

Abstract
Objective. To develop/validate an instrument to measure health-related quality of life (HRQoL) in patients with psoriatic arthritis (PsA), for use in clinical studies.
Methods. An item pool of 35 items was generated following standardized procedures. Item reduction was performed using clinimetric and psychometric approaches after administration to 66 patients with PsA. The resulting instrument, the VITACORA-19, consists of 19 items. Its validity content, internal consistency, test-retest reliability, known groups/convergent validity, and sensitivity to change were tested in a longitudinal and multicenter study conducted in 10 hospitals in Spain, with 323 patients who also completed the EuroQol 5-dimensional questionnaire (EQ-5D) and a health status transition item. There were 3 study groups: group A (n = 209, patients with PsA), group B (n = 71, patients with arthritis without psoriatic aspect, patients with arthrosis, and patients with dermatitis), and group C (n = 43, healthy controls).
Results. The questionnaire was considered easy/very easy to answer by 94.7% of the patients with PsA. The factorial analysis clearly identified only 1 factor. Cronbach’s alpha coefficient and interclass correlation coefficients exceeded 0.90. Statistically significant differences (p < 0.001) were observed between groups: subjects from group C had better HRQoL, followed by group B, and finally group A had the worst HRQoL. The VITACORA-19 scores showed significant correlations (p < 0.001) to PsA disease activity, EQ-5D, and perceived health state, scoring the patients with better health state higher. The minimum important difference was established as an 8-point change in the global score.
Conclusion. The Spanish-developed VITACORA-19, designed to measure HRQoL in patients with PsA, has good validity, reliability, and sensitivity to change.
Psoriatic arthritis (PsA) has been defined as a unique type of inflammatory peripheral and/or axial arthritis that is associated with skin psoriasis1,2. Its exact prevalence is unknown, but studies suggest that PsA occurs in 30% of patients with psoriasis3,4,5. PsA imposes a considerable economic and human burden, and has a substantial effect on patients’ health-related quality of life (HRQoL) and functioning6,7,8,9,10.
HRQoL is an important indicator of the burden of musculoskeletal disease and is usually defined as a multidimensional concept encompassing the physical, mental, and social components associated with an illness or its treatment11. That is, HRQoL is the subjective perspective of functioning, as is defined by the World Health Organization12,13. Generic instruments have traditionally been used to measure HRQoL, but studies have shown that correlation between clinical assessments and subjective generic measurement like HRQoL is poor14.
An attempt to overcome this gap was the development of specific HRQoL instruments. Only 1 disease-specific instrument has been developed to evaluate HRQoL in patients with PsA to date15 — the PsAQoL. That questionnaire is not validated in the Spanish population nor is there any other specific questionnaire for arthritis validated in this population.
Because the PsAQoL presents some limitations, instead of adapting it into Spanish, the aim of our present study was to develop a new instrument. It would be suitable for use in clinical studies.
MATERIALS AND METHODS
The new questionnaire was developed and validated following a standardized procedure. The process consisted of 2 main phases: (1) item generation, item reduction, and questionnaire development (pilot study); and (2) validation of the final version of the questionnaire (validation study).
Item generation, item reduction, and questionnaire development
Questionnaire content was developed from a literature review, consultations with clinical experts and experts in the development and use of patient-reported outcomes measures, and focus groups of patients with PsA. A comprehensive review of the scientific literature was conducted to identify instruments already developed to measure the PsA HRQoL and to identify issues of relevance in the construction of the new instrument. There were 7 focus groups of patients with PsA, and a semistructured script was used to guide discussions. Focus groups included 5 to 7 patients, and the most relevant statements obtained from those interviews were used to prepare the questionnaire.
