest. Other explanatory variables, collected during the inclusion interview immediately after the accident, were tested as possible predictive factors: (1) sociodemographic factors (sex, age, family situation, educational level); (2) accident-related factors (type of road and user, reason for travel, position in vehicle, antagonist, impact direction, responsibility in accident, intention to lodge a complaint, presence of an injured friend or family member); (3) preaccident financial problems (job loss, financial difficulties, failure, etc.); and (4) preaccident psychological history (sleep disorder, use of antidepressants/ anxiolytics, psychological treatment).
Consequence-related factors collected at 1 year were then added to be tested as associate factors: time off work; posttraumatic stress disorder (PTSD), assessed on the PTSD Checklist Scale, with scores ≥ 44 indicating probable PTSD29,30; debilitating physical pain (item 3 of the WHOQOL-BREF); disturbed occupational and leisure activities; and financial repercussions.
Statistics
The representativeness of the study population was assessed by comparing, on the one hand, respondents and nonrespondents at the 1-year followup, and on the other hand, the ESPARR whiplash casualties to the other Rhône registry whiplash casualties. Comparison used chi-squared tests (significance level, 5%), or Fisher’s exact test where samples were too small.
Variables associated with the dependent variable on univariate analysis (at a 10% significance level) were included in a full model, and a descending procedure progressively eliminated nonsignificant factors.
Multivariate analysis used 2 approaches. In the first, 2 modified Poisson regression models31 were constructed to study the relationship between overall QOL or health status and whiplash status (no whiplash/grade 1/grade 2) and to explore for other predictive factors; QOL and health status were expressed as dichotomous variables: good/very good versus neither poor nor good/poor/very poor quality of life; and satisfied/very satisfied versus neither satisfied nor dissatisfied/very dissatisfied with health status.
In the second approach, scores on the 4 WHOQOL domains were each introduced in an ANOVA to assess the relationship between whiplash grade and QOL and to explore for predictive factors for impaired QOL in the 4 domains. The validity (linearity, normal distribution, residual equal statistical variance) of the model constructed by residual analysis was checked.
In the next step, consequences observed at the 1-year followup and significant at the 10% level on univariate analysis were introduced in each final predictive model, to explore consequences associated with QOL. Because of a strong correlation between pain and PTSD (p < 0.0001), only the latter was introduced in the final models. In all models, age and sex were included, independently of their significance level, as adjustment variables.
Analysis was performed on the PROC GENMOD and PROC GLM procedures of the SAS 9.3 software package.
Informed consent was obtained from all subjects. The study was approved by French committees concerned with ethics and medical information.
RESULTS
Representativeness of the population
One hundred seventy-one of the 253 subjects with whiplash (67.6%) responded at 1 year; the response rate was similar for the non-whiplash population (71%; Figure 1). For both groups, there were no significant differences in inclusion criteria or accident-related factors between respondents and nonrespondents.
Further, neither group differed from the MAIS1 road-accident registry population in age, sex, type of road user, or reason for travel.
Whiplash grade 1 subjects had a lower response rate (64%) than whiplash grade 2 subjects (70%).
Comparison of the circumstances of the accident
Comparing the whiplash population as a whole and the non-whiplash population showed several differences: the whiplash population was more frequently female, driving a 4-wheel motor vehicle, in collision with another motor vehicle, and sustaining a rear impact; whiplash casualties also more frequently considered themselves not responsible for the accident (Table 1).
Description and comparison of the 2 MAIS1 populations (whiplash and non-whiplash victims), at 1 year after road accident.
Comparison between the 2 grades of whiplash showed no differences except for type of user: grade 2 whiplash casualties were more often 4-wheel motor vehicle users (p = 0.03).
Health status and consequences for everyday life at 1 year
At 1 year post-accident, more than half of the persons with whiplash injuries reported that their health status was not back to normal (Table 2), a significantly greater rate than for those with non-whiplash injuries; half of the patients with whiplash (vs 45% of non-whiplash cases) reported physical pain that was debilitating in daily life, and a quarter said they needed medical care to manage daily life. Seventy-nine percent of whiplash casualties claiming not to have recovered good health had debilitating pain at 1 year, compared to 13% of those reporting full recovery; 48% vs 5% reported headache, 34% vs 7% vertigo, 34% vs 4% memory disorder, and 33% vs 4% sensitivity to noise.
