

To the Editor:
Systemic sclerosis (SSc)-associated interstitial lung disease (ILD) affects 40% of patients with SSc and leads to reduced survival, even with mild disease1. Among patients with SSc-ILD, reductions in forced vital capacity (FVC) and DLCO predict mortality, with threshold percent-predicted FVC values of < 70%2,3 and < 55%4, and DLCO values ≤ 60%5 and ≤ 70%6 identified as predictors of poor outcome. We sought to assess for threshold values of baseline FVC and DLCO that are associated with survival in SSc-ILD.
Our study was approved by the University Health Network (REB number 11-0001-AE) and Mount Sinai Hospital (REB number 11-0003-C) research ethics boards, with requirement for informed consent waived. Adult patients were identified from our Scleroderma and ILD clinics (1983–2012) if they fulfilled the American College of Rheumatology (ACR) classification criteria for SSc7 and had findings of ILD on thoracic computerized tomography. Pulmonary function tests (PFT) were routinely performed. The primary outcome was death or lung transplantation (last determined May 2012) from clinic or hospital records, or obituary8. Survival was defined as time from ILD diagnosis to death/transplantation, right censored from last known-alive date (or at latest May 2012). Median survival was estimated using Kaplan-Meier curves and compared with the log-rank test. Cox proportional hazards models were used to estimate HR, 95% CI, and p values. We fitted bivariate and multivariate models, the latter in a forward stepwise manner. We explored plots of standardized log-rank statistic values versus FVC and DLCO percent-predicted. We assumed that PFT values that maximize the standardized log-rank statistics are most discriminatory, and may provide clinically useful predictive values of FVC and DLCO9. Analyses were performed using STATA (Stata statistical software, Release 6.0, 1999, Stata Corp.), R Studio version 0.96.331 (The R Foundation for Statistical Computing), and SAS 9.2 (SAS Institute Inc.).
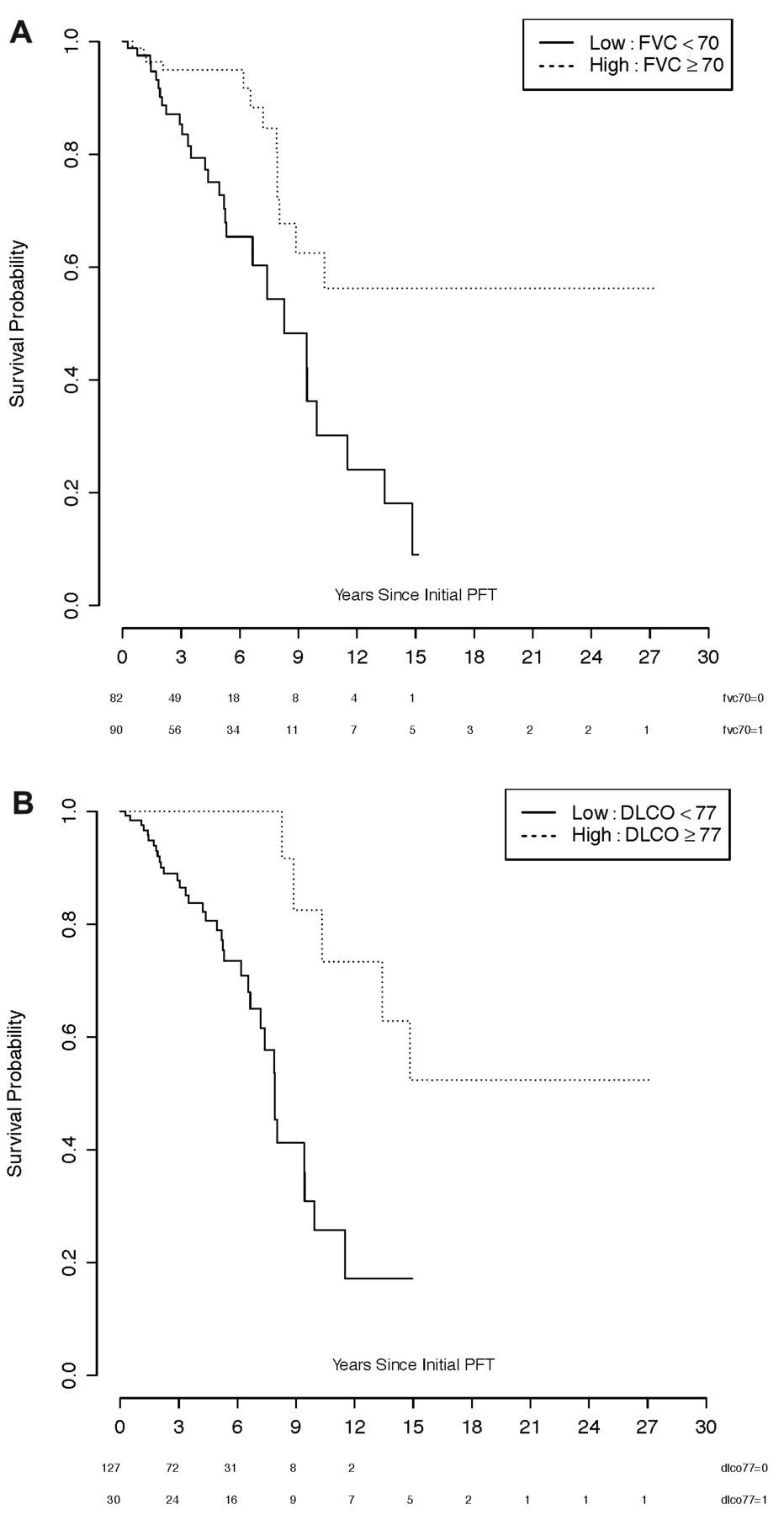
We identified 188 patients with SSc-ILD, and included 172 patients with available PFT and longitudinal followup (Table 1). In addition to the inclusion criteria7, all patients also met the 2013 ACR-European League Against Rheumatism classification criteria for SSc10. The median time from diagnosis of SSc to initial FVC was 4 years. Forty-two patients (24%) experienced death or lung transplant [37 died (22%), and 5 underwent lung transplant (3%)]. Unadjusted survival analysis found that FVC (HR 0.96, p < 0.001), DLCO (HR 0.96, p < 0.0001), baseline pulmonary hypertension (HR 3.84, p = 0.02), and immunosuppressive treatment (HR 2.45, p = 0.02) were all statistically significant (Table 1). In adjusted analysis, FVC (HR 0.97, p = 0.0009), DLCO (HR 0.97, p = 0.0004), and increasing age (HR 1.03, p = 0.04) remained significant (Table 1). Standardized log-rank statistic plots were not unimodal, and thus did not identify optimal PFT predictive thresholds clearly. However, we selected the tallest peaks of the plots as the preferred predictive thresholds. An FVC of 70% (p = 0.0007; Figure 1) and a DLCO of 77% (p = 0.0005; Figure 1) maximized the respective standardized log-rank statistics, and maximally discriminated between patients according to our outcome (survival or transplant).