To identify items for inclusion in the final version of the questionnaire, the items in the item pool were administered to a sample of patients with PsA in an observational, cross-sectional, multicenter study (pilot study). Analysis of missing responses and response distribution were included to reduce the number of items. In addition, using the responses collected, an item analysis was performed following a strategy based on Classic Test Theory (CTT)16 and the Rasch analysis17,18 to reduce the size of the instrument. The CTT presupposes, then one can directly infer, e.g., the quality of life of a patient with PsA by summing up the responses and calculating a total score, assuming that each item contributes equally to this total score. In contrast, the Rasch model provides an alternative scaling methodology that enables the examination of the hierarchical structure and the unidimensionality and additivity of HRQoL measures. The Rasch analysis constructs a line of measurement, with the items placed hierarchically, and provides a statistical adjustment indicating to what degree an item describes the group of subjects responding to the questionnaire.
The chi-squares in common use are known as OUTFIT and INFIT. These are reported as mean-squares (chi-square statistics divided by their degree of freedom), so that they have a ratio-scale form with expectation 1 and range 0 to +infinity. INFIT and OUTFIT MNSQ indices > 1.3 or < 0.7, respectively, were eliminated. Successive Rasch analyses were performed until a final set of items satisfied the model fit requirement. Additionally, those items with a separation below 1 were eliminated. Internal consistency coefficients (Cronbach’s alpha) were obtained for the overall scale as an expression of reliability.
Each item allows for 5 Likert-like response choices from “always” to “never”, and the referred time period is the previous week. Score for the overall questionnaire is obtained by adding the responses to the corresponding items, with subsequent standardization to a scale ranging from 0 (worst HRQoL) to 100 (best HRQoL). Standardization is obtained as follows:

The final Spanish version of the questionnaire is called VITACORA-19 (Appendix 1).
Questionnaire validation
To validate the VITACORA-19 questionnaire, a multicenter, observational, prospective study was conducted from January 2010 to September 2010 at the rheumatologic departments of 10 Spanish hospitals.
There were 3 study groups defined based on health condition. Group A included patients who were diagnosed with PsA according to the Moll and Wright criteria19. Two clinical subsets were used: peripheral PsA and axial PsA20. The distinction was made by each treating rheumatologist according to their clinical judgment. Group B included patients with arthritis, but not the psoriatic type (rheumatoid arthritis, ankylosing spondylitis, and undifferentiated arthritis), patients with arthrosis (any type), and patients with dermatitis (any type). Finally, Group C comprised healthy controls.
Our study aimed to include a total of 389 subjects. Each center participating consecutively included ambulatory patients aged more than 18 years, and all subjects provided informed consent to participate. The project was approved by the Ethics Committee at La Princesa Hospital in Madrid, Spain.
Sample size
The sample size was calculated for each study group. On the one hand, patients in group A (patients with PsA) were included to allow both assessment of the sensitivity to change and test-retest reliability of the questionnaire. The sample size required to assess the sensitivity to change was selected to guarantee an 80% statistical power to detect an effect size change (i.e., difference/SD) of 0.2, considered of small magnitude21, with significance level. Assuming 10% of patients would be lost to followup or not evaluable, the sample size calculated for this group was 198 patients. The sample size required to assess the test-retest reliability was observed to obtain an interclass correlation coefficient (ICC) of 0.7 or higher, assuming a minimum ratio of 0.5. With identical statistical criteria, 1 additional sample size of 63 patients with PsA was required.
For group B, a ratio of 1 control for every 5 patients with PsA was estimated. A sample size of 78 patients was required to detect an effect size of 0.4 or higher with a 5% 2-sided significance level of 0.05 and a statistical power of 0.80.
