

Abstract
Objective. Ankylosing spondylitis (AS) is associated with excessive cardiovascular (CV) morbidity. Interactions between activated endothelium and monocytes precede atherosclerotic plaques. Our aim was to quantify blood monocyte subsets in relation to endothelial activation and inflammatory activity in subjects with AS who were free of clinical atherosclerotic CV disease.
Methods. Markers of inflammation and endothelial activation were measured in 47 patients with AS receiving no disease-modifying antirheumatic drugs, and 22 healthy controls. Exclusion criteria included atherosclerotic CV disease and traditional risk factors. Flow cytometry was used to identify monocyte subsets: classical CD14++CD16−, intermediate CD14++CD16+, and nonclassical CD14+CD16++ monocytes and to evaluate their expression of CD11b and CD11c.
Results. Traditional risk factors were comparable among the groups, except for lower high-density lipoprotein cholesterol in AS (p = 0.007). Relative to controls, in subjects with AS counts of classical monocytes were higher (84.3 ± 5.4 vs 78.9 ± 5.3% of blood monocytes, p < 0.001) and nonclassical monocytes lower (2.9 ± 2.2 vs 5.5 ± 2.3%, p < 0.001). In AS we observed increased soluble intercellular adhesion molecule-1 [251 (224–293) vs 202 (187–230) ng/ml, p = 0.002], an endothelial ligand for monocytic β2-integrin CD11b/CD18. CD11b expression on all 3 monocyte subsets was elevated in 21 AS subjects with a Bath Ankylosing Spondylitis Disease Activity Index score ≥ 4 versus the remaining patients (p = 0.005–0.03). C-reactive protein, interleukin 6 (IL-6), and pentraxin-3 were increased in AS, in contrast to tumor necrosis factor-α and IL-18. IL-6 correlated with classical monocytes numbers in AS (r = 0.56, p < 0.0001) but not in the controls (r = 0.10, p = 0.65).
Conclusion. Our findings suggest a contribution of immune dysregulation to enhanced monocyte-endothelial interactions in AS, especially in patients with active disease, which possibly can accelerate atherogenesis on a longterm basis.
Rheumatoid arthritis (RA), ankylosing spondylitis (AS), and psoriatic arthritis are associated with increased cardiovascular (CV) mortality and morbidity because of accelerated atherogenesis and disease-specific CV manifestations1,2,3. Features of endothelial dysfunction, a predecessor of atherosclerotic plaques, have been observed in patients with each of these inflammatory arthropathies and free of clinical atherosclerotic CV disease or classical risk factors4,5,6,7,8,9.
Interactions between activated endothelium and blood monocytes precede development of atherosclerotic plaques10. It has been recognized that not only endothelial dysfunction10,11,12 but also a shift in blood monocyte subsets can predict adverse CV outcome in various clinical settings13,14,15,16. Elevated counts of intermediate CD14++CD16+ monocytes (a minor monocyte subpopulation presumably representing a transitory stage of differentiation of predominant classical CD14++CD16− monocytes toward nonclassical CD14+CD16++ macrophage-like monocytes17) were associated with increased risk of ischemic CV events in endstage renal disease13 and nondialysis chronic kidney disease (CKD)14, and excessive risk of major CV events in patients referred for coronary angiography16. An increased frequency of CD14/CD16–double-positive monocytes or intermediate CD14++CD16+ monocytes was also reported in RA18,19,20 and psoriatic arthritis21. We have recently described elevated counts of intermediate monocytes in young adult survivors of childhood acute lymphoblastic leukemia22, also known to exhibit endothelial dysfunction23 and to be prone to late CV morbidity24.
To our knowledge, no study has focused on blood monocyte heterogeneity in AS to date. Thus, our aim was to estimate frequencies of circulating monocyte subsets and their relations with markers of endothelial dysfunction and inflammatory activity in patients naive to disease-modifying antirheumatic drugs (DMARD) and having AS free of clinical atherosclerotic CV disease.
MATERIALS AND METHODS
Subjects
We studied 47 patients aged 20–47 years (mean ± SD, 33 ± 6 yrs; 41 men and 6 women) with AS diagnosed according to the modified New York criteria25. All patients had predominantly axial disease and were HLA-B27–positive. The patients were receiving only nonsteroidal antiinflammatory drugs and none of them had been treated with nonbiologic DMARD, anti-tumor necrosis factor (anti-TNF) agents, or steroids. The mean disease duration was 8 ± 5 years. Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) scores26 averaged 4.1 ± 2.0 (range: 1.4–9.5). We also recruited a control group of 22 healthy volunteers aged 22–42 years (mean 30 ± 7 yrs; 12 men and 10 women).
