

Abstract
Objective. To assess the occurrence, risk factors, morbidity, and mortality associated with lower extremity (LE) ulcers in patients with rheumatoid arthritis (RA).
Methods. Retrospective review of Olmsted County, Minnesota, USA, residents who first fulfilled the 1987 American College of Rheumatology criteria for RA in 1980–2007 with followup to death, migration, or April 2012. Only LE ulcers that developed after the diagnosis of RA were included.
Results. The study included 813 patients with 9771 total person-years of followup. Of them, 125 developed LE ulcers (total of 171 episodes), corresponding to a rate of occurrence of 1.8 episodes per 100 person-years (95% CI: 1.5, 2.0 per 100 person-yrs). The cumulative incidence of first LE ulcers was 4.8% at 5 years after diagnosis of RA and increased to 26.2% by 25 years. Median time for the LE ulcer to heal was 30 days. Ten of 171 episodes (6%) led to amputation. LE ulcers in RA were associated with increased mortality (HR 2.42; 95% CI 1.71, 3.42), adjusted for age, sex, and calendar year. Risk factors for LE ulcers included age (HR 1.73 per 10-yr increase; 95% CI 1.47, 2.04), rheumatoid factor positivity (HR 1.63; 95% CI 1.05, 2.53), presence of rheumatoid nodules (HR 2.14; 95% CI 1.39, 3.31), and venous thromboembolism (HR 2.16; 95% CI 1.07, 4.36).
Conclusion. LE ulcers are common among patients with RA. The cumulative incidence increased by 1% per year. A significant number require amputation. Patients with RA who have LE ulcers are at a 2-fold risk for premature mortality.
Rheumatoid arthritis (RA) is a common systemic inflammatory disorder that primarily affects the joints1. Lower extremity (LE) ulcer is one of the known common complications of longstanding RA. Based upon self-report, the prevalence of foot ulceration in RA has been estimated at 3.13%2. An overall prevalence of 10.08% was reported in a study from the UK, as opposed to a prevalence of chronic leg ulcers in 1% of the general adult population2,3. In contrast to diabetic foot ulcers, little is known regarding the magnitude and morbidity associated with LE ulcers in RA. We aimed to assess the occurrence, risk factors, morbidity, and mortality associated with lower extremity ulcers in RA.
MATERIALS AND METHODS
Study setting
This is a retrospective population-based study performed using resources of the Rochester Epidemiology Project (REP) medical record linkage system4. The REP allows virtually complete access to medical records from all community medical providers including the Mayo Clinic, Olmsted Medical Center and its affiliated hospitals, local nursing homes, and the few private practitioners in Olmsted County, Minnesota, USA. The uniqueness of the REP and its advantages in performing population-based studies in rheumatic diseases has been described5,6.
Study subjects and data collection
Cases of RA incident between January 1, 1980, and December 31, 2007, among residents of Olmsted County were previously identified using the REP. RA was defined according to the 1987 American College of Rheumatology criteria, as described7,8. All medical records of patients with RA were retrospectively reviewed and longitudinally followed until death, migration, or April 2012. Medical records were reviewed for episodes of LE ulcers. For the purpose of the study, LE ulcer was defined as a full-thickness skin defect occurring in isolation on or below the mid-level of thighs supported by physician diagnosis, clinical history, and physical examination. Excluded were LE ulcers due to surgery, biopsy, burns, animal bites, ingrown toenail, toenail removal, abrasion, cellulitis, foreign body, or herpes zoster. Further categorization of the LE ulcer according to ischemic, pressure, venous, vasculitic, and diabetic neuropathy was done based on physician diagnosis supported by available information such as ankle-brachial index, peripheral arterial angiogram, duplex ultrasound, location of the ulcer, history of trauma, biopsy results or impression of rheumatologist, podiatrist, or specialist in wound care or vascular medicine. Smoking status at the onset of LE ulcer was obtained. The use of antirheumatic medications at the onset of the LE ulcer was recorded, including disease-modifying antirheumatic drugs [DMARD; i.e., methotrexate (MTX), hydroxychloroquine, and other DMARD, and biologic response modifiers], systemic glucocorticosteroids, and nonsteroidal antiinflammatory drugs (NSAID, including cyclooxygenase-2 inhibitors).
