

Abstract
Objective. To measure concentrations of high-sensitivity cardiac troponin (HS-cTnT) and N-terminal pro-brain natriuretic peptide (NT-proBNP) in patients with rheumatoid arthritis (RA) and to examine correlates.
Methods. The plasma concentrations of HS-cTnT and NT-proBNP were measured in consecutive patients with RA and compared to values obtained from age-matched and sex-matched healthy controls.
Results. We included 236 unrelated patients with RA (192 females, 57 ± 13 yrs) and 213 controls (170 females, 55 ± 15 yrs). Seventy-one patients with RA were free of cardiovascular (CV) risk factors. HS-cTnT and NT-proBNP concentrations were significantly higher in the total cohort of patients with RA (p = 0.03 and p < 0.0001, respectively) and in the subgroup free of CV risk factors (p = 0.02 and p < 0.0001, respectively) compared to controls. In addition, both the total cohort of patients with RA and the subgroup free of CV risk factors were more likely to have levels above the cutoff concentrations of HS-cTnT (p = 0.003 and p = 0.007, respectively) and NT-proBNP (p = 0.0001 and p < 0.0001, respectively) than controls. Patients with RA and increased C-reactive protein (CRP) levels had higher HS-cTnT (p = 0.03) and NT-proBNP (p = 0.02) concentrations. HS-cTnT levels positively correlated with the 28-joint Disease Activity Score (DAS28-CRP; r = 0.2, p = 0.020). Multivariate logistic regression analysis indicated that increased HS-cTnT levels were independently associated with a DAS28-CRP > 5.1 (OR 11.8; 95% CI 1.6–35.5) and a body mass index > 30 kg/m2 (OR 2.7; 95% CI 1.3–5.5).
Conclusion. HS-cTnT and NTproBNP are increased in patients with RA, independent of CV risk factors. The association between HS-cTnT, NT-proBNP, and CRP, together with the correlation between HS-cTnT and disease activity, support the link between myocardial injury/dysfunction and inflammation.
- RHEUMATOID ARTHRITIS
- CARDIOVASCULAR
- BIOMARKER
- HIGH-SENSITIVITY CARDIAC TROPONIN
- MYOCARDIAL INJURY
- N-TERMINAL PRO-BRAIN NATRIURETIC PEPTIDE
Cardiovascular (CV) disease is now recognized as a major cause of morbidity and mortality in patients with rheumatoid arthritis (RA)1,2. Identifying patients with RA at a preclinical stage and/or at high risk of myocardial involvement is crucial because it may allow for the development of preventive strategies.
Recently, some biomarkers emerged as strong predictors of cardiac diseases, even in a very early course of the disease. These include troponins and B-type natriuretic peptides (BNP). Cardiac troponins (cTn) are markers of myocyte necrosis and injury. Measured with highly sensitive (HS) assays, HS-cTn have proven to hold valuable prognostic value in various conditions, including patients with suspected acute myocardial infarction, chest pain, heart failure, and in low-risk populations3,4,5.
The N-terminal fragment of pro-BNP (NT-proBNP) is released concomitantly with BNP by ventricular myocytes, as a consequence of increased strain. NT-proBNP plasma levels have been shown to predict cardiac mortality and morbidity in the general population, as well as in cohorts of patients with heart failure and stable coronary heart disease6,7,8,9.
Scant information regarding these cardiac biomarkers is available on patients with RA. We measured the plasma levels of cTnT isoform (using a highly sensitive assay; HS-cTnT) and NT-proBNP in large populations of patients with RA and healthy controls to: (A) test the hypothesis that HS-cTnT and NT-proBNP may be increased in patients with RA compared to healthy controls, and (B) examine the relative contribution of traditional CV risk factors and characteristics in RA disease, including inflammatory markers, in their concentrations.