Exclusion criteria were common for both groups and included clinical evidence of atherosclerotic CV disease, diabetes, hypertension, an estimated glomerular filtration rate (eGFR) below 90 ml/min per 1.73 m2 of body surface area, a history of malignancy, acute infections within previous 4 weeks, and any other chronic coexistent diseases. In agreement with the Declaration of Helsinki, the protocol had been approved by the ethics committee of our university, and written informed consent was obtained from each subject before inclusion in the study.
Study protocol
The procedure was carried out in the morning in the out-patient clinic of our center. The subjects had been asked to refrain from eating, smoking, and alcohol or caffeine consumption for at least 12 h prior to the study. The personnel involved in the protocol recorded demographic and clinical characteristics, anthropometric measurements were taken, and blood pressure was measured on the left arm after 5 min of rest in a sitting position. Then all participants underwent blood sampling for biochemical assays and flow cytometry.
Biochemical assays
A sample of blood was drawn from a left antecubital vein for measurements of serum concentrations of high-sensitivity C-reactive protein (hs-CRP) by immunonephelometry (Dade Behring II Nephelometer, GMI Inc.). Glucose, lipids, and creatinine were measured with a Hitachi 917 analyzer (Roche Diagnostics) using standardized laboratory techniques. An eGFR was calculated by the Chronic Kidney Disease Epidemiology Collaboration formula, which has proven more accurate than the Modification of Diet in Renal Disease study equation, especially at normal renal function27.
Plasma for extended biochemical analyses was collected from EDTA-anticoagulated blood and frozen at −80°C until assayed. Commercially available ELISA were used to measure plasma levels of TNF-α and interleukin 6 (IL)-6 (Quantikine high-sensitivity kits), monocyte chemotactic protein-1 (MCP-1), pentraxin-3 (PTX-3), soluble forms of vascular cell adhesion molecule-1 (sVCAM-1) and intercellular adhesion molecule-1 (sICAM-1; all R&D Systems), and IL-18 (MBL).
Flow cytometry
As described22, peripheral blood mononuclear cells were isolated from EDTA-anticoagulated blood and collected on the same day as remaining samples, using density gradient centrifugation and LSM 1077 (Lymphocyte Separation Medium, PAA Laboratories GmbH). One hundred thousand cells were stained for 20 min with fluorochrome-conjugated monoclonal antibodies (anti-CD14-APC-H7, anti-CD16-PE, anti-HLA-DR-PE-Cy7, anti-CD11b-Pacific Blue; and anti-CD11c-APC; Becton Dickinson Biosciences — Pharmingen) and then washed with phosphate buffered saline containing 1% fetal bovine serum (GIBCO). The cells were processed in the FACSCanto II flow cytometer (BD Biosciences) and then analyzed with FACSDiva software (BD Biosciences) and FlowJo (TreeStar Inc.). The cells were gated in a side scatter/forward scatter plot with the scatter gate for monocytes partially extending into lymphocytes28. The cells containing all monocytes and a part of the lymphocyte population were then gated in an HLA-DR/CD14 plot to exclude HLA-DR–negative natural killer cells (which would otherwise contaminate the CD14+CD16++ subpopulation) and finally analyzed for CD14 and CD16 expression28,29. Monocyte subsets were defined according to the expression of CD16 (Fcγ receptor type III) and CD14 (lipopolysaccharide receptor) as classical monocytes (CD14++CD16−), intermediate monocytes (CD14++CD16+), and nonclassical monocytes (CD14+CD16++)17. The expression of CD11b and CD11c on the 3 monocyte subsets was quantified. The results have been presented as either the percentage of cells expressing individual markers, absolute cell counts (per μl of blood), or mean fluorescence intensity (MFI). Total numbers of monocytes were calculated using peripheral white blood cell counts. In separate experiments BD Trucount beads were used, confirming that both methods yielded similar absolute values of cell counts.
All experiments were performed under standardized experimental conditions, including the procedure of cell isolation and reagents for sample preparation. The same number of cells and the same amounts of antibodies were used for samples. Simultaneously, in each case we checked the proper operation of the flow cytometer using BD Cytometer Setup and Tracking beads. Also, the operational stability was verified, so that the individual measurements did not differ significantly one from the other. Flow cytometry compensation was verified regularly using cells studied in the experiment and CompBeads. One operator performed the sample collection and the data analysis.
