

Abstract
Objective. Methotrexate-associated lymphoproliferative disorders (MTX-LPD) often regress spontaneously during MTX withdrawal, but the prognostic factors remain unclear. The aim of our study was to clarify the clinical, histological, and genetic factors that predict outcomes in patients with MTX-LPD.
Methods. Patients with MTX-LPD diagnosed between 2000 and 2012 were analyzed retrospectively regarding their clinical course, site of biopsy, histological typing, Epstein-Barr virus (EBV) in situ hybridization and immunostaining, and HLA type.
Results. Twenty-one patients, including 20 with rheumatoid arthritis (RA) and 1 with polymyositis, were analyzed. The mean dose of MTX was 6.1 mg/week and the mean duration of treatment was 71.1 months. Clinically, 5 patients were diagnosed with EBV-positive mucocutaneous ulcer (EBVMCU) and had polymorphic histological findings. The proportion of those patients successfully treated solely by withdrawal of MTX was significantly greater than that of those without EBVMCU (75% vs 7.7%, p = 0.015). The HLA-B15:11 haplotype was more frequent in patients with EBV+ RA with MTX-LPD than in healthy Japanese controls (p = 0.0079, Bonferroni’s method). EBV latency classification and HLA typing were not associated with the prognosis of MTX-LPD in our cohort.
Conclusion. Our data demonstrate that patients in the EBVMCU, a specific clinical subgroup of MTX-LPD, had a better clinical outcome when MTX was withdrawn than did other patients with MTX-LPD.
Methotrexate (MTX)-associated lymphoproliferative disorders (LPD) are a lymphoid proliferation or lymphoma that occur in patients immunosuppressed with MTX, classified as a part of the “other iatrogenic immunodeficiency-associated lymphoproliferative disorders” category by the World Health Organization (WHO) in 20081. Because MTX has recently gained acceptance as a first-line therapy for rheumatoid arthritis (RA)2,3 and other systemic rheumatic diseases (SRD), the incidence of MTX-LPD is expected to increase. A better understanding of this important disease is somewhat limited by its rarity. Epstein-Barr virus (EBV) infection is thought to play an important role in the pathogenesis of MTX-LPD, although EBV can only be detected on histopathologic examination in about half the cases of MTX-LPD4.
Under normal circumstances, EBV-specific cytotoxic T lymphocytes (EBV-CTL) act to suppress EBV-infected B cells. However, if the function of EBV-CTL is impaired by immunosuppressants, such as MTX or by aging, EBV-infected B cells are reactivated to induce B cell proliferation, leading to the development of LPD. There is speculation that MTX could reactivate latent EBV infection, because patients with SRD treated with regimens that include MTX have higher mean EBV loads in their blood than those who do not5. EBV-related LPD (EBV-LPD) can be categorized into 3 types on the basis of their expression of EBV-encoded small RNA (EBER), EBV latent membrane protein-1 (LMP1), and EBV nuclear antigen-2 (EBNA2): latency I (EBER+, LMP-1–, EBNA2–) as seen in Burkitt’s lymphoma; latency II (EBER+, LMP-1+, EBNA-2–) as seen in Hodgkin’s lymphoma or nasopharyngeal carcinoma; and latency III (EBER+, LMP-1+, EBNA-2+) as seen in posttransplant LPD (PT-LPD)6. EBV-LPD frequently occurs in immunosuppressed patients and its prognosis appears to vary widely.
LPD with EBV-positive mucocutaneous ulcer (EBVMCU) has been reported as a distinct disease entity with a self-limiting and indolent clinical course7. EBVMCU is found in various conditions of immunosuppression, including MTX-LPD or in age-related immunosenescence. The latter is characterized by age-related EBV+ B cell LPD (Age-LPD) on a background of EBV infection in elderly patients without immunodeficiency8. Although MTX-LPD often shows spontaneous regression, it is not clear whether MTX-LPD with EBVMCU has a better prognosis. The aim of our study was to clarify the clinical, histological, and genetic factors predictive of a good prognosis in patients with MTX-LPD.