Descriptive analysis of consequences for whiplash and non-whiplash victims, at 1 year after road accident.
The whiplash and non-whiplash populations did not significantly differ in frequency or duration of sick leave. Emotionally, the percentage of subjects reporting frequent negative feelings was similar in the 2 groups (whiplash, 23%; non-whiplash, 22%). More than 14% of the whiplash population developed PTSD; this percentage was not significantly different in the non-whiplash group (11.1%).
Ten percent of the persons with whiplash who worked at the time of the accident had not gone back to work at 1 year, either being still on sick leave or having lost their job, compared to 13% in the non-whiplash population (nonsignificant).
In general, however, persons with whiplash claimed that the accident had a significantly greater effect on their finances and work than did persons with non-whiplash injuries (Table 2). Disturbance of leisure, on the other hand, was the same in the 2 groups (26%).
Comparing the 2 grades of whiplash showed some significant differences: grade 2 casualties had longer sick leave (p = 0.05), and were more likely to report disturbed occupational activity (p < 0.01). Other consequences were not significantly different.
QOL at 1 year of followup
Whiplash did not correlate overall with dissatisfaction with QOL or health at 1 year after the accident (Table 3); the physical QOL domain, however, scored significantly lower in cases of whiplash (p < 0.01). Comparing the 2 grades of whiplash, scores for whiplash grades 1 and 2 were not statistically different, except for the mental score, which was significantly lower in whiplash grade 1 than 2 (p = 0.01).
Quality of life (WHOQoL-Bref) for whiplash and non-whiplash victims, at 1 year after a road accident.
Predictive factors for poorer QOL
Lesion type did not emerge as a factor predictive for impaired QOL or health after adjustment on the other variables (Table 4). Certain demographic and socioeconomic factors, however, were relevant: sex (women being less satisfied with their health status), educational level, preaccident financial problems, and age (those over 35 years being less satisfied with their QOL). Intending to lodge a complaint just after the accident was predictive of unsatisfactory health status at 1 year (RR 1.60; 1.13–2.26).
Predictive factors for a poor quality of life and for an unsatisfactory state of health and whiplash and other factors (Poisson modified regression, adjustment on age, sex).
When PTSD was entered in the previous models, however, it emerged as the major factor associated with unsatisfactory QOL, with a 2-fold greater risk of subjects being dissatisfied with their QOL (RR 2.37; 1.84–3.06) or health (RR 2.30; 1.78–2.96); in parallel, the intention to lodge a complaint ceased to feature in the models.
Analysis of the 4 QOL domains specified predictive factors more precisely in each (Table 5).
Type of lesion and other predictive factors related to the scores on the 4 quality of life (QOL) domains (ANOVA, adjustment on age and sex).
In the physical domain, after adjustment, lesion type no longer featured (p = 0.12). Age, sex, educational level, psychological history, and the immediate intention to lodge a complaint were predictive of a poorer score in the physical domain.
In the mental domain, educational level and psychological history were predictive of QOL. The type of lesion did not correlate with the mental score (p = 0.08), in spite of an apparent decrease in scores (β = −4.70) in whiplash grade 1 subjects.
In the social domain, age, psychological history, and financial problems before the accident were predictive of poor scores. The type of lesion did not explain the social score (p = 0.46).
In the environmental domain, QOL was mainly predicted by psychosocial factors such as educational level and financial problems before the accident. The type of lesion did not explain the environmental score (p = 0.62).
In all 4 WHOQOL-BREF models, when PTSD was introduced in a second step, it correlated strongly with poor scores, with β ranging from −16.33 in the environmental domain to −23.39 in the physical domain, without changing the results concerning the predictive factors observed in the predictive models.