Information regarding ulcer treatment including conservative, medical, or surgical measures was obtained. Information regarding RA disease in this cohort of patients was already collected for previous epidemiological studies8,9. This included results of clinically performed tests for rheumatoid factor (RF) and erythrocyte sedimentation rate (ESR), persistently high ESR (≥ 3 ESR values ≥ 60 mm/h with ≥ 30 days between measurements), large joint swelling, joint erosions/destructive changes on radiographs, joint surgery (i.e., synovectomy and arthroplasty), and severe extraarticular manifestations of RA (defined according to the Malmö criteria)10.
Statistical methods
Descriptive statistics (means, percentages, etc.) were used to summarize characteristics of the patients. Person-year methods were used to estimate the rate of occurrence of LE ulcers. Ninety-five percent CI for the rates was calculated assuming the observed LE ulcers followed a Poisson distribution. Cumulative incidence of LE ulcers adjusted for the competing risk of death was estimated11. These methods are similar to the Kaplan-Meier method, with censoring of patients who are still alive at last followup. However, patients who die before experiencing LE ulcers are appropriately accounted for to avoid overestimation of the rate of occurrence of LE ulcers, which can happen if such subjects are simply censored.
Cox proportional hazards models were used to assess the association of risk factors with LE ulcers. These models were adjusted for age, sex, and calendar year of RA incidence. Time-dependent covariates were used to model risk factors that developed over time (e.g., joint surgery, rheumatoid nodules, severe extraarticular manifestations, medication exposures), allowing patients to be modeled as “unexposed” to the risk factor during the followup time prior to development of the risk factor, then change to “exposed” following development of the risk factor. Because risk factor data were collected previously, they were available only through December 31, 2008, for patients who were still alive and living in Olmsted County on that date. Therefore, followup was truncated at the last followup of available risk factor data for the risk factor analyses, and LE ulcers occurring after that data were not included in these analyses.
The influence of LE ulcers on mortality was examined using Cox models with time-dependent covariates for the first LE ulcer occurring during followup. First, the influence of LE ulcers on mortality was assessed in a model adjusted for age, sex, and calendar year of RA incidence. Then the influence of LE ulcers was assessed in a model that was additionally adjusted for factors known to be related to mortality: body mass index (BMI), history of smoking, RF positivity, severe extraarticular manifestations, comorbidities [diabetes mellitus (DM), cardiovascular (CV) disease, cerebrovascular disease, venous thromboembolism, renal disease, liver disease, dementia, and cancer], history of alcohol abuse, exposure to glucocorticosteroids, and DMARD and/or biologic agents. This additional list of adjustors was obtained from a previous study12 and augmented with factors found to be associated with the occurrence of LE ulcers, in an attempt to provide a comprehensive adjustment while avoiding issues of bias related to variable selection. Poisson regression models were used to examine trends in LE ulcers over time. Both calendar time and disease duration were examined. In these models, smoothing splines were used to allow examination of potential nonlinear time trends, and the models were adjusted for age and sex.
RESULTS
The study included 813 patients with incident RA between January 1, 1980, and December 31, 2007. The characteristics of the 813 patients with RA are listed in Table 1. All patients were 18 years or older. There were 556 women (68%) and 257 men (32%). The mean age at diagnosis of RA was 56 years. The average length of followup was 12 years, with 9771 total person-years of followup for the cohort. RF was positive in 537 patients (66%). The mean ESR at diagnosis of RA was 24.8 mm/h.
Characteristics of 813 patients with rheumatoid arthritis (RA).