MATERIALS AND METHODS
Patients and control subjects
We performed a cross-sectional controlled study, including consecutive patients with RA, > 18 years of age, fulfilling the 1987 American College of Rheumatology (ACR) classification for RA, who have been treated at the Rheumatology A department of Cochin Hospital and Rheumatology department of Bichat Hospital, over a 9-month period10. Patients with RA were excluded if they had a history of coronary disease, ischemic stroke, heart failure, or abnormal plasma creatinine values. The control group consisted of 213 healthy controls recruited during a systematic screening at Tenon Hospital in Paris. The characteristics of the controls have already been reported in a study aimed at defining the 99th percentile cutoff point of HS-cTnT3. To that aim, to be enrolled healthy controls had to be at low CV risk after history, clinical examination, and blood analysis, including glucose and cholesterol tests. Exclusion criteria were smoking, body mass index (BMI) > 30 kg/m2, treated/untreated hypertension, known/symptoms of coronary artery disease, diabetes, dyslipidemia, and plasma creatinine values above the normal range. The local ethics committees approved the study and all the subjects gave written informed consent.
Data collection from patients with RA
History taking, physical examination, laboratory tests, and review of medical files were systematically performed. Current and past medication use was obtained from information provided by patients and based on the review of medical records. Blood pressure was measured from patients in a supine position for 10 min. Hypertension was defined as systolic blood pressure ≥ 140 mm Hg, diastolic blood pressure ≥ 90 mm Hg, or current use of antihypertensive medication. Diabetes was defined as fasting glucose ≥ 7 mmol/l (1.26 g/l) or current use of antidiabetic drug. Dyslipidemia included patients with low-density lipoprotein cholesterol ≥ 4.13 mmol/l (1.6 g/l) or current use of lipid-lowering drugs, high-density lipoprotein cholesterol < 1.03 mmol/l (0.4 g/l), triglyceridemia ≥ 1.69 mmol/l (1.5 g/l), or current use of fibrate. Current smokers were defined as subjects reporting at least 1 cigarette/day.
RA disease activity was assessed using the Disease Activity Score based on evaluation of 28 joints (DAS28)11, using the C-reactive protein (CRP). Surrogate measures of cumulative disease activity were health status and joint destruction. Health status was measured by the self-administered Stanford Health Assessment Questionnaire (HAQ). Systematic hand and foot radiographs were performed to measure joint destruction, defined by the presence of erosions.
Laboratory tests
Laboratory diagnostics were obtained from patients with RA on the morning of hospital admission. They included complete blood (cell) count, Westergren erythrocyte sedimentation rate (ESR; considered elevated above 28 mm/h), CRP concentration (considered elevated if above 10 mg/l), and serum creatinine concentration. Rheumatoid factor (RF) and second-generation anticyclic citrullinated peptide (anti-CCP2) antibodies were detected using ELISA.
Cardiac biomarkers
The plasma HS-cTnT concentrations were measured on an Elecsys 2010 analyzer, using an electrochemiluminescence immunoassay (Roche Diagnostic), as described3. According to the manufacturer, the measurement range of the assay is 3 to 10,000 ng/l. The 99th percentile, with a coefficient of variation (CV) ≤ 10%, is achieved for 14 ng/l12.
NT-proBNP concentrations were measured using an Elecsys NT-proBNP sandwich immunoassay (Roche Diagnostic), as described3,13. The analytical range of plasma NT-proBNP levels extended from 20 ng/l to 35,000 ng/l; the intraassay coefficient of variation was 2.5% for a concentration of 175 ng/l and 2% for a concentration of 1070 ng/l; the interassay coefficient of variation was 3.2% and 2.7%, respectively. Thresholds for high NT-proBNP concentrations (97th percentile of normal values, as determined by the manufacturer) according to age and sex are mentioned in Appendix 1.
The investigators performing the assays (CCG and DB) were blinded to the result of the clinical evaluations.
Statistical analysis
All data are presented as median (range) for continuous variables, and numbers and percentages for categorical variables, unless otherwise stated. Data were analyzed using the Mann-Whitney U test. Spearman’s rank correlation test was used to assess the relation between quantitative variables. Differences in frequency were examined using the chi-square test. Comparisons between levels of cardiac biomarkers according to disease activity (low disease activity, DAS28-CRP < 3.2; moderate disease activity, DAS28-CRP between 3.2 and 5.1; and high disease activity, DAS28-CRP > 5.1) were performed by using a nonparametric Kruskal-Wallis test.
Multivariate analysis was performed with logistic regression including all variables with p ≤ 0.1 univariately as covariates. For all of the study variables, 2-tailed p values < 0.05 were considered statistically significant.