MATERIALS AND METHODS
Patients
Twenty-one patients with SRD who developed MTX-LPD between 2000 and 2012 were included in our study. There were 20 with RA and 1 with polymyositis (PM). Of the 20 patients with RA, 3 had RA overlapping with Sjögren syndrome (SS), 1 had RA with systemic lupus erythematosus (SLE), and 1 had RA with polymyalgia rheumatica (PMR). The diagnoses of RA, PM, SS, SLE, and PMR were made according to the American College of Rheumatology classification criteria. The stage of RA was evaluated by Steinbrocker’s classification and the stage of LPD by Ann Arbor classification. After the histologic diagnosis of MTX-LPD was made, MTX was withdrawn in all patients. Necessity of chemotherapy was determined according to the histology, karyotypes, stages, or clinical judgment of poor response to MTX withdrawal.
Ethics statement
The study was conducted in compliance with the Declaration of Helsinki and was approved by the Kyoto University Ethics Committee Review Board; written informed consent was obtained from all patients.
Histological analysis
Two pathologists performed histological analysis of specimens from each patient. Diagnoses were made in accordance with the criteria specified in WHO Tumors of Hematopoietic and Lymphoid Tissues, fourth edition1. Immunostaining of paraffin sections was performed using monoclonal antibodies against LMP1 (Clone CS.1–4, Dako) and EBNA2 (M7004, PE2, Dako). The presence of EBER was determined by in situ hybridization (ISH) using a peptide nucleic acid (PNA) ISH detection kit (K5201, Dako) and an EBER PNA Probe/Fluorescein kit (Y5200, Dako).
Typing of HLA
HLA-A, B, and DR typing studies of 16 cases of RA with MTX-LPD and 96 control cases of RA without MTX-LPD diagnosed in our department were undertaken using the PCR-Luminex method. The frequency of each HLA allele was analyzed with reference to the Japanese HLA laboratory database (http://hla.or.jp/haplo/haplonavi.php?type=haplo&lang=ja), which includes over 20,000 cases.
Statistical analysis
Data are expressed as mean ± SD. Comparisons of HLA and histological data were made using Fisher’s exact test. Each allele seen in more than 2 cases was assessed with significant level corrected p value (Pc) by Bonferroni’s method. A Kaplan-Meier plot of the chemotherapy-free survival was evaluated by the log-rank test. All analyses were performed using PASW Statistics 18 (18.0.0) and statistical significance was defined as p < 0.05.
RESULTS
Clinical and pathological details of patients with MTX-LPD
The clinical, pathological, and genetic characteristics of 21 cases of MTX-LPD are shown in Table 1; 17 (81%) were female; the mean age was 65.8 ± 7.5 years (range 52 to 79 yrs). The average dose of MTX was 6.1 ± 1.7 mg/week; treatment duration was 71.1 ± 57.8 months. Staging of RA was undertaken using Steinbrocker’s classification; 1 patient fulfilled the criteria for stage I, 3 for stage II, 3 for stage III, and 13 for stage IV. Three patients (cases 1, 5, and 15) were treated with infliximab. Seventeen out of 20 RA cases (85%) were rheumatoid factor (RF)-positive and 7 out of 14 cases (50%) were anticitrullinated protein antibody (ACPA)-positive.
Clinical and pathological findings in 21 cases of methotrexate-associated lymphoproliferative disorders (MTX-LPD).
