

Abstract
Objective. Many older patients express concerns about medication risks, and have higher risk thresholds than physicians for cardiovascular preventive medications. We hypothesized that patients have relatively high risk thresholds for fracture preventive medications.
Methods. Women ≥ 60 years old were recruited from 3 primary care internal medicine clinics in Wisconsin. Participants were provided information regarding fracture risks and treatment risks and benefits, followed by a series of vignettes depicting a 70-year-old woman at baseline fracture risks between 5–50%. Fracture risks were shown graphically and treatment side effects were provided for each vignette, and participants were asked to respond regarding whether they would accept treatment. The association of vignette treatment acceptance with participant beliefs regarding medication risks was examined in analyses adjusted for perceived risk of medications, patient numeracy, and prior respondent experience with osteoporosis.
Results. The mean age of women in the cohort was 69.4 years (SD 7.29). Ninety-one percent were non-Hispanic whites, 34% reported a history of fracture, and 20.3% a history of osteoporosis. Subjects varied substantially in their responses to vignettes, but only 51% reported they would accept prescription osteoporosis treatment at the threshold currently recommended by national physician treatment guidelines, and fewer would accept treatment at lower risks. Belief that medications are generally not worth their risks was associated with lower acceptance of treatment at all levels of fracture risk.
Conclusion. There is substantial variability in preferences for postmenopausal osteoporosis treatment. Presentation of individualized fracture risks as recommended by current guidelines has potential to allow better targeting to higher-risk patients, but further work is needed regarding how to present this information and counsel patients.
Physician treatment of osteoporosis has undergone substantial changes over the last 3 decades. From the 1980s to the early 1990s, osteoporosis was primarily diagnosed after patients had fractures. By the early 2000s, randomized trials showed the fracture benefits of treatment for patients with hip bone mineral density (BMD) T score ≤ 2.5 SD below the young adult mean1,2, and treatment of low bone density became widely accepted. In 2008, guidelines by the National Osteoporosis Foundation (NOF) and American Association of Clinical Endocrinologists continued to recommend prescription treatment of patients with hip and vertebral fractures and those with a central dual-energy x-ray absorptiometry (DEXA) T score ≤ −2.5, but also began to recommend treatment of patients with DEXA-based T scores between −2.5 and −1 if they had 10-year hip fracture probability ≥ 3% or major osteoporotic-related fracture probability ≥ 20%3,4.
There are no randomized trials supporting treatment of patients based on fracture risk. This addition to guidelines substantially expands the population of treatment-eligible patients; for example, 72% of white women 65 years and over are eligible for treatment by NOF guidelines5. At the same time, new side effects of oral bisphosphonates, the most commonly used treatment, have been reported, including osteonecrosis of the jaw and atypical femoral fractures. Most of these side effects appear to be rare among patients with osteoporosis6, but the US Food and Drug Administration (FDA) warns that risks probably increase with prolonged use7, and patients and physicians seem to be responding to the warnings. Bisphosphonate use, which rose rapidly to 46.8 million total prescriptions by 2007, dropped by nearly half by 20128.
It is possible that the “ups and downs” of osteoporosis treatments have now led to well-targeted treatment. However, it is more likely that patient fears about medications are reducing treatment among all patients, and thus worsening the already suboptimal9,10 treatment of high-risk patients. There is evidence that side effect concerns reduce preventive medication use by patients at all levels of disease risk. For example, nearly all women reject breast cancer prevention with tamoxifen and raloxifene, with minimal differences by baseline risk11,12. Evidence in other preventive care is weaker, but 1 study found that Canadian patients who had been informed about hypertension outcomes still believed that hypertension treatment thresholds should be higher than their physicians’ recommendations13.
Little is known about how patients perceive fracture risk thresholds, or the contribution of medication risks to their beliefs. As part of a project designed to improve osteoporosis treatment for both high-risk and low-risk patients through decision support, we performed a pilot study of patient perceptions of thresholds for osteoporosis treatment. After presenting extensive information about osteoporosis and its treatments, we used a series of patient vignettes with 10-year fracture risks varying from low to high to examine patient decision making about thresholds for use of oral bisphosphonates. We also examined the potential influence of patients’ perceptions of medication risks upon those decisions.