RESULTS
Study population
Of the 261 patients with RA that were selected, 25 were not included because of coronary disease (n = 20) and ischemic stroke (n = 5). The final population consisted of 236 patients with RA (192 women, median age 57 yrs; range 24–87 yrs) and 213 controls (170 women, median age 55 yrs; range 21–90 yrs). Seventy-one patients with RA were free of traditional CV risk factors, including smoking, hypertension, diabetes mellitus, dyslipidemia, and obesity defined by a BMI > 30 kg/m2). Detailed characteristics are provided in Table 1.
Characteristics of patients with rheumatoid arthritis (RA).
Plasma levels of HS-cTnT and NT-proBNP in patients with RA compared to healthy controls
HS-cTnT levels positively correlated with NT-proBNP levels (r = 0.34, p < 0.0001) in patients with RA.
We first analyzed median plasma levels of cardiac biomarkers in the whole population of patients with RA versus healthy controls. HS-cTnT and NT-proBNP concentration were significantly higher in patients with RA than controls (Figure 1A, 1B). Patients with RA were more likely to have elevated HS-cTnT and NT-proBNP levels than controls [HS-cTnT > 14 ng/l: 16/236 patients (7%) with RA vs 2/213 controls (1%), p = 0.003; elevated NT-proBNP levels: 37/236 patients (16%) with RA vs 8/213 controls (4%), p = 0.0001].

Plasma levels of high-sensitivity cardiac troponin (HS-cTnT; A and C) and N-terminal pro-brain natriuretic peptide (NT-proBNP; B and D) in the whole population of patients with rheumatoid arthritis (RA) and in patients free of cardiovascular risk factors, compared to controls.
Then, to compare 2 homogeneous populations, we stratified patients with RA and healthy controls according to the lack of CV risk factors. Thus, we focused on the subset of patients with RA who were free of classical CV risk factors (n = 71), who were compared to healthy controls. Consistently, with the results observed in the whole RA population, this subgroup of patients with RA had significantly increased HS-cTnT and NT-proBNP plasma concentrations when compared to controls (Figure 1C, 1D). In addition, patients with RA without classical CV risk factors were also more likely to have concentrations above the cutoff value of HS-cTnT and NT-proBNP than controls [HS-cTnT > 14 ng/l: 6/71 patients (8%) with RA vs 2/213 (1%) controls, p = 0.007; elevated NT-proBNP levels: 20/71 patients (28%) with RA vs 8/213 (4%) controls, p < 0.0001].
Relationship between plasma levels of HS-cTnT/NT-proBNP and CV risk factors in patients with RA
Median HS-cTnT and NT-proBNP plasma levels did not differ between patients with RA with or without hypertension, diabetes mellitus, or dyslipidemia, as well as smoking habits (Figure 2A, 2B, 2C, 2D, 2E, 2F, 2G, 2H, 2J). A trend was observed for increased HS-cTnT levels in patients with BMI > 30 kg/m2 (p = 0.1; Figure 2I). In agreement with these results, none of these CV risk factors were associated with above the cutoff value concentrations of Hs-cTnT or NT-proBNP, except a trend observed between HS-cTnT > 14 ng/l and a BMI > 30 kg/m2 (p = 0.05; Table 2).