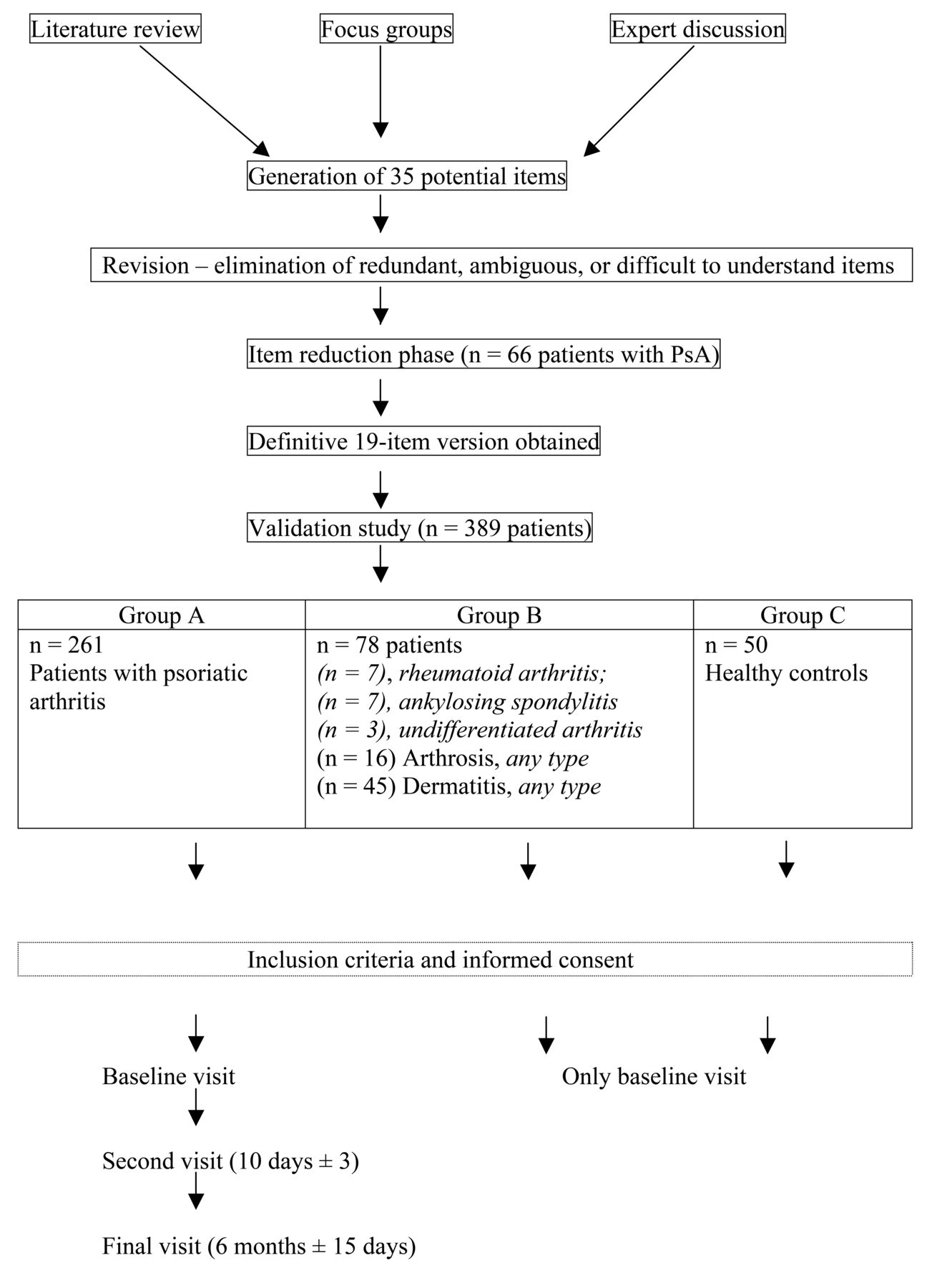
Group C, a sample of healthy controls, comprised 50 healthy subjects. Figure 1 shows the study design and the size of the groups.

Development and validation process for the VITACORA-19 questionnaire. PsA: psoriatic arthritis.
Study measurements
All patients with PsA recruited into the study (group A) attended 3 visits: a baseline visit, a second visit at 10 days, and a final visit at 6 months. The patients in groups B and C attended only the baseline visit.