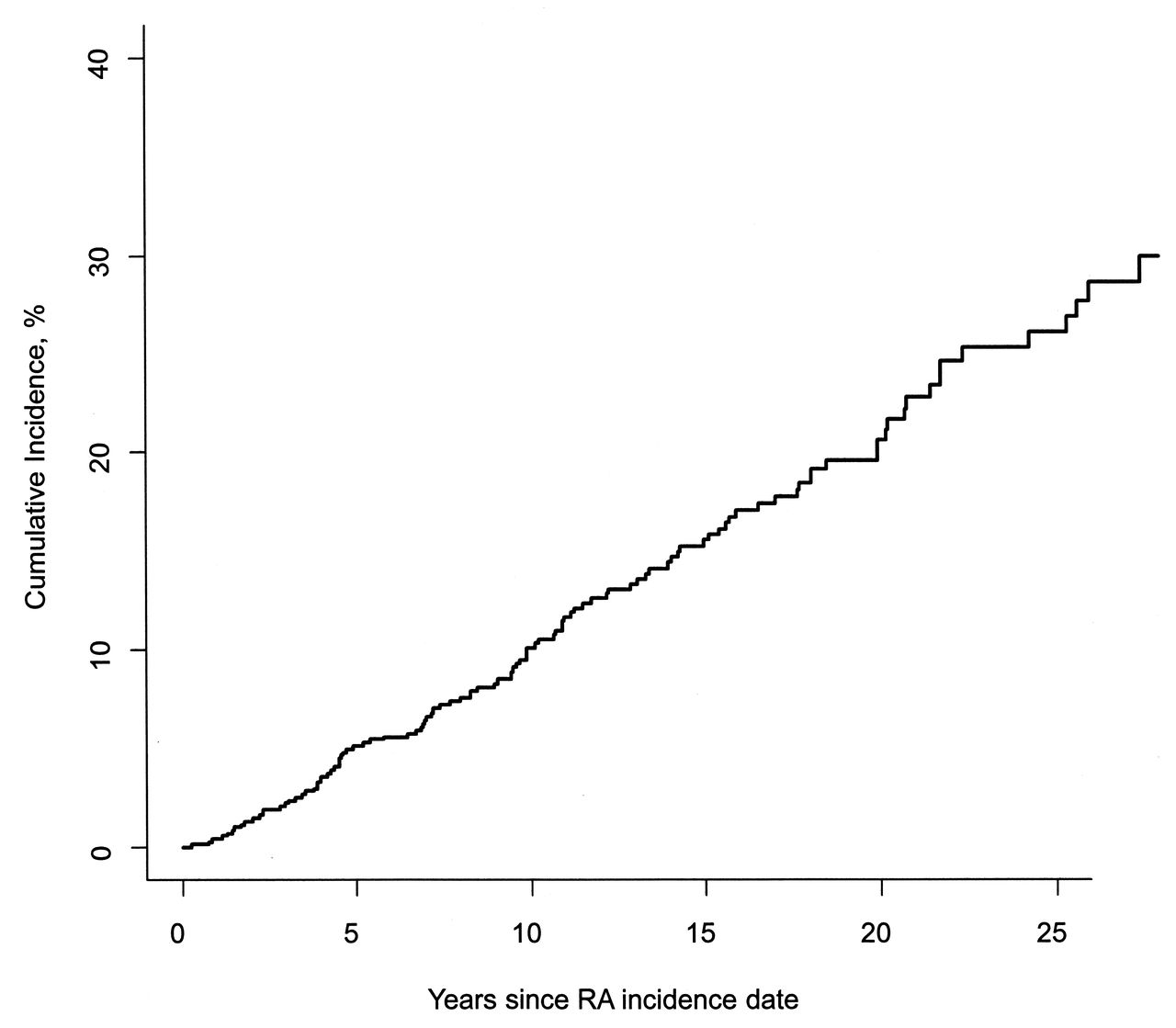
LE ulcer occurred in 125 patients with a total of 171 episodes, which corresponds to a rate of occurrence of 1.8 episodes per 100 person-years (95% CI 1.5, 2.0 per 100 person-yrs). The rate of occurrence of a first LE ulcer was 1.4 per 100 person-years (95% CI 1.1, 1.6 per 100 person-yrs). Among patients with a first LE ulcer, the rate of occurrence of a second LE ulcer was substantially increased (7.9 per 100 person-yrs; 95% CI 5.5, 10.9). The cumulative incidence of first LE ulcers in patients with RA was 4.8% (95% CI 3.2%, 6.4%) at 5 years after diagnosis of RA and increased to 26.2% (95% CI 21.3%, 31.1%) by 25 years (Figure 1). The constant rate of increase of 1% per year in the cumulative incidence of first LE ulcers suggests that there was no association between RA disease duration and the occurrence of LE ulcers. There was no apparent change in the rate of development of LE ulcers over the range of RA disease duration (p = 0.71). Analyses of disease duration trends in rate of LE ulcers by type revealed a significant decline in the rates of venous LE ulcers (p = 0.007), which appeared to be most common in the first few years after RA incidence. A marginal increase in the rate of pressure LE ulcers over disease duration (p = 0.12) was also noted.