The pathological findings were as follows: 10 cases were diagnosed with diffuse large B cell lymphoma (DLBCL), 7 with polymorphic lymphoproliferative disorder (p-LPD), 3 with HL, and 1 with small B cell lymphoma that later transformed into DLBCL. The biopsy site was extranodal in 12 cases (57%); all 7 cases of p-LPD were extranodal, while 3 cases of HL were nodal. Of the 10 cases of DLBCL, half were extranodal and half nodal. Twelve out of 20 cases (60%) were EBER-positive, while 8 cases of 19 (42%) were LMP1-positive and 3 cases out of 19 (16%) were EBNA2-positive. EBV latency was classified by means of EBER, LMP1, and EBNA2 expression into 4 groups: EBV-negative and latencies I–III. Representative histological images are shown in Figure 1. The cases diagnosed as p-LPD comprised 7 of the 12 patients in latency I–III groups; but there were none among the 8 patients in the EBV-negative group (p = 0.012). Extranodal involvement was found in 8 of 12 patients in the latency I–III groups but only 3 of 8 in the EBV-negative group. EBVMCU was diagnosed in 5 cases (cases 1, 2, 4, 5, and 21), each characterized by sharply demarcated skin ulcers with an erythematous appearance accompanied by crusting and necrosis (Figure 2) which, on histological examination, were found to be polymorphic with a mixture of lymphocytes and immunoblasts. Lymphocytic vasculitis was seen in 3 out of 5 cases (cases 2, 5, and 21). Four out of 5 cases (80%) of EBVMCU were seropositive.

Pathological findings in 3 cases of MTX-LPD classified by EBV latency. A–D. DLBCL (case 10, latency I). E–H. Polymorphic LPD (case 4, latency II). I–L. Polymorphic LPD (case 3, latency III). Pathological findings are shown by H&E (A, E, I), EBER (B: positive, F: positive, J: positive), LMP1 (C: negative, G: positive, K: positive), and EBNA2 (D: negative, H: negative, L: positive) staining. MTX-LPD: methotrexate-associated lymphoproliferative disorders; EBV: Epstein-Barr virus; DLBCL: diffuse large B cell lymphoma; EBER: EBV-encoded small RNA; LMP1: EBV latent membrane protein-1; EBNA2: EBV nuclear antigen-2.
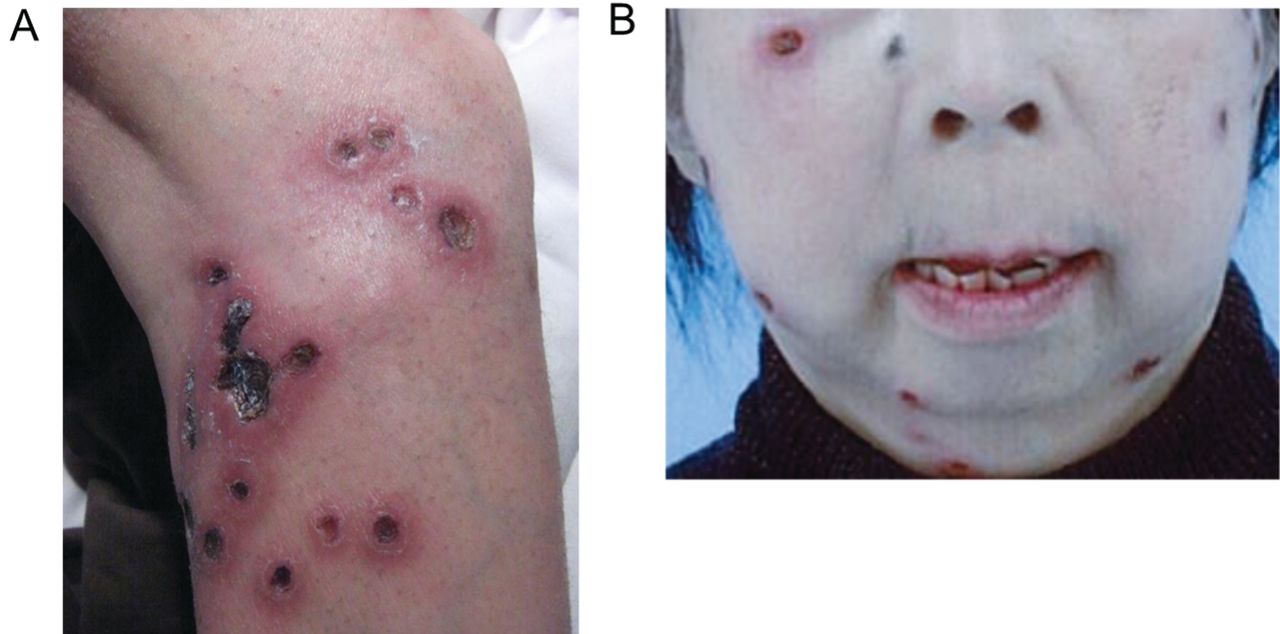
Two representative cases with skin manifestations of EBV-positive mucocutaneous ulcer (EBVMCU). Typical skin manifestations of EBVMCU (A: case 5, B: case 2) are shown. Characteristic sharply demarcated skin ulcers with an erythematous appearance accompanied by crusting and necrosis can be seen.