Statistical analysis
Data are presented as mean ± SD unless stated otherwise or medians (interquartile range) for continuous variables, and numbers (percentages) for categorical variables. The accordance with a normal distribution was tested by the Kolmogorov-Smirnov test, and uniformity of variance (homoscedasticity) by Levene’s test. Intergroup differences were assessed by the unpaired 2-sided Student’s t test for continuous variables and Fisher’s exact test for proportions. Logarithmic transformation (ln, natural logarithm) was applied, when necessary, to obtain a normal distribution (hs-CRP, TNF-α, IL-6, sVCAM-1, PTX-3, percentage of intermediate monocytes) or to eliminate the nonuniformity of variances. The 2-sided Welch’s t test was used in case of the lack of homogeneity of variances even in ln-transformed data. A p-value below 0.05 was considered significant. Bivariate relations between continuous variables were estimated by Pearson’s correlation coefficients (r). Owing to multiple testing, exclusive correlations with p ≤ 0.001 were inferred as significant. Analyses were performed by means of the Statistica data analysis software system (version 10.0.1011.0; StatSoft Inc.).
RESULTS
Clinical and biochemical characteristics of the patients with AS and healthy controls
Traditional CV risk factors were similar in patients with AS and healthy controls except for lower high-density lipoprotein (HDL) cholesterol, in agreement with a previous report30, and a higher ratio of total cholesterol to HDL cholesterol in AS (Table 1). Additionally, levels of fibrinogen, hs-CRP, IL-6, sICAM-1, and PTX-3 were significantly increased in patients with AS, whereas TNF-α, sVCAM-1, IL-18, and MCP-1 were similar between the groups (Table 2).
Clinical and conventional biochemical characteristics of patients with ankylosing spondylitis (AS) and control subjects. Data are shown as medians (interquartile range) or n (%). P values in boldface are statistically significant.