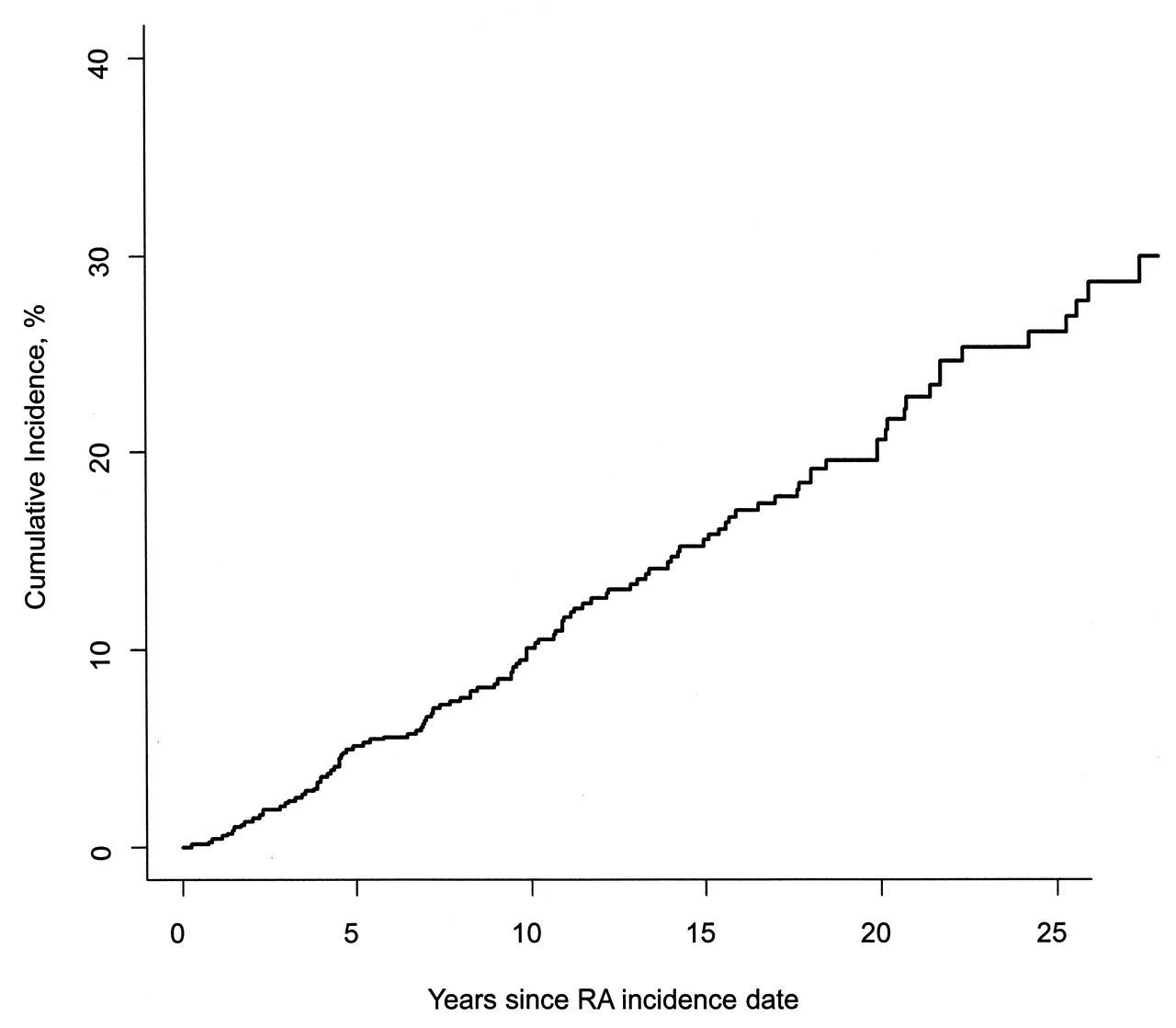
Cumulative incidence of foot ulcers among 813 patients with rheumatoid arthritis (RA).