Kaplan-Meier survival curves comparing survival stratified by initial (a) FVC 70% predicted, showing longer survival in patients with FVC ≥ 70% predicted (p = 0.0007), and (b) DLCO 77% predicted, showing longer survival in patients with DLCO ≥ 77% predicted (p = 0.0005). Numbers of patients at risk are presented beneath time axis. FVC: forced vital capacity.
Clinical data and Cox proportional hazards survival analysis for death or lung transplantation in patients with SSc-associated interstitial lung disease. HR calculated for combined endpoint of death or lung transplant; per unit increase of the variable for continuous variables. Variables use measurements at initial observation in predictive models.
Baseline FVC and DLCO were strongly associated with survival. A threshold of 70% predicted FVC and 77% predicted DLCO appeared to maximally discriminate among patients by survival. However, nearly equivalent thresholds appeared for both FVC and DLCO (about 80% and 65% predicted, respectively). Our results are consistent with prior studies. Among patients with SSc, regardless of the presence of ILD, FVC thresholds of 80%5 and 70%2,3 have been identified as poor prognostic markers3,5. Our observation, based on standardized log-rank statistic plots, that an FVC of 80% may represent a nearly equivalent discriminative threshold (compared with 70%) is intriguing. Perhaps clinicians should take note of even mildly reduced FVC values, in that even a small reduction from expected baseline lung function may be an important finding to be carefully considered in patient management.
We estimated that a DLCO < 77% appeared to be most discriminative regarding mortality in our cohort. This high value should be interpreted with caution, in that we identified a fairly similar threshold at a much lower initial DLCO of about 65% predicted. DLCO thresholds of ≤ 60%5 and ≤ 70%6 have been previously identified in studies including patients with SSc regardless of the presence of ILD. Surprisingly, pulmonary hypertension did not persist as a statistically significant predictor in our multivariate model, perhaps because of our definition (right ventricular systolic pressure > 35 mmHg, and/or right ventricular dilatation or dysfunction on echocardiogram), which was not ideal, but selected based on data availability. Alternatively, perhaps DLCO, a marker of both interstitial and pulmonary vascular disease, outperformed pulmonary hypertension as a risk factor. Despite limitations in our study (retrospective design, limitations of available data including pulmonary hypertension definition, and drug treatment over time), our results support the idea that FVC and DLCO are strong and consistent predictors of survival in SSc-ILD. There is uncertainty around optimal thresholds, but perhaps even small reductions from “normal” PFT values are important predictors in patients with SSc-ILD.
Footnotes
-
Dr. Johnson is supported by a Canadian Institutes of Health Research Clinician Scientist Award, the Freda Feier Fund, and the Norton Evans Fund for Scleroderma Research.








{kind=link}