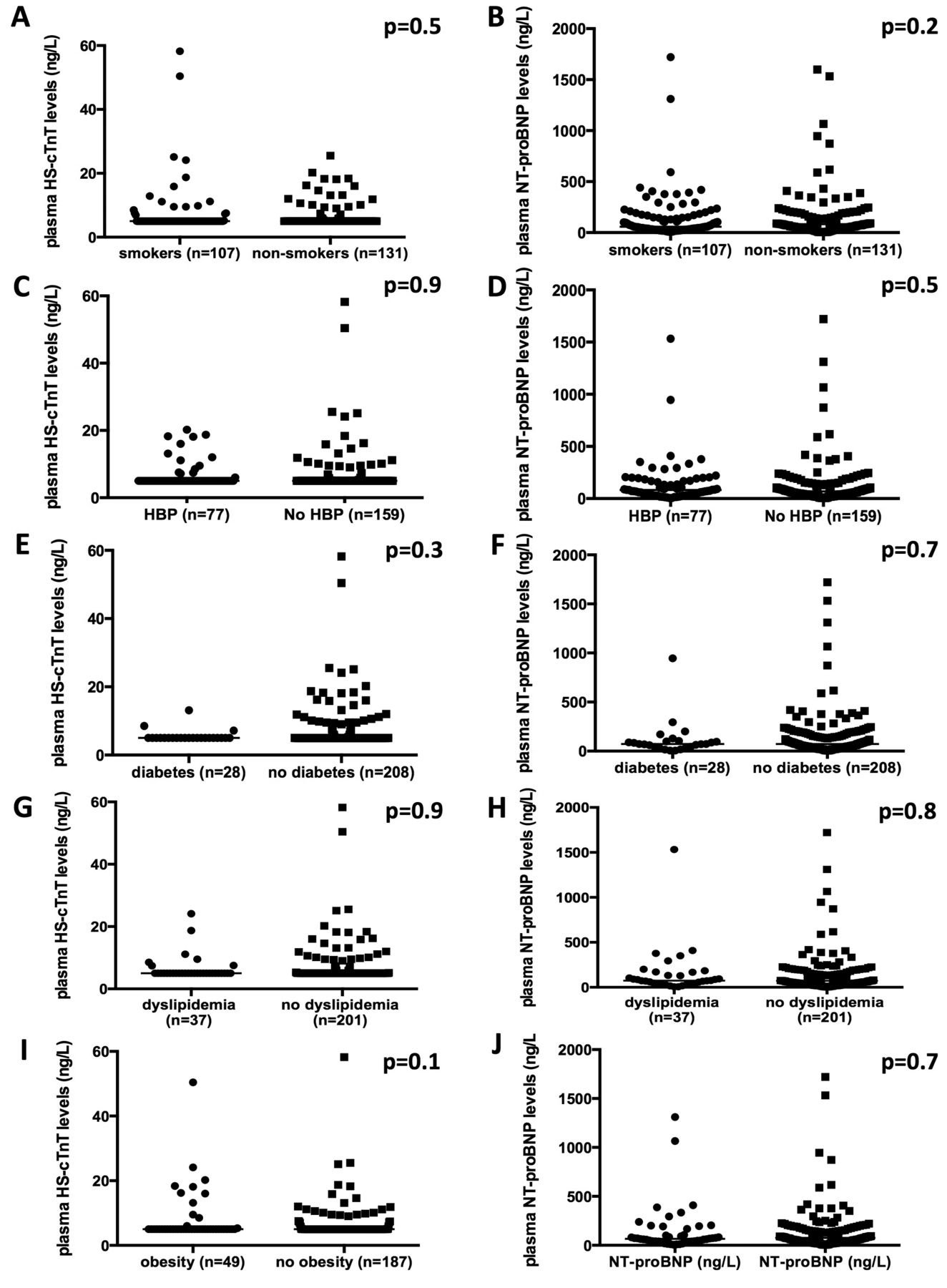
Influence of classical cardiovascular risk factors, including smoking (A and B), high blood pressure (HBP; C and D), diabetes (E and F), dyslipidemia (G and H), and obesity (I and J), on median plasma levels of high-sensitivity cardiac troponin (HS-cTnT) and N-terminal pro-brain natriuretic peptide (NT-proBNP).
Multivariate logistic regression analysis including increased high-sensitivity cardiac troponin (HS-cTnT) levels (> 14 ng/l) as the dependent variable. Data are n (%) unless otherwise indicated.