At the baseline visit, the following were recorded: sociodemographic data, clinical subsets of PsA, time since diagnosis, and PsA activity assessments [C-reactive protein, erythrocyte sedimentation rate (ESR), body surface area (BSA), Bath Ankylosing Spondylitis Function Index (BASFI), Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), and the 28-joint Disease Activity Score (DAS28)]. At the final visit, the same variables were recorded, except for sociodemographic characteristics. At each visit, study participants completed the specific VITACORA-19 questionnaire, the Spanish EuroQol 5-dimensional (EQ-5D) questionnaire22, and the visual analog scale (VAS) of the EQ-5D, and they were asked about their perceived general health using a Likert scale with 7 response options (from “very good” to “very poor”). Patients and clinicians were also asked to estimate the PsA global activity, and 1 additional item pertains to health state transition.
Statistical method
A descriptive, comparative analysis of the sociodemographic and clinical characteristics of groups A, B, and C study participants was performed. For group comparison, ANOVA test with the Bonferroni correction was used for multiple comparisons of continuous variables, and a chi-square test was used for categorical variables. Changes in PsA activity variables and overall scores from baseline to the final visit were also compared in the different study groups using the same statistical tests. The questionnaire’s feasibility was assessed through the ease-of-use question. The distribution of the overall scores was analyzed by calculating mean scores, SD, observed score ranges, and floor and ceiling effects.
The unidimensionality of the VITACORA-19 questionnaire was explored through examination of the residual correlation of a one-factor exploratory factor analysis of the items to determine whether the new instrument could be reduced to a unique summary score. A unidimensional questionnaire is one that measures only 1 concept (dimension, construct), e.g., disability (or its inverse, function).
The instrument’s internal consistency was assessed by estimating Cronbach’s alpha coefficient for the overall score at baseline. An alpha value of 0.70 or above is necessary to call a scale internally consistent16. The 10-day test-retest reliability was assessed by calculating the ICC between visits in patients who did not report any significant change on the health status transition item23.
Known-groups validity was tested by comparing the questionnaire scores of the different study groups, using an ANOVA test. Because they could have both skin lesions and joint disease, the patients with PsA were expected to report HRQoL worse than that of patients with psoriasis, or patients with arthritis without psoriasis, or those with arthrosis or dermatitis, or healthy controls. The statistically significant differences between study groups were confirmed using a regression model that adjusted by sociodemographic characteristic differences.
To assess convergent validity, the relationship between the scores in the VITACORA-19 and scores obtained in the descriptive system of the EQ-5D was analyzed at baseline using an ANOVA test or no parametric test of Kruskal-Wallis, and the correlation between the scores in the VITACORA-19 and the scores obtained in the VAS of the EQ-5D was analyzed using Pearson’s correlation coefficient. Patients with PsA were included in this analysis. Scores obtained in the questionnaire were analyzed based on the presence of problems in the items of the descriptive system of the EQ-5D questionnaire using a Student’s t test.
To assess longitudinal validity, changes seen in scores in the VITACORA-19 questionnaire from the baseline to the final visit were compared to the changes seen in PsA activity assessments during the same time period. For this, a Student’s t test, an ANOVA test, and the Pearson’s correlation coefficient were used depending on the type of variable analyzed.
Finally, to assess sensitivity to change, the effect size obtained in VITACORA-19 was calculated. The minimal clinically important difference (MCID) of the questionnaire was estimated as the difference seen by patients who stated that their health status had a “small improvement” at 6 months after study start. Effect size values of about 0.2 were considered to represent a small change, values of about 0.5 a moderate change, and values of about 0.8 or higher a large change21.
A significance level of 0.05 was considered for all group comparisons.
RESULTS
Item generation, item reduction, and questionnaire formatting
The literature review identified only 1 instrument to measure HRQoL in patients with PsA; it was not validated in the Spanish language. Recommendations from the expert consensus meeting concerning the characteristics of the new questionnaire included that it should contain basic symptoms and be self-administered and easy to score. The focus group sessions included 66 patients with PsA and generated an initial item pool of 35 items. The pilot test reduced the number of items to 19 and gave a preliminary indication of the good measurement properties of the questionnaire.