The LE ulcers were located between ankle and knee in 58 episodes (34%), tip of toes in 46 episodes (27%), plantar metatarsal in 18 episodes (11%), heel in 18 episodes (11%), lateral malleolus in 18 episodes (11%), and medial malleolus in 13 episodes (8%).
Comorbidities included varicose veins in 32 episodes (19%), DM in 42 (25%), coronary artery disease in 54 (32%), and peripheral arterial disease in 33 (19%). Pressure ulcers were noted in 62 episodes (36%), ischemic ulcers in 22 (18%), venous ulcers in 20 (12%), neuropathic ulcers in 18 (11%), and vasculitic ulcers in 2 (1%). Etiology was unclear or unknown in 10 episodes (6%). A history of smoking was noted in 15 episodes (9%) at diagnosis of LE ulcer (Table 2). A history of recent local trauma was noted in 69 episodes (40%).
Characteristics of 171 lower extremity ulcer episodes in 125 patients with rheumatoid arthritis.
Vascular imaging was performed in 49 episodes (29%). Biopsy of the ulcer was done in 9 episodes (5%). Some of the episodes fell under more than 1 category of type of ulcer. Antirheumatic medications used at the onset of LE ulcer included NSAID in 70 episodes (41%), glucocorticosteroids in 79 (46%), MTX in 63 (37%), leflunomide in 9 (5%), infliximab in 4 (2%), etanercept in 5 (3%), rituximab in 3 (2%), and cyclophosphamide in 2 (1%). At the onset of LE ulcer, infliximab was stopped in 1 episode and etanercept in 2 episodes.
LE ulcer treatment included conservative methods such as elevation of foot, cleaning, moist sterile dressing, and/or compression bandages in almost all cases (169 episodes). The LE ulcers healed spontaneously with conservative therapy in 18 episodes (11%). Antibiotic was used in 147 episodes (86%). Topical glucocorticosteroid therapy was used in 4 episodes (2%). Surgical skin grafting was done in 5 episodes (3%) and surgical debridement in 44 (26%). Surgical limb amputation was required in 10 episodes (6%). The mean time for the ulcers to heal was 120 days [SD 290; median time 30 days (25th percentile 14, 75th percentile 115)].
The incidence of LE ulcers in RA increased among patients with incident RA in the 1995–2007 period compared to those with incident RA in the 1980–1994 period (HR 2.14; 95% CI 1.27, 3.58; Table 3). The incidence of LE ulcers increased 6% per year over the range of calendar years of followup (rate ratio: 1.06 per year, 95% CI 1.03, 1.10, p < 0.001; Figure 2). Analyses of time trends by type of LE ulcer revealed significant increases in the rates of venous (p = 0.027), pressure (p = 0.002), and traumatic (p = 0.003) LE ulcers, but no trends over time in ischemic (p = 0.30) or diabetic (p = 0.53) LE ulcers.