DISCUSSION
Our study compared 2 road accident casualty groups from the ESPARR cohort with mild (MAIS1) injury, 1 with whiplash injury and a reference group with contusion, sprain, or minor wounds to other body regions, to compare the consequences of the accident at the 1-year followup and to search for any specific effect of whiplash on QOL at 1 year after the accident. The main findings were (1) whiplash casualties had a lower rate of recovery of health status at 1 year, especially in regards to persistent pain, and they experienced greater disturbance of occupational activities and greater financial difficulty than did persons with non-whiplash casualties, although there was no difference for PTSD; (2) after adjustment for age and sex, QOL and health status did not correlate with whiplash as the form of injury; (3) psychological history and sociodemographic factors were predictive of poor scores in the various QOL domains, independent of the initial lesion; and (4) PTSD was a more important factor influencing QOL than whether the injury was whiplash, but PTSD correlated very strongly with residual pain at 1 year, so that it is difficult to say which of these 2 factors was causally implicated.
Although the consequences of whiplash have been widely documented4,5,6,7, there have been few comparisons with injuries of comparable severity: Kasch, et al32 showed that individuals with whiplash more often suffered from residual pain and a certain disability at 1 year than did patients with ankle lesions of comparable severity. Symptoms observed at 1 year in patients with whiplash having not recovered are quite similar to the symptoms observed in fibromyalgia. However, like Tishler, et al33, we did not observe differences between the 2 groups of injured. Further, the symptoms could be considered those of hypersensitivity, as reported by Sterling, et al15.
Buitenhuis, et al34 reported an 8% rate of PTSD at 1 year in whiplash casualties followed up after their accident, which was a lower rate than in our study, but agreed with the present finding that chronic pain syndrome at 1 year is associated with PTSD.
At inclusion in our study, persons with whiplash did not more frequently report that they intended to lodge a complaint; nor had they more frequently had prior psychological treatment, indicating that these were not specifically whiplash-related factors, despite widespread reports of a causal link between compensation demands16,17 and/or previous psychological disorder and persistence of whiplash pathology35.
At the 1-year assessment, patients with whiplash or other mild injury did not differ in psychological consequences: PTSD was slightly but not significantly more frequent in the former (14.6%, vs 11.1% in the reference group). Comparison with findings for other specific groups finds comparable PTSD rates: McCauley36, et al found a 12% rate of PTSD in mildly injured patients with light to moderate cranial trauma and a 14% rate in those without cranial trauma; a similar rate (12.6%) was reported by McGregor, et al37 in military personnel with mild injury (of any sort) sustained in Iraq.
In comparison with the general French population38, persons with mild casualties in the ESPARR cohort more frequently reported not having satisfactory or very satisfactory QOL or health. This finding is all the more notable because mean age in those reporting not having satisfactory or very satisfactory QOL or health was lower than in the general population, while these scores usually diminish with age. Like several other reports19,20, our study found that whiplash casualties had poorer QOL than the general population; what is interesting is that a similar trend was observed for the other mild casualties. Comparing QOL in patients with WAD and patients with rheumatoid arthritis (RA), Soderlund and Lindberg4 found higher psychosocial disorder rates in the former. Similarly, Ferrari, et al39 found comparable health-related QOL consequences in patients with WAD and those with RA. These studies, however, focused only on chronic (WAD) cases and not on whiplash cases as a whole.
The fact that intention to lodge a complaint ceased to feature in the model when PTSD was introduced suggests a link between these 2 variables: intention to lodge a complaint may be a sign of early stress, as suggested by many studies that correlated early stress and PTSD.
Strengths and limitations
The ESPARR cohort is a prospective road accident casualties cohort, representative of accidents in a precise geographic area for which a registry of road accident injuries has been operating since 1995, with a high level of exhaustiveness compared to official statistics24,40. Comparison of the injured in the ESPARR cohort and those included in the registry but not in ESPARR showed no selection bias. Moreover, the present 69% response rate was very satisfactory for a postal survey conducted at a 1-year interval. The study population was selected from the ESPARR cohort to include on the one hand only “pure” whiplash casualties without associated lesions, and on the other hand mildly injured subjects without any lesion of the neck or spine, thereby improving the specificity of the correlations observed. Descriptions of initial lesions were collected from medical files (medical and radiological examinations) in all the hospitals participating in the Rhône road crash registry, and each lesion was coded by the physician in charge of coding for the registry independent of recruitment in the cohort, avoiding possible recruitment bias.