Relationship between plasma levels of HS-cTnT, NT-proBNP, and RA disease characteristics
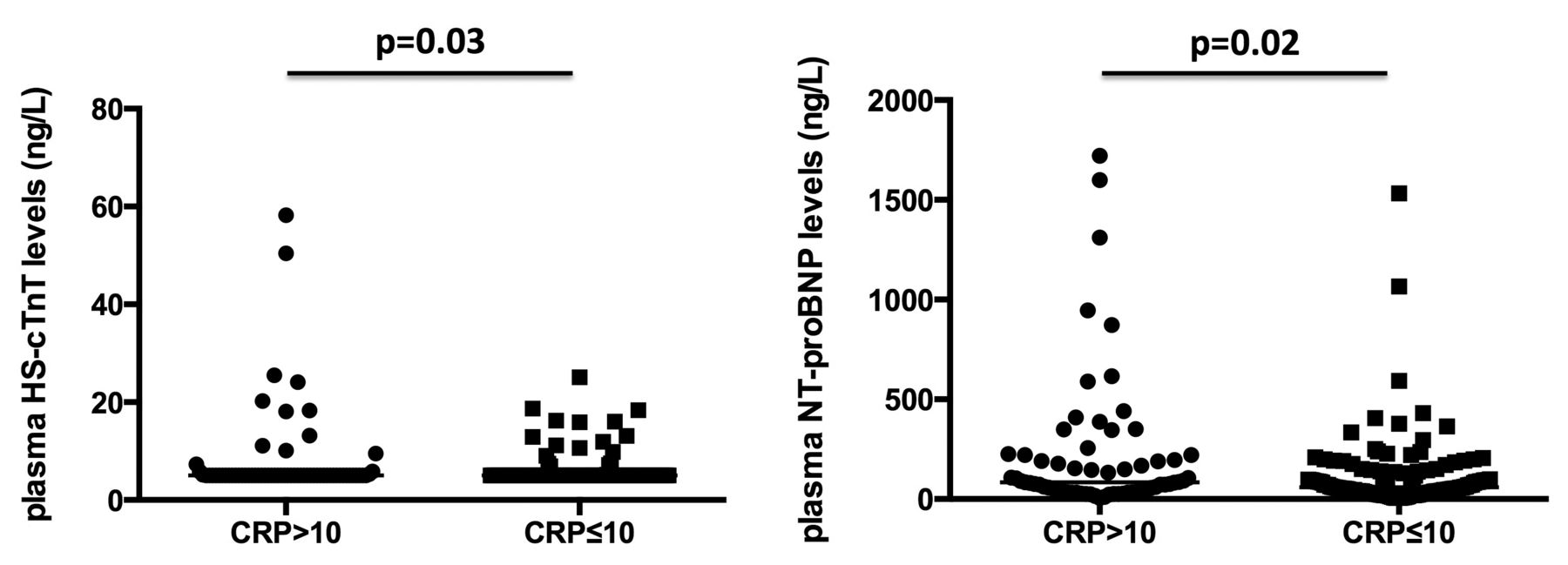
Patients with CRP > 10 mg/l were more likely to display significantly increased median plasma levels of HS-cTnT and NT-proBNP (p = 0.03 and p = 0.02, respectively; Appendix 2). In addition, HS-cTnT levels positively correlated with the DAS28-CRP (r = 0.2, p = 0.02; Figure 3A). Indeed, patients with high disease activity, defined by a DAS28-CRP > 5.1, had increased median HS-cTnT concentrations when compared with patients with mild or moderate disease activity (Figure 3B). Patients with increased HS-cTnT concentrations (> 14 ng/l) were also more likely to have CRP levels > 10 mg/l and a DAS28-CRP > 5.1. No association was observed between disease activity and NT-proBNP levels.

(A) Correlation between high-sensitivity cardiac troponin (HS-cTnT) plasma levels and the Disease Activity Score based on evaluation of 28 joints, using the C-reactive protein (DAS28-CRP). (B) Median HS-cTnT levels according to disease activity assessed by the DAS28-CRP: low disease activity was defined by a DAS28-CRP ≤ 3.2, moderate disease activity by DAS28 > 3.2 and ≤ 5.1, and high disease activity by DAS28-CRP > 5.1.
No significant association or correlation between median HS-cTnT/NT-proBNP plasma levels and radiographic erosions, Health Assessment Questionnaire, antibody status, or current treatment regimen was observed, while there was trend between increased HS-cTnT levels and the presence of positive rheumatoid factors (p = 0.08; Table 2).
In a logistic regression model including all variables with a p value ≤ 0.1 as covariates, DAS28-CRP (OR 11.8, 95% CI 1.6–35.5) and a BMI > 30 kg/m2 (OR 2.7, 95% CI 1.3–5.5) were independently associated with increased HS-cTnT levels (> 14 ng/l; Table 2).