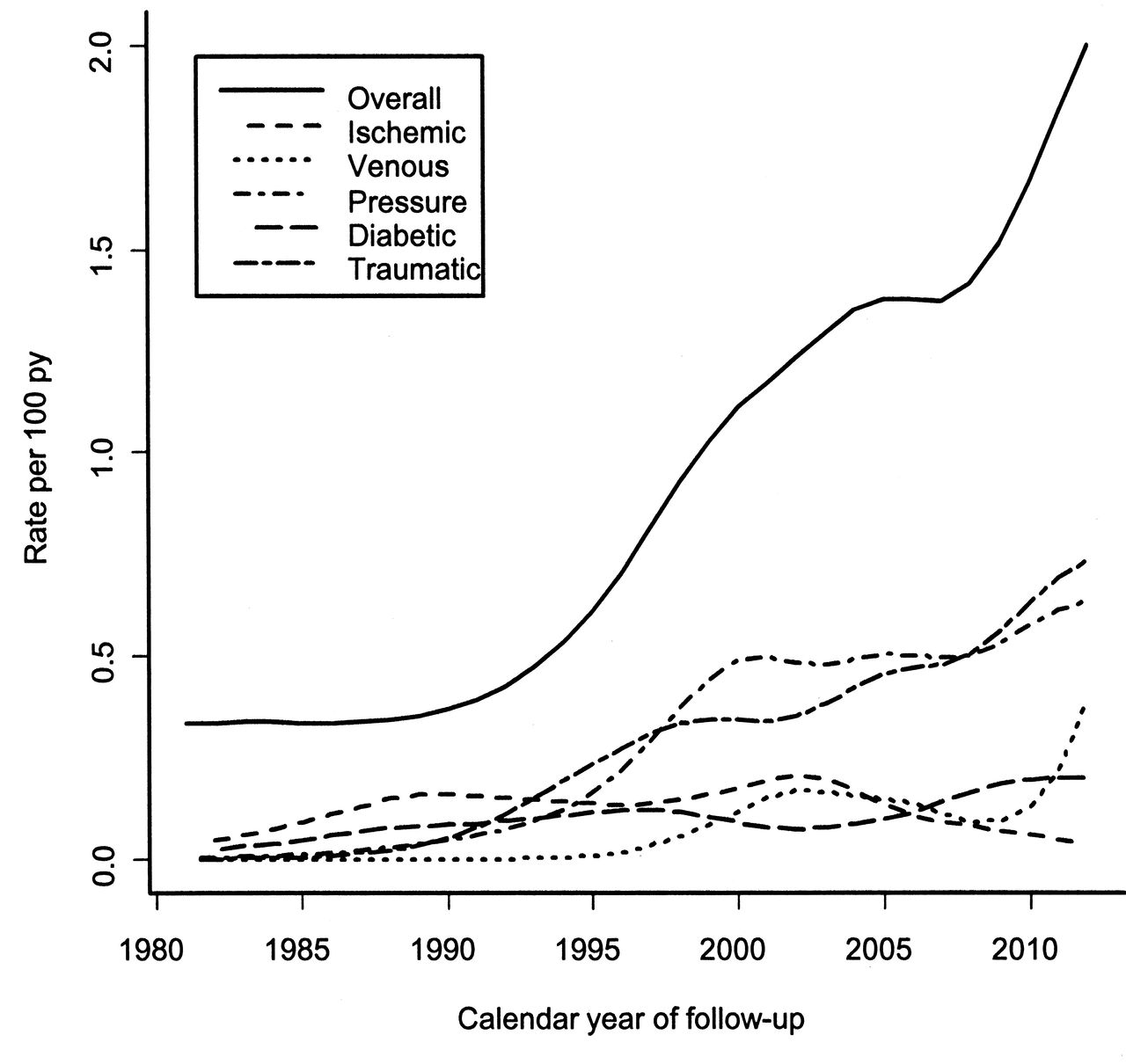
Rate of lower extremity ulcer incidence overall and by type among patients with incident rheumatoid arthritis, by calendar year of followup.