Validation of the VITACORA-19 questionnaire
The new questionnaire was considered easy or very easy to answer by 94.7% of 323 patients with PsA. Using the whole Rasch reduced version, the unidimensionality of the questionnaire was explored and only 1 principal component was identified that accounted for most of the observed variance (55.8%). Evaluable responses were available for a total of 323 patients at the first visit.
Table 1 provides the baseline characteristics and health of study participants. Patients in group A had a slightly higher mean age (48.7 yrs) than subjects in the 2 other groups (46.5 yrs in group B and 42 yrs in group C, p < 0.001). The table also includes patient-reported information about health status at the baseline in the groups under study. Worsening functional status, perceived health state, and HRQoL were reported by the group of patients with PsA compared with the other groups. Clinical features comparison between group A and group B shows the same time from diagnosis (8 yrs), and a similar percentage of comorbidities. BSA and scores for BASDAI and DAS28 were measured only in group A.
Baseline characteristics and health of the study participants (n = 323). Group A: patients with PsA. Group B: patients with arthritis and no psoriatic—any type of arthrosis—any type of dermatitis. Group C: healthy controls.
Table 2 shows the score distributions, floor and ceiling effects, internal consistency, and test-retest reliability coefficient for the questionnaire. Floor and ceiling effects were less than 2% for the overall score. Cronbach’s alpha value and the ICC value for the overall score exceeded 0.90. The 10-day test-retest reliability was assessed in a subgroup of patients who did not report any significant change on the health status transition item (n = 97).
Score distributions, floor and ceiling effects, internal consistency, and test-retest reliability of the VITACORA-19 questionnaire.
Table 3 shows the results of testing the known groups’ validity of the VITACORA-19 questionnaire. Statistically very significant differences (p < 0.001) were observed among the groups: subjects from group C (healthy controls; mean overall score 93.7, SD 9.1) had a better HRQoL, followed by group B (patients with arthritis but not PsA, and those with arthrosis or dermatitis; mean overall score 69.2, SD 24.8), and finally group A (PsA; mean overall score 56.2, SD 24.8), which had the worst HRQoL. No significant differences were found between PsA clinical subsets (axial vs peripheral) or oligoarthritis versus polyarthritis. On the contrary, statistically significant differences were found between patients with PsA and patients with psoriasis (group B control, p < 0.05). Patients with psoriasis had higher HRQoL scores than did patients with PsA. In patients with PsA with different disease activity, as measured by DAS28, significant differences were found (p < 0.001) among groups using the accepted cutoff value of remission (better HRQoL), moderate activity, and high activity (worse HRQoL). When VITACORA-19 global score was analyzed according to the level of problems in each of the EQ-5D dimensions and to patient/clinician perceived health state, significant differences were found (p < 0.001).
Known-groups validity of VITACORA-19 questionnaire according to groups under study, to subset/clinical/activity features, and to EQ-5D and health state perception scores of patients with PsA at baseline (n = 209). Values given are means ± SD. Higher scores signify better HRQoL. Range from 0 to 100.
Table 4 shows the results of testing convergent validity of the VITACORA-19. The highest correlation coefficients were the relationships for ESR, DAS28, EQ-5D VAS, and for the estimation of PsA global activity according to patients and physicians.
Convergent validity of VITACORA-19 overall score with EQ-5D VAS, PsA activity assessments, axial night pain intensity, and PsA global activity estimation by clinician and patients.
Finally, Table 5 shows the results of testing the sensitivity to change of the VITACORA-19 questionnaire among patients reporting at least a small improvement in health state (n = 73). Effect sizes for the global score changes between 2 study visits among patients with PsA ranged from 0.20 to 0.80. The MCID was established as an 8-point change in the global VITACORA-19 score.
Sensitivity to change over time of the VITACORA-19 questionnaire among patients with PsA according to perceived health state changes.
DISCUSSION
Our present study has described the development of a new specific questionnaire designed to assess HRQoL in patients with PsA. This kind of patient-reported outcome is an attractive option in a busy medical practice24. The idea of developing a specific questionnaire based on systematic methodology arose from the scarce number in the literature of PsA HRQoL instruments and their limitations.