Extended inflammatory markers in ankylosing spondylitis (AS) patients and controls. Data are shown as medians (interquartile range). P values in boldface are statistically significant.
Blood monocyte subsets and their expression of CD11b and CD11c in patients with AS and healthy controls
Compared to the controls, patients with AS exhibited significantly higher counts of classical CD14++CD16− monocytes and lower numbers of nonclassical CD14+CD16++ monocytes (Table 3). There were no differences in the expression of CD11b and CD11c on all 3 monocyte subsets between AS subjects and the controls (p > 0.1).
Monocyte subsets and total monocyte counts in ankylosing spondylitis (AS) patients and healthy subjects. Data are shown as mean ± SD. P values in boldface are statistically significant.
Pooling both groups as a whole, men tended to have higher total monocyte counts than women (536 ± 208 vs 436 ± 115 cells/μl, p = 0.09). Because the percentage of men was higher in patients with AS (87% vs 55%), we repeated the comparisons after limitation of the analysis to male subjects, which revealed similar directions and levels of significance for intergroup differences in classical (p = 0.001) and nonclassical (p < 0.001) monocytes.
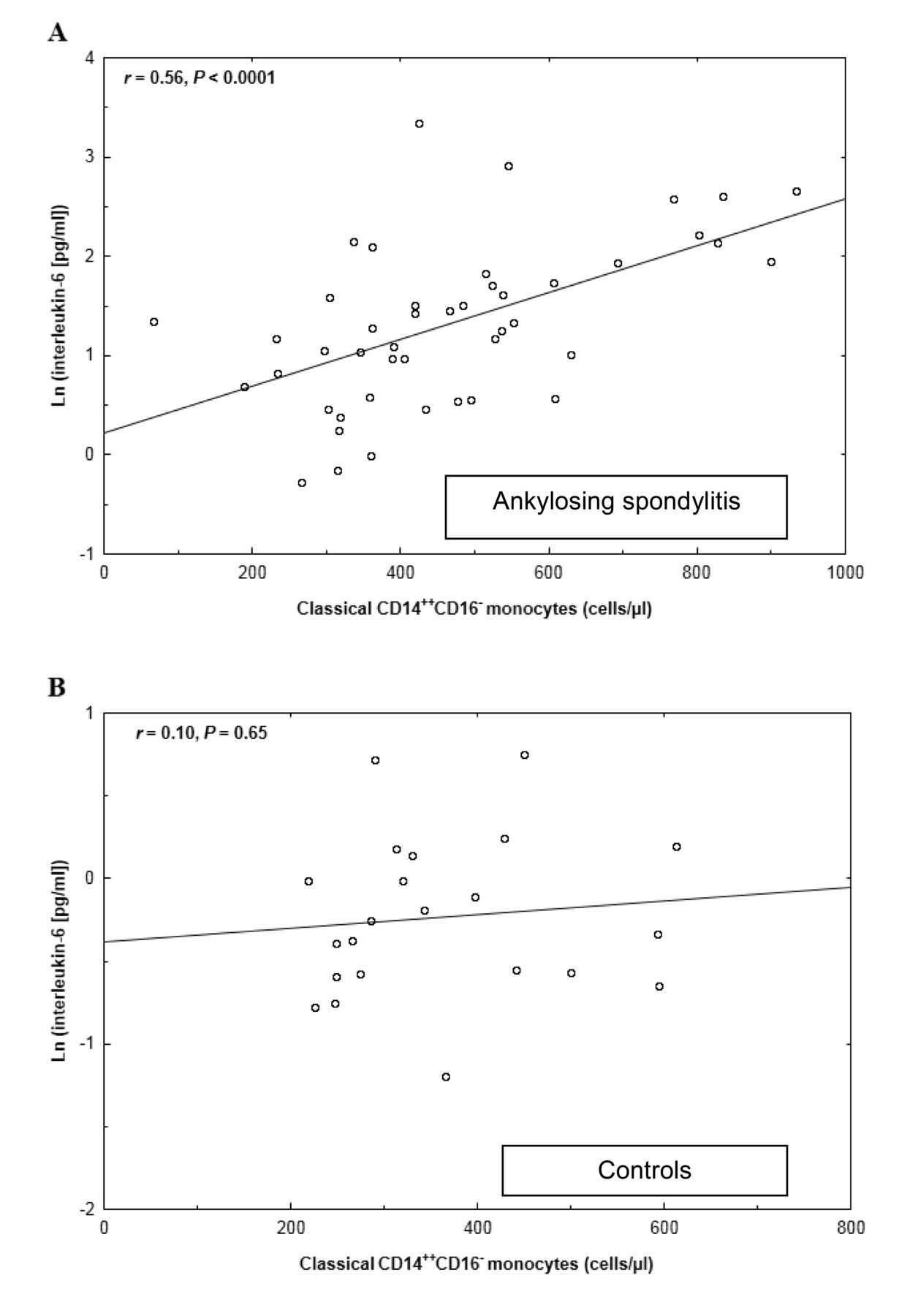
There was a correlation between IL-6 and the count of classical monocytes in patients with AS (r = 0.56, p < 0.0001; (Table 4 and Figure 1A) but not in the controls (r = 0.10, p = 0.65; Figure 1B). Neither HDL cholesterol nor the ratio of total to HDL cholesterol correlated to any of the variables derived from flow cytometry (p ≥ 0.1).

A positive correlation between the numbers of classical monocytes and interleukin 6 levels in patients with ankylosing spondylitis (A) but not in the controls (B). Levels of interleukin 6 were transformed in natural logarithm (Ln) to obtain a normal distribution.
Pearson’s correlation coefficients between inflammatory markers, disease activity, monocyte subsets size, and monocytic CD11b and CD11c expression in patients with ankylosing spondylitis. Data in boldface are statistically significant.