Risk factors for lower extremity ulcers in patients with rheumatoid arthritis (RA).
The following were identified as risk factors for LE ulcers in RA: age, RF positivity, history of BMI < 20 kg/m2, presence of rheumatoid nodules, radiological erosions/destructive changes, ESR ≥ 60 mm/h on 3 occasions, and severe extraarticular RA. Venous thromboembolism was also significantly associated with the development of LE ulcers, and several other comorbidities (DM and CV disease) had elevated HR, but did not reach statistical significance. Regarding medications, MTX exposure was significantly associated with the development of LE ulcers, and both biologic agents and glucocorticosteroids demonstrated elevated risks that did not reach statistical significance.
During followup, 229 patients died. LE ulcers in RA were associated with an increased mortality rate (HR 2.42; 95% CI 1.71, 3.42) adjusted for age, sex, and calendar year. This increased risk persisted following additional adjustment for RA disease characteristics and comorbidities known to influence mortality in RA (HR 2.38; 95% CI 1.63, 3.46), indicating the influence of LE ulcers on mortality in RA may not be explained by other factors.
DISCUSSION
Although the association of LE ulcer with RA was recognized by the 1950s13,14, LE ulcers in RA continue to be a major concern, with prolonged wound healing and morbidity, but are inadequately studied compared to, for example, diabetic foot ulcers2.
A postal survey of all patients with RA under the care of rheumatologists at the Bradford teaching hospitals in the UK estimated an overall prevalence of foot ulcers at 9.73%, with a prevalence of 3.39% in RA2. This postal survey was not a population-based study and had a 78% response rate; it excluded ulcers above the level of malleolus. Thirty-four percent of the episodes of LE ulcers in our study were located above the level of malleolus. The other common locations of ulceration noted in our study were tips of toes and plantar aspect of metatarsal heads, which is consistent with the UK study2. More than 1 site in the lower extremity was involved in a significant proportion of patients in our study. Pressure ulcers were the most common type in our study, followed by ischemic ulcers. This may be related to the fact that RA is associated with subclinical peripheral arterial disease15. Immobility, reduced ankle movement, and venous thrombosis can predispose the patients with RA to calf pump failure, which is associated with formation of venous ulcers, usually located over the medial malleolus and often associated with pedal edema16.
Only 1% of the episodes in our study had biopsy-proven rheumatoid vasculitis (RV). Because the majority of the patients did not undergo biopsy, it is unclear whether vasculitis was underdiagnosed. In an institution-based study on lower extremity ulcers in RA, 16 of 366 patients had active LE ulcers in a 3-year period and 12 of the 16 underwent biopsy. Of those 12, 3 had histopathological evidence of vasculitis17. RV typically presents as a painful deep cutaneous ulcer with a punched out appearance in the area of medial or lateral malleoli. Medium-vessel vasculitis could also potentially lead to digital ischemia and gangrene18. In a small prospective study from Sweden, 11 of 19 patients with RA and chronic leg ulcers had histopathological evidence of vasculitis19. However, this study included exclusively patients with non-healing leg ulcers for > 2 months’ duration.
We assessed risk factors for LE ulcers in RA, although a formal cohort study with a control group was not performed. Age and venous thromboembolism were identified as risk factors for LE ulcers in RA, which is not surprising because they are known risk factors for LE ulcers in the general population. It is unclear whether increased disease activity of RA is associated with LE ulcer, although disease severity indicators such as presence of rheumatoid nodules, ESR ≥ 60 mm/h on 3 occasions, and presence of extraarticular features were identified as risk factors. Other factors such as deformities secondary to RA and the reduced mobility of these patients may also lead to the development and healing of the LE ulcers.