MATERIALS AND METHODS
Study design overview and population
We examined osteoporosis medication decisions at a range of baseline levels of fracture risk through a study of postmenopausal female primary care patients. An initial questionnaire consisted of Likert-scaled questions regarding experiences with and perceptions of osteoporosis and osteoporosis treatments (questionnaire is available from the author upon request). After being provided information regarding the experience and potential outcomes of osteoporosis and osteoporosis preventive treatments, subjects were also asked to assess a series of hypothetical vignettes with differing fracture risk probabilities, and report their preferences for treatment thresholds.
Following Medical College of Wisconsin Institutional Review Board approval, women were recruited for the study from 3 Milwaukee, Wisconsin, urban/suburban general internal medicine practices in January through May of 2009. Physicians were provided with a list of female subjects ≥ 60 years old who were randomly selected from a list of all subjects seen in the prior 12 months. The cohort entry criteria were designed to target postmenopausal women who are likely to be faced with fracture preventive treatment decision making. Physicians excluded any subjects they judged to have a life expectancy < 1 year. The remaining subjects were sent recruitment letters with a postcard and phone number. Participants were contacted only once. All participants were given the necessary information to make an informed decision about consent.
The educational content of the study was written at a seventh-grade reading level and was pilot-tested for clarity and understandability of graphics and questionnaire questions with 10 subjects. To further ensure that the population could interpret information in English, a registered nurse performed an in-person additional eligibility screen using an English-language brief mental status examination at a study site contiguous to the internal medicine clinics. There were no other restrictions on eligibility. All women were also offered the option of having materials read to them. Subjects who declined that option were provided a written questionnaire to complete in person immediately, with access at any time to a study nurse.
Study content
Initial survey questions included measures of demographics, health literacy14, and numeracy measures15. Personal fracture risk factors (history of fracture, family history of fracture, smoking history, and glucocorticoid use), osteoporosis screening history, dietary calcium intake, nonprescription calcium and vitamin D use, and personal osteoporosis diagnoses and prescription treatments were measured. Subjects were also asked about sources of information about osteoporosis (advertisements, other media, and physicians) and attitudes toward pharmacologic treatments. Women who had osteoporosis were asked to estimate their personal 10-year fracture risk on an open-ended 0–100 scale. Those who did not report osteoporosis were asked to also estimate their personal 10-year risk of developing osteoporosis. All women completed a 3-question numeracy scale15.
The study vignettes consisted of 4 half-pages of descriptive and probabilistic information regarding fractures and fracture prevention followed by 6 hypothetical patient vignettes (Figure 1). The informational pages included definitions of osteoporosis; tests used to diagnose it; its link with fracture; descriptions of functioning, pain, and the risk of mortality after fractures; and descriptions of fracture-preventive medications (indications, benefits, and side effects). Information was drawn from large metaanalyses, randomized trials, or cohort studies16,17,18,19,20,21. Illustrations were used where appropriate. To simplify the presentation, only mean data were presented, and details were provided only for the most commonly prescribed class of osteoporosis medications at the time (oral bisphosphonates).

Sample vignette pictograph of treatment risks and benefits.
The presentation of the 6 vignettes was based on studies in hypertension and breast cancer11,12,13,22. Each vignette asked the subject to imagine that she was a 70-year-old woman whose risk of a broken hip in the next 10 years was n% and risk of other fractures was 4n%. All risks were based on a validated algorithm23 that gives results similar to the World Health Organization’s FRAX risk assessment algorithm24,25,26. The effect of treatment was summarized with the statement, “if you take an osteoporosis medication once weekly, you can reduce your chance of breaking a bone” and was also depicted using 2 pictographs. Each pictograph showed 100 women and their fracture outcomes in next 10 years. The first pictograph showed the risk with no medication and the second the risk with medication. Adverse effects, which were listed in a box next to the pictograph, included stomach upset27,28,29 severe enough to stop therapy (5 or more out of 100 people), osteonecrosis of the jaw27,28,30 (1/100,000), and atrial fibrillation28,31,32 (1/100). The vignettes were displayed in order of increasing risk (1% hip/4% other, 2%/8%, 3%/12%, 6%/24%, 8%/32%, and 10%/40%). Subjects were asked whether they would take the medication (yes/no response).