Clinical and biochemical characteristics, monocyte subset size, and monocytic expression of CD11b and CD11c in relation to disease activity
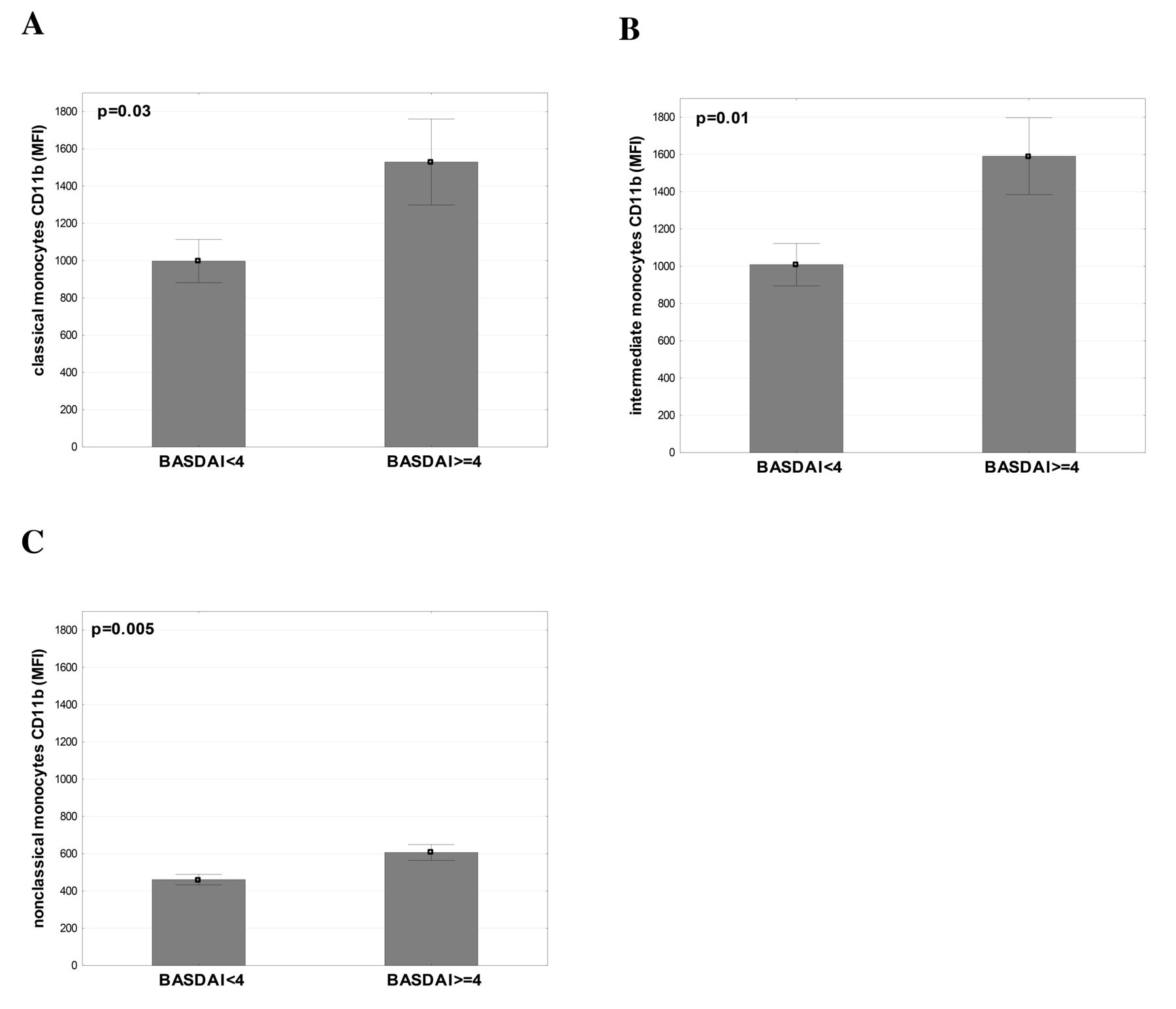
BASDAI correlated to the expression of CD11b on classical (r = 0.47, p = 0.001), intermediate (r = 0.49, p < 0.001), and nonclassical monocytes (r = 0.52, p < 0.001; Table 4). Accordingly, compared to AS patients with a BASDAI score < 4 (n = 26), AS patients with BASDAI ≥ 4 (n = 21) had higher monocytic expression of CD11b on classical (1529 ± 1006 vs 998 ± 591 MFI, p = 0.03; Figure 2A), intermediate (1591 ± 899 vs 1009 ± 579 MFI, p = 0.01; Figure 2B), and nonclassical monocytes (607 ± 185 vs 461 ± 143 MFI, p = 0.005; Figure 2C). Relative increases in CD11b expression on classical, intermediate, and nonclassical monocytes associated with a high disease activity averaged 53%, 58%, and 32%, respectively, with the reference to the remaining subjects with AS. The expression of CD11b was reduced by about one-third in the patients with AS who had a low disease activity, relative to controls on all 3 monocyte subpopulations: classical (998 ± 591 vs 1539 ± 629 MFI, p = 0.003), intermediate (1009 ± 579 vs 1523 ± 584 MFI, p = 0.004), and nonclassical monocytes (461 ± 143 vs 729 ± 566 MFI, p = 0.02).