Only 1 disease-specific instrument (PsAQoL) has been developed to date to evaluate HRQoL in patients with PsA, using the needs-based model15. We decided not to adapt this questionnaire into Spanish because it does not take into account basic symptoms in these patients nor repercussions of the dermatological process on the HRQoL. Thus, we felt the need to develop a new instrument, considering the HRQoL as a multidimensional construct and keeping in mind the Wilson and Cleary-integrated HRQoL model for health outcomes14,25,26. In the VITACORA-19 validation process, we have seen that basic symptoms in patients with PsA (swelling or pain) and psychosocial aspects of the dermatological disease (sense of shame or social rejection) affect HRQoL. Therefore, several items of the questionnaire are related to these PsA-specific problems.
The VITACORA consists of only 19 items and has proven quick and easy to complete. It is thus considered suitable for use in standard clinical practice.
The development of the VITACORA-19 followed recommended guidelines27,28, and a considerable effort was made to include the point of view of the clinicians/patients from different parts of Spain, and to ensure that the sample was reasonably geographically representative. Although content validity evaluations tend to be fairly subjective, the rational basis, the comparison with existing standards, expert opinions, and the inclusion of focus groups of patients with PsA in the development process of the questionnaire ensured the new instrument’s content validity. The fact that only 1 component/dimension was obtained in the inspection of the residual correlation of 1-factor exploratory factor analysis suggests the instrument’s unidimensionality and supports the use of the summary scores.
The VITACORA-19 shows good psychometric characteristics, and meets accepted criteria for use in clinical studies27,28,29. Floor and ceiling effects were within acceptable limit30. The instrument also shows good internal consistency for the overall score and meets the recommended level of 0.7 for use at group level27,28,29. The Cronbach’s alpha value (0.95) is sufficient to permit its use at individual level16. Test-retest reliability results were positive; they are higher than the recommended threshold of 0.70.
The analysis of known groups’ validity showed that the VITACORA-19 questionnaire discriminated well between groups under study. Likewise, it has discriminated well between PsA clinical subsets, between patients with PsA and patients with psoriasis, and according to different disease activity levels. These findings are coherent with our previous hypothesis and coincide with reports by other authors6. Significant differences between patients with PsA and the general population have been shown9,31,32,33; it causes as much disability as do other major diseases34.
As expected, a higher level of problems in each of the EQ-5D variables corresponds to a lower HRQoL global score in the VITACORA-19 questionnaire. The high percentage of patients with PsA with anxiety/depression and pain/discomfort can explain the high PsA HRQoL deterioration because these symptoms are important correlates of HRQoL. Kotsis, et al have described a correlation in this sense35, and a consequential and bidirectional relationship has been seen between depressive symptoms and pain36. Reinforcing this hypothesis, patients with PsA reported greater role limitations attributable to emotional problems and more bodily pain than did patients with other inflammatory arthritis, such as rheumatoid arthritis37. Although this last fact can be supposed from our findings, attributable to a low number of patients with arthritis within group B, further investigation is needed to establish that HRQoL in patients with PsA is worse than in other types of arthritis as measured by the VITACORA-19 questionnaire.
The psychological and social effects of skin involvement have been well documented in patients with psoriasis38,39, and dimensions typically affected by PsA were mental health and social functioning33. Khraishi, et al reported that patients who had PsA for longer than 2 years had rates of depression 2 to 5 times higher than those of age-matched controls who had no history of PsA or psoriasis40. The extent of disability and the effect on physical and mental HRQoL is possibly related to the psoriatic skin lesions and peripheral and/or axial joint disease33,41 that these patients have. These statements correspond to our findings.
The correlations revealed a moderate relationship between VITACORA-19 global score with EQ-5D VAS, BASFI, and DAS28, and a weak relationship with the BSA, in line with similar results shown by the other PsA-specific HRQoL instrument42. Significant correlations between VITACORA-19 overall score and perceived health state by patient/clinician indicated that patients with better health state reported higher HRQoL.