A preliminary investigation in the UK with a small sample population compared 15 patients with RA and foot ulcer with 66 control RA patients without foot ulcer and suggested that active RA disease and current glucocorticosteroid therapy were associated with foot ulcer, whereas abnormal sensation, foot deformity, and raised plantar pressures were not20. Foot deformity, ill-fitting shoes, and appliances can predispose these patients to ulcers from local trauma or pressure21.
While skin atrophy in RA with prolonged glucocorticosteroid use may predispose the skin to break or tear with minor trauma, we found a marginal association between glucocorticosteroid use and LE ulcers in our subjects, which did not reach statistical significance22. The effect of glucocorticosteroid and other medications on the development of LE ulcers is unclear, and may be confounded by disease activity. Use of DMARD and biologics in RA was also marginally associated with LE ulcer in our study, but these associations did not reach statistical significance. Others have reported that treatment with a biological agent was associated with an increased likelihood of healing of LE ulcers in patients with RA17. Three of the 16 patients with LE ulcers in our study17 had biopsy-proven vasculitis, but it is unclear whether these results can be generalized because the sample size was small. Vasculitis was less common in LE ulcers in patients with RA in another institution-based retrospective study of hospitalized patients from a dermatology service23.
The cumulative incidence of LE ulcers steadily increased by 1% every year after RA diagnosis. We found no increased risk of LE ulcers with increasing duration of RA, which is in contrast to the UK study2. The recurrence rate was high among the patients with RA who had already experienced an episode of LE ulcer. LE ulcers occurred more frequently in recent years (1995 to 2007) than previous years (1980 to 1994). The reasons for this increase in occurrence are unclear; it cannot be excluded that improved documentation in the electronic medical records in recent years may have affected this result.
Owing to their protracted course, LE ulcers may reduce the quality of life of patients with RA. A significant proportion of patients in our study required surgical limb amputation, a finding that emphasizes the magnitude of morbidity in these patients. RA itself has an increased risk of mortality compared to the general population, mostly attributed to increased risk of CV death24. In our study, LE ulcers were associated with double the mortality rate in RA. This is the first study to find an association with LE ulcers and increased mortality in RA. The reasons for increased mortality are unclear and the increased risk persisted after adjusting for factors previously known to be related to mortality. Thromboembolism, one of the adjusted factors, was also found to be a risk factor for LE ulcers.
The strengths of our study are that it was population-based and targets an inadequately studied yet common problem in patients with RA. A major strength is that our study includes both nonhospitalized and hospitalized patients, so it does not have hospital or geographic referral bias. With the exception of a higher proportion of the working population employed in the health care industry, and correspondingly higher education levels, on the whole, the results of our study using the population of Olmsted County are generalizable to the populations of interest elsewhere25. Study weaknesses are those inherent in the retrospective design. Only those persons who had a medical encounter during a leg ulcer event could be identified and included. Events of leg ulcers in persons not seeking medical care for this problem or whose diagnosis was miscoded would not be identified. The wound characteristics were not well described in the charts of several of the LE ulcers. Some of the minor LE ulcers may not have been reported to the physician by the patient and hence were not documented in the records.
Because LE ulcers are a major problem for patients with RA, a good lower extremity examination and early diagnosis and treatment may help reduce the morbidity associated with them. Heightened awareness of this complication on the part of patients and healthcare providers is vital to ulcer prevention and management. RA patients with LE ulcers need to be managed using a multidisciplinary approach involving rheumatologists, wound care nurses, podiatrists, and people in other disciplines such as vascular medicine or dermatology as needed.
Footnotes
-
Supported by a grant from the US National Institutes of Health (NIH), the US National Institute of Arthritis and Musculoskeletal and Skin Diseases (R01 AR46849), the Rochester Epidemiology Project (R01 AG034676 from the National Institute on Aging), and Grant Number UL1 TR000135 from the National Center for Advancing Translational Sciences. The article’s contents are solely the responsibility of the authors and do not necessarily represent the official views of the NIH.
- Accepted for publication November 19, 2013.








{kind=link}
{kind=link}