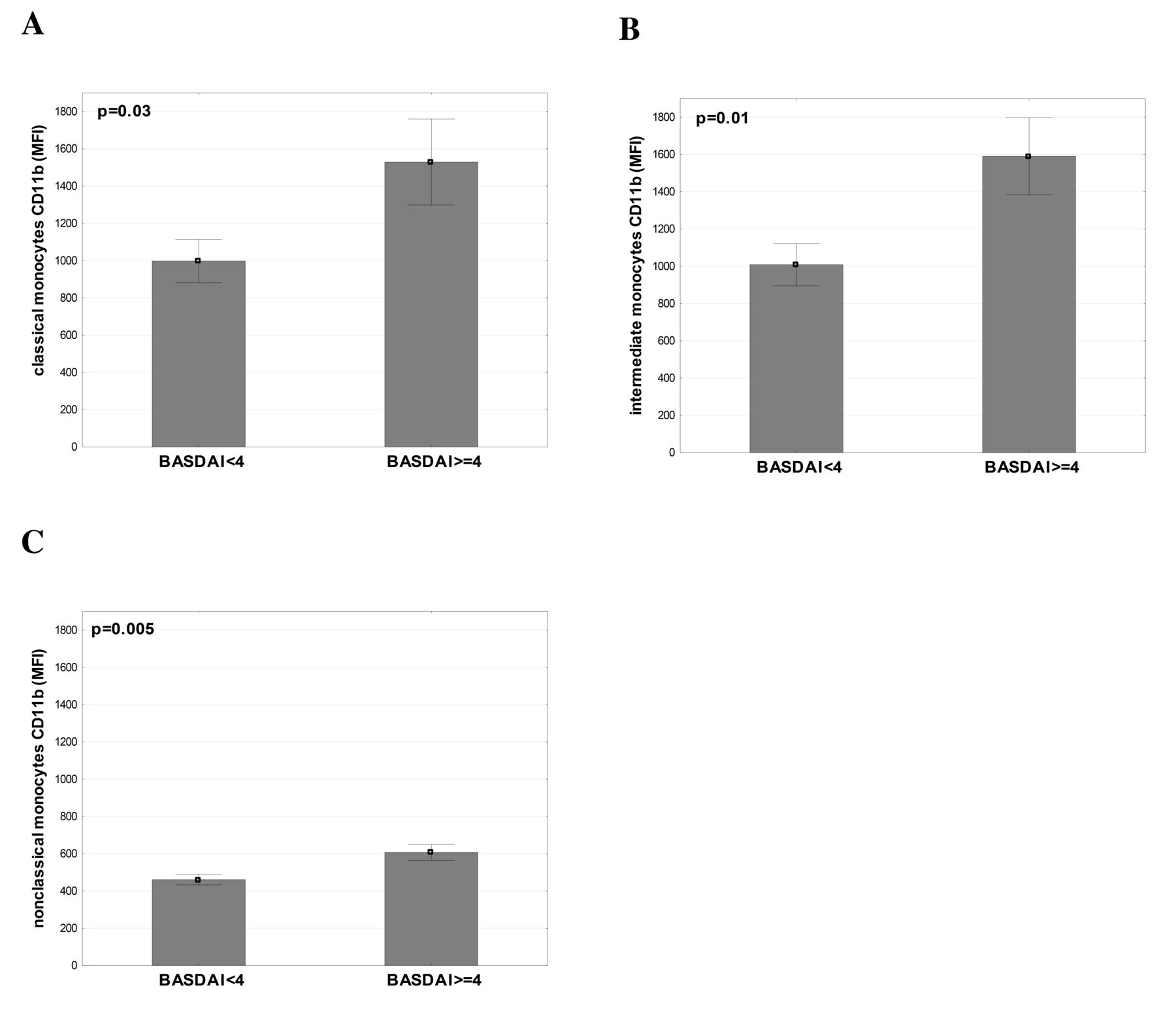
Elevated CD11b expression on classical (A), intermediate (B), and nonclassical (C) monocytes in subjects with ankylosing spondylitis and a BASDAI score ≥ 4 (n = 21) compared to the remaining patients (n = 26). Data are shown as means ± SE of the mean; p values by Student’s t test. BASDAI: Bath Ankylosing Spondylitis Disease Activity Index score; MFI: mean fluorescence intensity.