At followup, no significant correlations were found between VITACORA-19 overall score changes and PsA clinical assessment changes. Usually, no correlations values higher than 0.7 were reported43. This indicates that the clinical HRQoL-specific assessments should be considered not as overlapping but as complementary.
Finally, the instrument appears to be sensitive to changes in patients’ health status. Effect sizes for the global score changes showed an improvement in health status. This helps determine the longitudinal validity of the instrument. The MCID was established as an 8-point change in the global VITACORA-19 score, useful in the interpretation of scores in the clinical practice.
A criticism of disease-specific measures is that they do not allow comparisons to be made across diseases and cultures. Taking this into account44,45, an English version of VITACORA-19 is being developed following the recommended guidelines46. Further studies should concentrate on both testing the VITACORA-19 with current measures of PsA comorbidity and linking its content to The International Classification of Functioning, Disability and Health47,48 as an authorized external reference of what to measure49.
Our study permitted the evaluation of the measurement properties of this new instrument, which has been designed to measure the PsA HRQoL and has shown good reliability, validity, and responsiveness.
Acknowledgment
We thank the members of the Vitacora Group: Dermatology: Rosa Izu Belloso (H. de Basurto de Bilbao); Carlos Muñoz Santos (H. Clínic i Provincial de Barcelona); Vicente Oliver Martínez (H. Gral. U. de Valencia); José Manuel Hernanz (H. Infanta Leonor); Yeray Peñate (H. Insular de Gran Canaria); Victoria Mendiola Fernández (H. Virgen de la Victoria); Mariano Ara Martín (H. Clínico U. Lozano Blesa); Isabel Belinchón Romero (H. Gral. de Alicante). Rheumatology: Santiago Muñoz (H. Infanta Sofía de Madrid); Ángel García Aparicio (H. Virgen de la Salud); Rafael Ariza (H. Virgen Macarena de Sevilla); Carlos González Fernández (H. Gregorio Marañón de Madrid); Carlos García Porrua (H. Xeral Calde de Lugo); Luis González Puig (H. La Fe Valencia); J.L. Peña Sagredo (H. Marqués de Valdecilla de Santander); Antonio José Lozano Sáez (H. de La Plana); Alberto Bermúdez Torrente (H. U. Virgen de la Arrixaca de Murcia); Antonio Mera Varela (H. Clínico U. de Santiago); Luz García Vivar (H. de Basurto de Bilbao); José Miguel Ruiz Martín (H. de Viladecans); Héctor Corominas Macias (H. de St. Joan Despí Moisès Broggi); Xavi Juanola Roura (H Bellvitge de Barcelona); Esther Rincón (H. San Pedro de Alcántara); Jesús Alberto García Vadillo (H.U. La Princesa de Madrid); Raúl Veiga (H. de Fuenlabrada); Roberto Miguélez Sánchez (H. Móstoles. Madrid); Lucía Pantoja Zarza (H. El Bierzo de León); Alexia de Juanes Montmeterme (H. 12 de Octubre de Madrid); Juan Miguel Sánchez Bursón (Complejo Hospitalario Virgen de Valme, Sevilla).
APPENDIX 1.
Validated version of the VITACORA-19 questionnaire. The following statements refer to how signs and symptoms of psoriatic arthritis could affect your daily life. Your answers will help us to determine your health status, and how your illness affected your ability to perform your daily activities during the last week. There are 5 possible answers following each statement. Please read each statement carefully, answering every question. In case you are not confident, please choose the answer that fits to your reality more accurately. Answers are neither correct nor incorrect. We are just interested in how your illness affects your daily life.
During the last week, because of your psoriatic arthritis…
Footnotes
-
Supported in part by a grant from Pfizer for the Investigator Initiated Research project “Development and validation of a new instrument to assess health related quality of life in psoriasis arthritis: the Vitacora-19 questionnaire.”
- Accepted for publication June 13, 2014.








{kind=link}