HLA typing of patients with MTX-LPD
As shown in Table 2, we found that 3 cases out of 16 were heterozygous for the HLA-B15:11 allele. The allele frequency of HLA-B15:11 was higher in EBV+ RA with MTX-LPD, compared with the control JHD group and that of the Japanese RA cohort (Pc = 0.0079 and 0.024, respectively, Table 3). RA-shared epitopes were observed in 11 of 16 cases (69%), a significantly higher proportion than in healthy Japanese controls (38%, n = 1508; p = 0.018), but not in Japanese patients with RA (n = 759)9.
HLA-A, B, and DR alleles of 16 cases of RA with MTX-LPD.
Risk allele of RA with MTX-LPD in Japanese population.
Clinical course of patients with MTX-LPD
MTX was withdrawn in all cases at the time of LPD diagnosis. When examining the need for chemotherapy within 18 months of diagnosis, withdrawal of MTX alone was more successful for those in the EBVMCU group (n = 4, cases 1, 4, 5, and 21) than the other cases (n = 13; 75% vs 7.7%, p = 0.015; Figure 3). Because the observation periods were at most 2 years in the majority of cases, we were unable to calculate longterm prognosis. Five patients (cases 2, 7, 8, 9, and 12) died; LPD recurred in 2 patients at 90 months (case 9) and 21 months (case 12) from the original diagnosis and did not respond to continued chemotherapy. One patient (case 2) died from intercurrent myelitis and sepsis soon after the diagnosis of LPD and 1 patient (case 7) died from bleomycin-induced pneumonia.
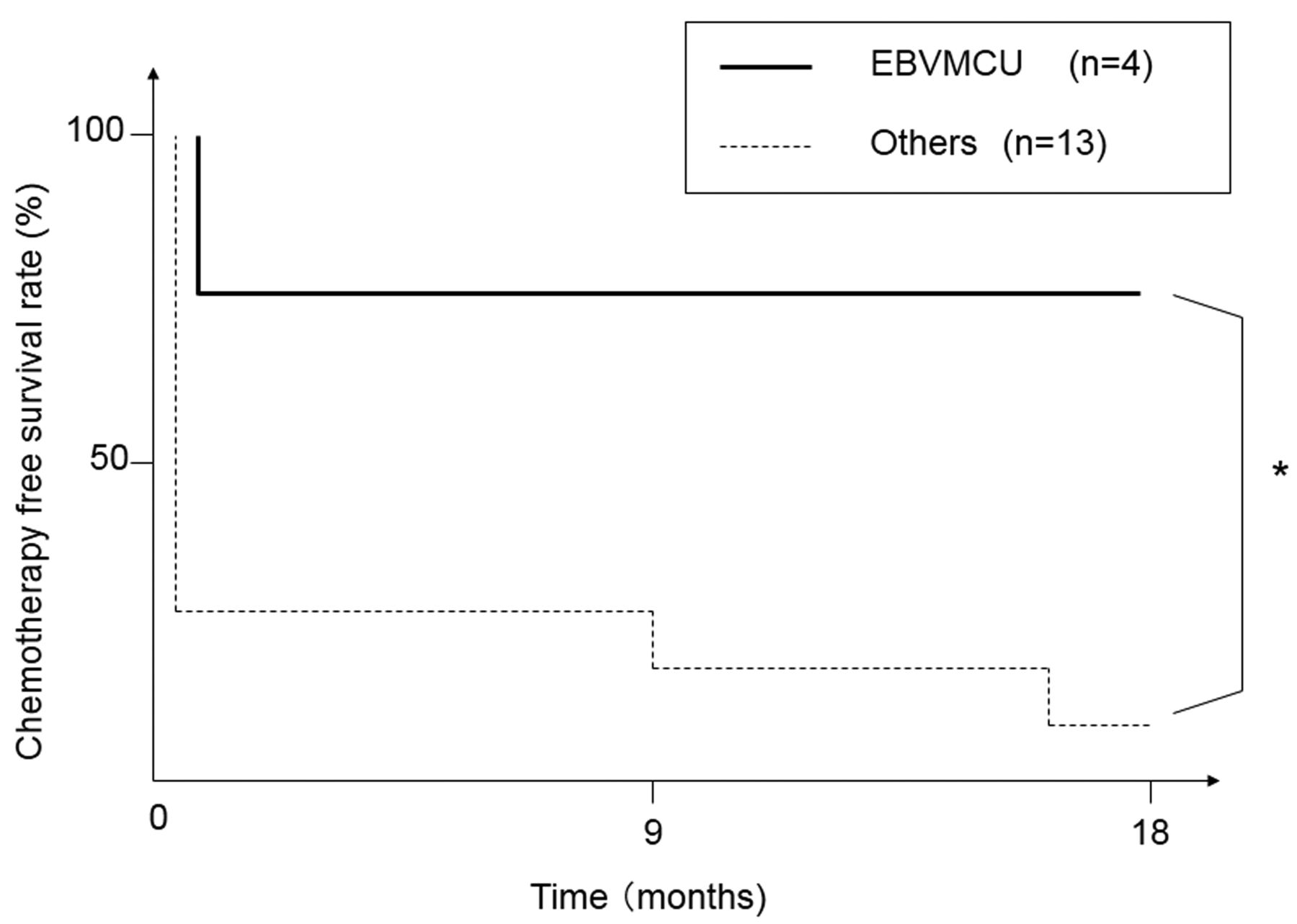