The study population was representative of whiplash casualties in general, providing a picture not focused on any particular type of road user or accident variables, nor exclusively on patients consulting for persistent pain, as frequently was the case in previous reports12.
The various questionnaires and the data collection did not specifically target whiplash, because the ESPARR cohort includes all kinds of lesion; this avoided the subjectivity bias phenomenon whereby patients develop more complaints in regions of interest to the investigator, and allowed comparison with a control group with different injuries.
The WHOQOL-BREF is a generic instrument, perfectly adapted for use in both general populations and nonselected patient groups, notably allowing comparison between different types of patient.
Several limitations remain. Despite the good response rate (69%) for a postal survey, there may have been a response bias, as several authors have described41,42. The mildly injured participate less often than the more severely injured, and tend more often to be male. However, for a given severity level (all the present subjects being MAIS1), no difference in age or sex was found between respondents and nonrespondents. Because whiplash casualties were more frequently women, a higher response rate might be expected in the whiplash group because women usually participate better in studies; but this was not the case (67.6% vs 70.4%). However, the present results are unlikely to have been affected by this female predominance in the whiplash group, especially as multivariate analysis adjusted the model on age and sex. But subjects with better QOL may have been less likely to respond, thereby attenuating the difference in QOL between the 2 groups.
There have been some reports of the WHOQOL-BREF lacking sensitivity in certain pathologies43,44, which might impede longitudinal followup of mildly injured populations; the present results, however, showed no such effect. Scores in the injured were lower than in the general French population38,45.
Our present results should be useful in attracting the attention of both clinicians and the public administration to patients at risk of suffering from consequences after a mild accident; in particular, it seems very important to improve awareness and management of PTSD without, however, neglecting the physical burden of whiplash.
In spite of more frequent complaints by persons with whiplash in non-recovered health status and the occupational effects of pain, impaired QOL observed in the mildly injured 1 year after their accident is not predicted by the presence of whiplash lesion, but rather by sociodemographic factors and psychological history. Whatever the initial lesion, posttraumatic stress is a determining factor in impaired QOL. PTSD certainly correlated very strongly with residual pain at 1 year.
Acknowledgment
The authors are grateful to the accident victims for their cooperation in data collection. The authors thank all those who assisted in carrying out this study: Nadia Baguena, Jean Yves Bar, Amélie Boulanger, Elodie Paquelet, Stuart Nash, and Véronique Sotton for collecting the data; Irène Vergnes for organizing the databases; Anne-Marie Bigot, Nathalie Demangel, and Geneviève Boissier for subject database management; Blandine Gadegbeku, Amina Ndiaye, and The Association for the Rhône Road Trauma Registry for their help in collecting and providing medical data; the Scientific Committee (Daniel Floret, François Chapuis, Jean Michel Mazaux, Jean Louis Martin, Jacques Gaucher, and Etienne Javouhey); Dominique Boisson for her participation in the ESPARR scientific management team; and all the hospital staff who accepted the interviewers’ presence and referred persons with injuries. Also thanks to P.P. Vidal and other members of the whiplash consortium of the Road Safety Foundation program. Special thanks go to Iain McGill for comments and manuscript editing.
Footnotes
-
Supported by the French Ministry of Equipment, Transport, Housing, Tourism and Sea (Program Predit 3 “New Knowledge in the Field of Road Safety”: N° SU0400066), from the National Agency for Research (Program Predit “Safe, reliable and adapted transport” No. ANR-07-TSFA-007-01), from the French Ministry of Health (Program PHRC 2003: PHRC-N03 and PHRC 2005: PHRC-N051) and from the Road Safety Foundation (2010/MP/01/).
- Accepted for publication October 17, 2013.








{kind=link}