Analysis
Descriptive statistics were used for questionnaire items regarding demographics, personal history, and factors facilitating or acting as barriers to fracture prevention. We calculated the frequency of acceptance of prescription treatment for the 6 vignettes. For each vignette, we also used logistic regression models to examine the association of several factors with prescription/treatment decisions. Factors of interest included concern about treatment side effects, subjects’ measured or perceived personal osteoporosis risk (personal diagnoses of osteoporosis, older age, and estimates of personal fracture risk), and a measure of patients’ capacity to use numeric risk information (numeracy)33,34.
RESULTS
Invitations to participate in the study were sent to 790 women. A total of 241 completed the study, for a participation rate of 31.0%. Participants were primarily white, and had a range of educational backgrounds and household income levels (Table 1). Sixty-three percent had at least 1 major fracture risk factor other than low bone density (Table 1), including 34% with a personal history of prior fracture. Additional characteristics of the study sample are shown in Table 1.
Subject characteristics (n = 241). Data are percentages, unless otherwise indicated.
Personal osteoporosis history and risk estimates
A minority of subjects reported a personal history of osteoporosis: 49 reported their physician(s) had told them they had osteoporosis, and 39 reported that their BMD test showed osteoporosis (Table 1). Subjects with osteoporosis estimated their 10-year risk of fracture of any kind to be 43%, and subjects without osteoporosis estimated it to be 37%. Women both with and without an osteoporosis diagnosis estimated their lifetime fracture risk to be 50% (SD 33); they estimated the average US woman’s lifetime risk to be 55% (SD 34).
Subjects reported a number of previous information sources and experiences regarding fracture prevention, including 76% who reported that their physician had talked to them about osteoporosis. Eighty-four percent reported their physician had recommended BMD testing, and all but 1 of those reported having the testing. Ninety-three percent had seen some advertising for osteoporosis medications in the prior month, and 54% reported seeing 7 or more advertisements.
Fracture prevention vignettes
Responses to the 6 vignettes are shown in Figure 2. Fewer than half of subjects would accept prescription treatment for the low-risk scenarios where risk was below guideline-based treatment thresholds. Respondents’ acceptance of treatments rose along with hypothetical fracture risk. However, substantial numbers of women would not accept treatment at or above physician guidelines’ thresholds for prescription medication use (vignettes 3–6); over 49% would not accept treatment at a hip fracture risk of 3% and a total fracture risk of 12%, and 18% of women who would not accept treatment even at 50% fracture risk levels.