DISCUSSION
We examined the concentrations of HS-cTnT and NT-proBNP in 236 patients with RA and compared those concentrations to those obtained from healthy age-matched and sex-matched patients. Of the most interest, the elevation of the 2 markers in patients with RA was independent of CV risk profile, suggesting that elevated HS-cTnT and NT-proBNP levels may reflect subclinical myocardial damage and dysfunction caused by the disease itself. This is consistent with previous reports, which showed that heart failure in patients with RA is not explained by traditional CV risk factors, and neither solely by the presence of ischemic heart disease14,15.
Increased levels of inflammatory markers are associated with an increased risk of CV morbidity and mortality in the general population16. Moreover, disease activity in RA correlates with mortality, CV disease, and chronic heart failure17. Hence, the relationship between markers of inflammation/disease activity and cardiac biomarkers is of great interest. We report an association between CRP and NT-proBNP levels, which has only been reported once18. CRP levels were also associated with HS-cTnT concentrations and a positive correlation between HS-cTnT levels and the DAS28-CRP was identified. This result differs from another study, in which no association between HS-cTnI concentrations and acute phase reactants or the DAS28 was observed19. Although the median DAS28 and median CRP values were similar in both studies, this discrepancy might be related to the characteristics of patients included, because a high proportion of our patients had active disease, whereas patients in the previous study had a relatively well-controlled disease19.
The information given by cTn, CRP, and NT-proBNP might be pertinent to 3 distinct pathways (myonecrosis, inflammation, hemodynamic stress) that are thought to be involved in the pathogenesis of CV disease and acute coronary syndromes. These 3 biomarkers have demonstrated incremental value in identifying patients at higher risk of future myocardial infarction and death in the general population and in patients with acute coronary syndrome. Taken together, these results may suggest that systemic inflammation might induce myocyte necrosis and dysfunction, leading to the release of HS-cTnT and NT-proBNP. It is striking and challenging to observe that some patients with RA exhibit a concomitant increase in these 3 complementary markers. It might suggest that RA should be regarded as a model of inflammation that leads to myocardial damage. Of course, this hypothesis needs to be confirmed in dedicated experimental studies. In addition, the exact meaning of concomitant increase of these markers will need to be determined by the prospective followup of such patients with RA for the occurrence of CV events.
Other factors may explain elevated HS-cTnT in RA, including stunned or hibernating myocardium, and apoptosis or necrosis of myocytes secondary to subendocardial ischemia20,21,22,23. Increased circulating HS-cTnT was also associated in multivariate analysis with obesity, in agreement with previous data that reported a link between HS-cTnT, obesity, and metabolic syndrome24.
Radiographic damage and HAQ score are surrogate measures of cumulative disease activity. We did not find any association between cardiac markers and the presence of erosions or the HAQ, although it has been suggested once for NT-proBNP6. Previous reports on the association between joint destruction and CV disease in RA have been inconsistent; some reports suggesting that early progression of erosions increased the risk of CV events, and others did not find any association between joint erosions and CV death or myocardial infarction25,26. We observed a trend between HS-cTnT levels and positive rheumatoid factor, which did not persist in multivariate analysis. However, this association might not have achieved statistical significance because of the lack of power of our study.
Our study has several shortcomings that deserve consideration. We did not perform morphologic evaluation of cardiac function and did not investigate patients for possible silent coronary ischemia. In addition, we did not assess coronary artery calcification in the whole cohort of patients with RA. False positive elevation of cTnI has been reported in patients with seropositive RA, using the Beckman Access Immunoassay System and the microparticle enzyme immunoassay27,28. However, we focused on the T isoform and we used a completely different assay. Median disease duration was 13 years, highlighting that most of the patients had established RA. In such patients, ischemic lesions may have occurred without any symptoms, as in diabetes. Since we did not investigate ischemia in our RA population, the relationship between HS-cTnT and RA could be related to unknown ischemic lesions. Our study is also limited by its observational design and any pathogenic link that emerged from this type of study should be taken very cautiously. However, our study had a large sample size of patients carefully assessed and phenotyped in 2 tertiary centers with much experience in RA evaluation and care. Prospective studies will be needed to assess the temporal relationship between disease activity and cardiac biomarkers.