Chemotherapy-free survival. Kaplan-Meier curve shows chemotherapy-free survival within 18 months, comparing patients in the EBV-positive mucocutaneous ulcer (EBVMCU) group with those with other forms of MTX-LPD. Methotrexate was withdrawn in all cases. *Log-rank test, p < 0.05. MTX-LPD: methotrexate-associated lymphoproliferative disorders; EBV: Epstein-Barr virus.
One patient (case 8) was first diagnosed with EBV-positive small B cell lymphoma (SBL). Although chemotherapy resulted in partial remission, she had an indolent clinical course without chemotherapy until the tumor progressed and histopathological study revealed EBV-negative DLBCL with the same phenotype as the SBL. A clonal relationship between the 2 lymphomas was not proven; however, Richter syndrome was suspected clinically. With regard to the predicted unfavorable prognosis, she was treated with autologous peripheral blood stem cell transplantation, but she died of pneumocystis pneumonia under continuous immunosuppression. Although 2 cases of EBVMCU (cases 2 and 5) were included in Ann Arbor stage IV, each had a favorable clinical outcome.
DISCUSSION
We have shown that the presence of EBVMCU appears to confer a better prognosis in patients with MTX-LPD. Most of our patients with positive outcomes had been diagnosed with EBVMCU. Of the 12 cases of MTX-LPD with mucocutaneous ulcer reported in the literature7,10,11,12,13,14,15,16,17 all except 117 were EBV-positive and all 9 cases with available data showed complete remission without chemotherapy.