The AS patients with a BASDAI score ≥ 4 and < 4 did not differ in terms of traditional risk factors (p > 0.1), levels of sICAM-1 (270 ± 70 vs 262 ± 50 ng/ml, p = 0.7, respectively), sVCAM-1 [541 (491–607) vs 591 (500–658) ng/ml, p = 0.08], hs-CRP [7.02 (2.57–18.20) vs 5.05 (2.95–13.60) mg/l, p = 0.8], PTX-3 [631 (421–739) vs 551 (483–772) pg/ml, p = 0.6], TNF-α [1.77 (1.50–2.20) vs 1.80 (1.58–2.07) pg/ml, p = 0.8], IL-6 [3.09 (2.24–6.98) vs 3.55 (1.80–5.55) pg/ml, p = 0.5], IL-18 [446 ± 137 vs 422 ± 153 pg/ml, p = 0.6], MCP-1 [252 ± 72 vs 264 ± 74 pg/ml, p = 0.6], and size of monocyte subsets (p = 0.4–0.8; Table 4).
The expression of CD11c was similar in patients with AS who had high disease activity, low disease activity, and the controls on classical (1475 ± 638 vs 1522 ± 497 vs 1695 ± 1231 MFI, respectively), intermediate (3381 ± 1025 vs 3468 ± 1040 vs 3983 ± 2612 MFI), and nonclassical monocytes (3620 ± 972 vs 3809 ± 1029 vs 3635 ± 2359 MFI; all intergroup p = 0.3–0.9).
DISCUSSION
Our salient finding was a higher number of classical CD14++CD16− blood monocytes and its association with elevated IL-6 levels in DMARD-naive patients with AS. This study is the first, to our knowledge, to report a shift in blood monocyte subpopulations in AS. Additionally, in AS we observed increased sICAM-1, a marker of endothelial activation and an endothelial ligand for monocytic β2-integrin CD11b/CD18. Moreover, on all 3 monocyte subsets the expression of CD11b was decreased in AS subjects with low disease activity compared to those with high disease activity, or healthy controls.
The shift in monocyte subsets in AS differed from the previously observed expansion of CD14/CD16–double positive monocytes18,20 or CD14++CD16+ intermediate monocytes19 in RA. This might result from distinct pathogenesis of these 2 forms of inflammatory arthritis. However, we have not studied patients with RA, which limits comparisons of our findings with those reports18,19,20.
That the observed increase in CD14++CD16− monocyte counts in AS correlated to 6-fold elevated IL-6 levels, but not TNF-α or IL-18 concentrations, is compatible with a high secretion of IL-6 by classical monocytes from healthy individuals in response to lipopolysaccharide31,32. Because IL-6 (besides inducing the synthesis of acute-phase reactants) plays a role in the differentiation of Th1733 and Th2 cells34, this relationship may reflect the contribution of a shift in blood monocyte subpopulations to the pathogenesis of AS, reportedly associated with a 10-fold increase in the percentage of Th17 cells among peripheral blood mononuclear cells without in vitro stimulation35. Nevertheless, it is unknown whether classical monocytes have the same properties in patients with AS and healthy subjects.
Previous reports relating monocyte heterogeneity to CV prognosis are inconsistent. A higher frequency of intermediate monocytes but not classical monocytes independently predicted adverse CV outcome in 94 patients receiving dialysis and in 119 nondialysis CKD subjects followed for about 3 and 5 years, respectively13,14. In 951 patients referred for elective coronary angiography, mainly with prevalent coronary artery disease (CAD) or cerebrovascular disease, both classical and intermediate monocytes emerged as univariate predictors of major CV events during a mean followup of 2.6 years, whereas upon multivariate adjustment the statistical significance was retained exclusively for intermediate monocytes16. Therefore, our findings might suggest that excessive CV risk in AS might be independent of a shift in favor of classical monocytes.
On the other hand, classical monocytes, but not other monocyte subsets, independently predicted ischemic CV events in 700 randomly selected participants of the cardiovascular arm of the Malmö Diet and Cancer study over a 15-year followup15. Additionally, in a group of high-risk patients with stable CAD36, the proportion of classical monocytes was elevated at the expense of nonclassical monocytes, as in our AS subjects, compared to low-risk and medium-risk groups delineated on the basis of the number of traditional risk factors in 80 subjects with CAD. Further, Urra, et al37 found a positive association between classical monocytes (which exhibited the highest platelet-monocyte interactions) and 3-month mortality in 46 consecutive patients with stroke.
However, the published observations on the association between adverse CV outcome and classical CD14++CD16− monocytes or intermediate CD14++CD16+ monocytes may be not entirely contradictory because Cros, et al31 have provided evidence (by means of whole-genome expression arrays) that both classical and intermediate human monocytes resemble murine Ly6ChighGr+ monocytes, exhibiting preferential homing to activated endothelium and atherosclerotic plaques in experimental models of atherosclerosis38,39,40. In addition, preferential transendothelial migration in response to MCP-1 was demonstrated for human classical monocytes as compared to the other monocyte subsets41. Moreover, classical monocytes are the main source of reactive oxygen species31,42 known to impair the activity of nitric oxide43, an endogenous antiatherogenic molecule.