HS-cTnT and NT-proBNP plasma concentrations were increased in patients with RA independent of CV risk factors. Our results show, to our knowledge for the first time, an association between increased HS-cTnT concentrations, CRP levels, and high RA disease activity, which supports the link between myocardial injury and inflammation in this population. Increased HS-cTnT concentrations in RA may indicate subclinical, indolent myocardial injury, which may be related to myocardial dysfunction, supported by the positive correlation of HS-cTnT and NT-proBNP levels. Further studies are necessary to determine the merit of Hs-cTnT and NT-proBNP to predict CVD in RA.
APPENDIX 1.
Thresholds for high N-terminal pro-brain natriuretic peptide (NT-proBNP) plasma levels according to age and sex.
APPENDIX 2.
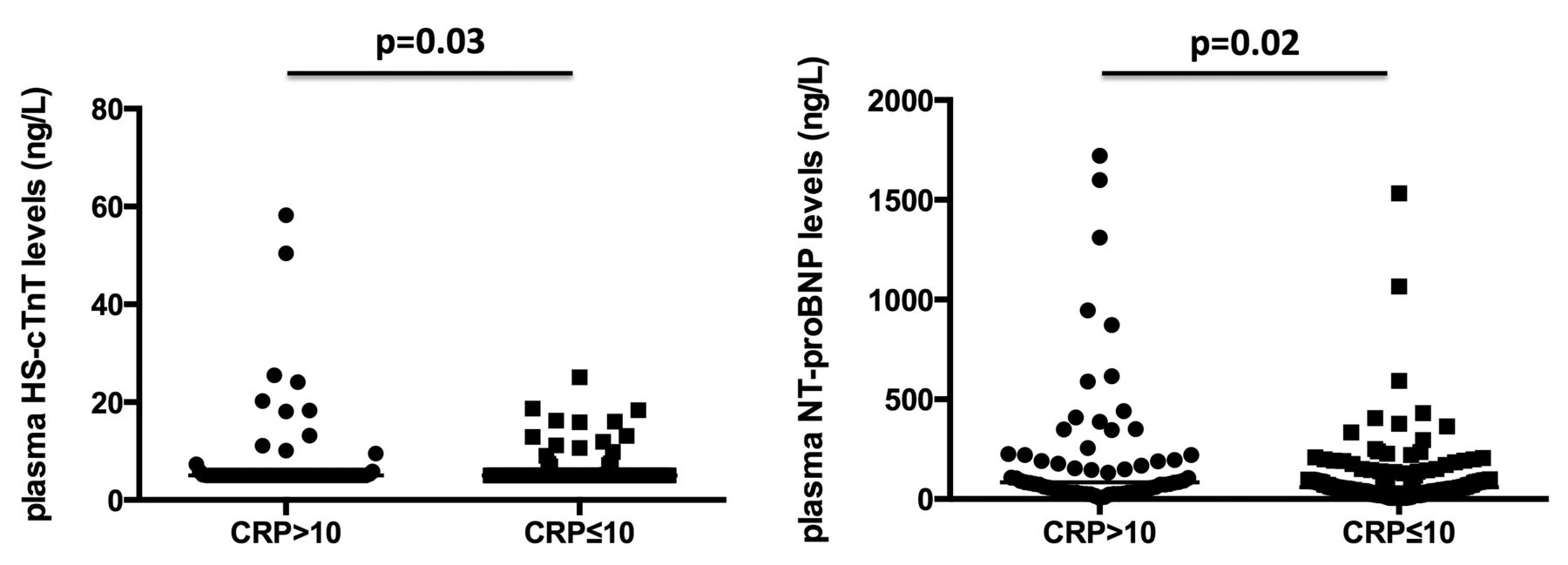
Median plasma levels of high-sensitivity cardiac troponin (HS-cTnT; A) and N-terminal pro-brain natriuretic peptide (NT-proBNP; B) levels according to C-reactive protein (CRP) concentrations.
- Accepted for publication September 17, 2013.








{kind=link}
{kind=link}
{kind=link}
{kind=link}