EBVMCU was first reported to be a favorable prognostic indicator in a case series of 26 patients (consisting of 19 with Age-LPD and 7 with iatrogenic immunodeficiency-associated LPD including 4 with MTX-LPD)7, but the incidence of EBVMCU in MTX-LPD was not known. Our study shows that the incidence of EBVMCU in EBV+ MTX-LPD is 42% (5 out of 12), which is higher than that of EBVMCU in Age-LPD (13%, 16 cases out of 122)18.
Age-LPD is believed to be a consequence of an underlying immunological deficit, or immunosenescence of the T cell receptor (TCR) repertoire19,20 — a natural degeneration of the immune system that occurs with aging. Considering the high average age of our cases, age-related immunosenescence might be partly involved in the development of MTX-LPD. This may be revealed by decreases in the TCR repertoire in the future.
Only a few cases of EBV latency in MTX-LPD have been reported; those of EBV latency among MTX-LPD, PT-LPD, and Age-LPD are summarized in Table 421,22,23. Other case series include 53 cases of LPD in a variety of autoimmune diseases, including 4 cases of MTX-LPD, in which all 16 cases of EBV+ LPD were in latency II24. Taken together, these data suggest that EBV+ MTX-LPD is more likely to be in latency II, followed by latency III. This observation also appears to hold true for PT-LPD and Age-LPD. PT-LPD has been generally categorized as latency III25, but is often seen to be in latency II. Cases of Age-LPD were also found to be mainly in latency II. Nonetheless, the latency classification had no value in predicting the prognosis of MTX-LPD in our cohort. The utility of EBV latency in MTX-LPD remains unknown.
EBV latency classification among MTX-LPD, PT-LPD, and Age-LPD.
Although the pathogenesis of EBVMCU is unclear, lymphocytic vasculitis was observed in more than half our cases of EBVMCU. In EBV-positive LPD, the Mig monokine, induced by interferon-γ (IFN-γ), and IFN-γ inducible protein-10 (mainly produced by reactive cells including endothelial cells) are thought to be powerful instigators of vascular and tissue injuries26. Thus, we hypothesize that tissue necrosis and the impairment of local blood flow to the area of vascular damage might be pivotal to the pathogenesis of EBVMCU. Although it is unclear why patients with MTX-LPD who developed EBVMCU had a better prognosis, several factors might be responsible. One possibility is that the mucocutaneous ulcer is so conspicuous that patients seek medical help more promptly, when diagnosis is relatively straightforward and the disease is in an earlier, potentially reversible stage. Thus, the prompt cessation of MTX may lead to a good outcome.
Our study is the first, to our knowledge, to have conducted HLA typing, revealing that HLA-B15:11 could be a risk allele in EBV+ RA with MTX-LPD. Notably, all 3 HLA-B15:11-positive cases were EBV-positive and 2 were polymorphic, indicating that this allele may be linked to the susceptibility to EBV infection and development of LPD. In our study, HLA-B15:11 had no correlation with HLA-shared epitopes, RF, or ACPA. To the best of our knowledge, there have been no reports of any relationship between this allele and other diseases. The identification of a genetic risk factor could help to clarify the pathogenesis of LPD and to achieve safer therapy for patients who might be at risk of LPD if their RA is treated with MTX. Because this is a retrospective study, there are some limitations, and a larger scale prospective trial is needed to clarify the pathogenesis of this disease.
We have demonstrated that cases of EBVMCU, a subgroup of MTX-LPD, were all histologically polymorphic and had a more favorable outcome by withdrawing MTX alone. In addition, we found that the frequency of the HLA-B15:11 allele was significantly increased in our cohort, which suggests that it may be a risk factor for EBV+ RA with MTX-LPD.
Acknowledgment
The authors thank Dr. Toda (Kyoto University, Center for Anatomical Studies) for performing immunostaining studies and Dr. Inoko (Tokai University, Department of Molecular Science) for kindly providing the HLA reference data of Japanese patients with rheumatoid arthritis.
- Accepted for publication October 8, 2013.








{kind=link}
{kind=link}
{kind=link}