Thus, an increased frequency of classical monocytes in our subjects with AS who had elevated sICAM-1, an index of endothelial activation and an endothelial ligand for monocytic β2-integrin CD11b/CD1844, supported by a relative increase in the expression of CD11b on classical and intermediate monocytes by over 50% in patients with active disease compared to those with low disease activity, might reflect enhanced leukocyte-endothelial interactions and chronic inflammation within the vascular wall10. Because BASDAI score had been reportedly associated with traditional risk factors, including metabolic syndrome components45,46, the leukocyte-endothelial interactions could potentiate pro-atherogenic effects of the classical risk factors in patients with high disease activity. Admittedly, monocytic CD11b expression did not differ between the patients with AS who had active disease and the controls; nevertheless, a decreased CD11b expression on monocytes of the subjects with AS who had low disease activity could hypothetically reflect an effective compensatory antiinflammatory mechanism that was absent in those with a BASDAI score ≥ 4. This suggestion remains speculative and requires further investigation.
On the other hand, the biological significance of relatively small differences in sICAM-1 levels and the frequency of classical monocytes remains unclear. Nevertheless, compared to controls, patients with AS exhibited higher average relative elevations of these variables [classical monocytes: 469 vs 364 per μl of blood (29%); sICAM-1: 251 vs 202 ng/ml (25%)] than those previously reported in participants who later experienced an ischemic CV event versus the event-free subjects in prospective studies [classical monocytes: 344 vs 297 per μl of blood (16%) in the Malmö Diet and Cancer study15; sICAM-1: 289 vs 244 ng/ml (18%) in the Atherosclerosis Risk in Communities study47].
It is noteworthy that PTX-3, elevated in patients with AS, is released locally from cells involved in atherogenesis and (despite its atheroprotective effects) can be considered a marker of vascular inflammation48. Further, higher PTX-3 levels predicted CV mortality independently of hs-CRP and traditional risk factors in subjects free of prevalent CV disease49. However, we have provided no direct evidence supporting the notion of a better ability of PTX-3, adhesion molecules, or monocyte subsets to predict accelerated atherogenesis compared to classical risk factors and conventional inflammatory markers in AS. To verify this speculative concept, further studies are warranted, relating these variables to coexistent atherosclerotic CV disease or subclinical atherosclerosis in patients with AS.
Several limitations of our study need to be acknowledged. First, the small number of subjects constrains the conclusions based on our findings. Second, we have measured cytokines and chemokines in plasma, whereas the assessment of cytokine generation in response to various stimuli and the expression of chemokine receptors by different monocyte subsets would add information to the in situ plasma levels18,19,31,32,42. Third, we are not able to exclude the influence of nonsteroidal antiinflammatory drugs on the activation of both monocytes and endothelial cells in patients with AS. Fourth, blood monocyte subpopulations might be affected by lipids50, and a lower level of HDL cholesterol was observed in subjects with AS. However, no lipid variable correlated to the size of any of the monocyte subsets or their β2-integrin expression in our study. Finally, although we made every effort to ensure similar characteristics in both groups, the percentage of men was higher in AS. Rogacev, et al16 described higher absolute counts of classical monocytes in men referred for elective coronary angiography mainly because of increased numbers of total monocytes, also present in our data. Nevertheless, we observed intergroup differences in both relative and absolute counts of classical monocytes, which argues against the notion of sex differences in total monocyte counts as an explanation of our results. In addition, the results have not changed after limitation of the analysis to male subjects.
Patients with AS exhibit a shift in blood monocyte subpopulations. Our preliminary cross-sectional findings suggest contribution of immune dysregulation to enhanced monocyte-endothelial interactions in AS, especially in patients with active disease, which possibly can accelerate atherogenesis on a longterm basis. Further longitudinal studies are warranted to determine the relevance of these abnormalities for late CV morbidity.
Footnotes
-
Dr. Surdacki and Dr. Sulicka contributed equally to this work and are co-first authors.
-
Supported in part by a research grant from the Ministry of Science and Higher Education, Warsaw, Poland (No. N402 267636).
- Accepted for publication November 27, 2013.








{kind=link}
{kind=link}