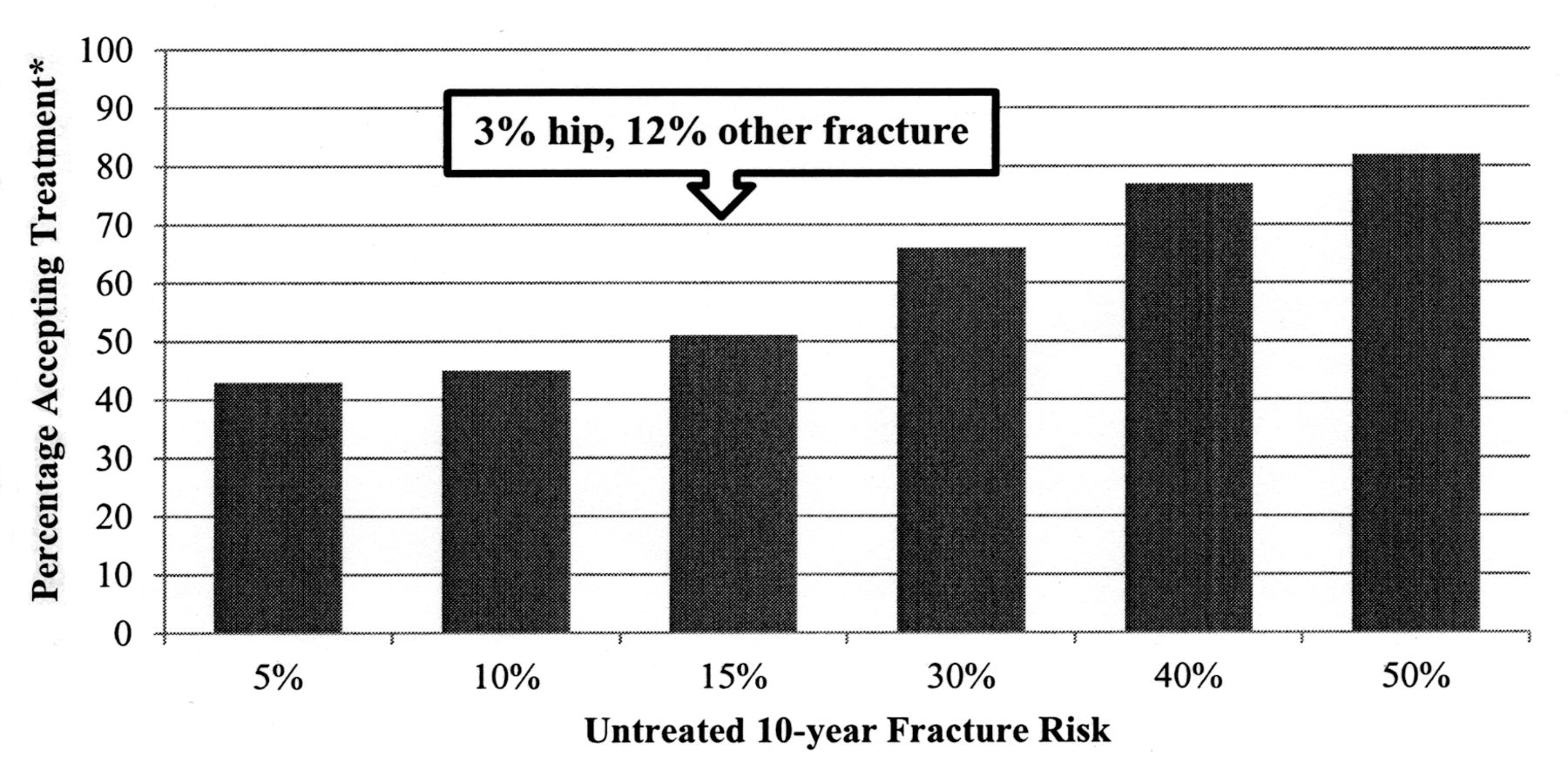
Subjects’ willingness to accept osteoporosis treatment. Percentage of participants who would agree to preventive treatment at each (untreated) 10-year risk percentage. Subjects were given information about fractures/fracture prevention and asked to assume they were a 70-year-old woman with 10-year fracture risks as shown. *Thirty-three percent fracture risk reduction with treatment assumed.
Factors that were associated with acceptance of treatment are shown in Table 2. Subjects who agreed with a statement that treatments are “not usually worth the risks” were less likely to accept treatment for all vignettes. These differences were statistically significant for all vignettes at or above current treatment thresholds (vignettes 3–6). Higher perceptions of fracture risk were associated with higher likelihood of treatment acceptance for all vignettes. A personal history of osteoporosis was also associated with a higher likelihood of treatment acceptance; this was statistically significant for vignettes 1–4. Subjects with high numeracy (2–3 correct on a 3-question scale) were significantly less likely to accept treatment at the lowest risk level (1% hip, 4% other fracture risk). They were actually more likely than those with lower numeracy to accept treatment as risks increased, though the differences were not statistically significant.
Factors associated with osteoporosis treatment (TX) acceptance for patient vignettes at increasing baseline fracture risk.
Importance of risk information
Participants judged both treatment efficacy and side effects as important to their decision making: on a Likert scale from not at all important to very important, 74% reported that the risk of hip fracture as described in the vignettes was important or very important to their decision, and 63% that other fractures were important/very important. Side effects including osteonecrosis of the jaw (53%), stomach ailments (50%), and atrial fibrillation (62%) also were judged to be important/very important. Only 20 women (8%) reported previous knowledge of another side effect that affected their decision.
DISCUSSION
After receiving detailed information about fracture risk and pharmacologic prevention of fractures, only 51% of a sample of postmenopausal primary care patients would be willing to accept prescription osteoporosis medications at currently recommended risk thresholds. Women’s treatment acceptance rose with increasing fracture risk, from 43% at a 5% 10-year risk to 82% at a 50% 10-year risk. Women with perceptions that medications are generally not worth the risk were less likely to accept treatment. Although women with personal histories of osteoporosis or higher estimates of personal fracture risks were more likely to accept treatment for the low-risk scenarios, a substantial number of these women would also decline treatment.
One central finding of our study is that a substantial proportion, though not all, of a group of informed women would decline medications when fracture risk is low. Such decisions are consistent with current physician guidelines, which recommend treatment at or above a 10-year hip fracture risk of 3% or total fracture risk of 20%. This degree of fracture risk is extremely common in early menopause; the average postmenopausal woman in her 50s or 60s in the United States has 10-year fracture risks similar to those presented in scenarios 1 and 25,35. Treatment of these low-risk women is well above accepted cost-effectiveness thresholds36. However, bisphosphonates are FDA-approved for osteoporosis prevention for postmenopausal women generally, and 30–40% of a national sample of primary care physicians report that they recommend treatment of women with mild osteopenia37,38. Our results suggest that guidelines that advocate systematic use of a personalized fracture risk algorithm36,39, particularly if used with tools such as a patient decision aid40, have the potential to reduce such variation in treatment.
A related finding of our study is that a number of women might also be unwilling to accept treatment even when provided personalized information showing that they are at high risk. For such women, the benefits substantially outweigh the risks, and treatment may save money by reducing surgery costs41. Because our study did not provide physician guideline thresholds, we expected that subjects would not have an identical threshold to physician groups. Nonetheless, the substantial difference between subjects’ choices and guideline recommendations in our study adds to limited earlier evidence that well-informed subjects and physicians can be far apart in preventive thresholds. In breast cancer prevention, less than 1% of women who fit guideline-recommended risk thresholds took chemoprophylaxis after reviewing a comprehensive decision aid, and only 6% even talked to their doctors about tamoxifen12. Patient attitudes against use of cardiovascular preventive medications are not as extreme, but Canadian patients with hypertension had substantially higher treatment thresholds than their physicians13, and many US study subjects who were given detailed information about risks and benefits of cardiovascular medications reported that they would decline preventive medication even if they had substantial baseline cardiac risks42,43. This finding suggests the need for studies that examine ways to put risks into perspective for patients, such as providing estimates of the benefits of other major preventive interventions42.
The findings in our adjusted model also suggest that factors other than numerical risks and benefits might be used by patients considering osteoporosis therapy. In our study, personal experience with osteoporosis and personal risk perceptions were associated with decision-making thresholds for hypothetical patients. It is likely that personal experience with osteoporosis in relatives or friends influences actual patient decision making through familiarity with an issue or an “availability” heuristic42,44. In addition, respondents with higher levels of numeracy were less likely to accept treatment when the vignette indicated a low risk of fracture and more likely to accept treatment when the vignette indicated a high risk of fracture. This is consistent with prior findings that increased numeracy mitigates the effects of cognitive biases related to risk perception45.
Our study has some limitations. It was performed in a population with high osteoporosis screening rates, so it may not be generalizable to settings where there are fewer people who are aware of osteoporosis. However, this cohort was chosen because they were women likely to actually face osteoporosis decision making; other studies also suggest that exposure to osteoporosis information among postmenopausal women is relatively high46. We used vignettes rather than actual behavior, but the decision was nonetheless salient for nearly all of our participants, given that the majority would eventually become candidates for prescription fracture prevention5. There are limitations in the currently available data regarding the small but serious risks of bisphosphonates. For example, 1 metaanalysis of population-based studies suggested that the risk of bisphosphonate-associated osteonecrosis of the jaw among patients with osteoporosis is negligible, because its risk only becomes detectable with the higher cumulative doses used for metastatic cancer47, and many studies have not found any increase in atrial fibrillation48. Given our 10-year time horizon and the challenges of estimating rare medication risks, we chose to include the best available current estimates at the time of the study. Finally, to reduce any anchoring bias, we did not provide subjects with any guidance about others’ judgments of risk thresholds; it is possible that physician advice about thresholds would have changed our findings. However, our methods were designed to assess patient decision thresholds for preventive therapy independent of norms provided by physician guidelines to inform patient education.
About half of primary care subjects who were given information about osteoporosis and its treatment reported that they would be unwilling to accept treatment. This suggests that patients who are weighing risks and benefits of their own preventive care may believe less “care” (i.e., prescription medication use) is better in many situations. It may be particularly important to appropriately frame risks and benefits for patients at high fracture risk, because our study suggests that many such patients have higher expectations for preventive medicines than currently available medications can provide.
Footnotes
-
Dr. Neuner is supported by the US National Institutes of Health/National Institute on Aging (K08 AG021631) and the American Cancer Society (RSG-11-098-01-CPHPS). Dr. Schapira is supported by the American Cancer Society (RSG-11-104-01-CPPB).
- Accepted for publication November 27, 2013.








{kind=link}
{kind=link}